(UroToday.com) The 2025 ESMO annual meeting featured a urothelial carcinoma mini oral session and a discussant presentation by Dr. Shilpa Gupta discussing three abstracts “Health-related quality of life outcomes from the NIAGARA trial of perioperative durvalumab plus neoadjuvant chemotherapy in muscle invasive bladder cancer” by Dr. Michiel Van der Heijden, “Phase 1 study of LY3866288, a potent, highly isoform-selective FGFR3 inhibitor in FGFR3-altered advanced solid tumors (FORAGER-1): Dose optimization” by Dr. Alexandra Drakaki, and “Datopotamab deruxtecan + rilvegostomig in patients with locally advanced or metastatic urothelial cancer: Results from the phase 2 TROPION-PanTumor03 study” by Dr. Sun Young Rha.
Dr. Gupta started by discussing NIAGARA and highlighting that there are several factors affecting a cancer patient’s quality of life, including patient-related factors, disease-related factors, psychological factors, treatment-related factors, and socioeconomic/cultural/environmental factors:

The goal of effective cancer treatments is to help patients live longer and improve/maintain their quality of life. Thus, patient-reported outcome assessments in clinical trials is crucial for patient-centric evaluation.
In NIAGARA,1 cisplatin-eligible patients with muscle invasive bladder cancer (cT2-T4aN0/1M0) planned for radical cystectomy were randomized 1:1 to 4 cycles of neoadjuvant durvalumab (1500 mg IV every 3 weeks) + neoadjuvant chemotherapy (cisplatin + gemcitabine IV every 3 weeks) followed by radical cystectomy then 8 cycles of adjuvant durvalumab monotherapy (1500 mg IV every 4 weeks) (durvalumab arm) or neoadjuvant chemotherapy followed by radical cystectomy alone (comparator arm):
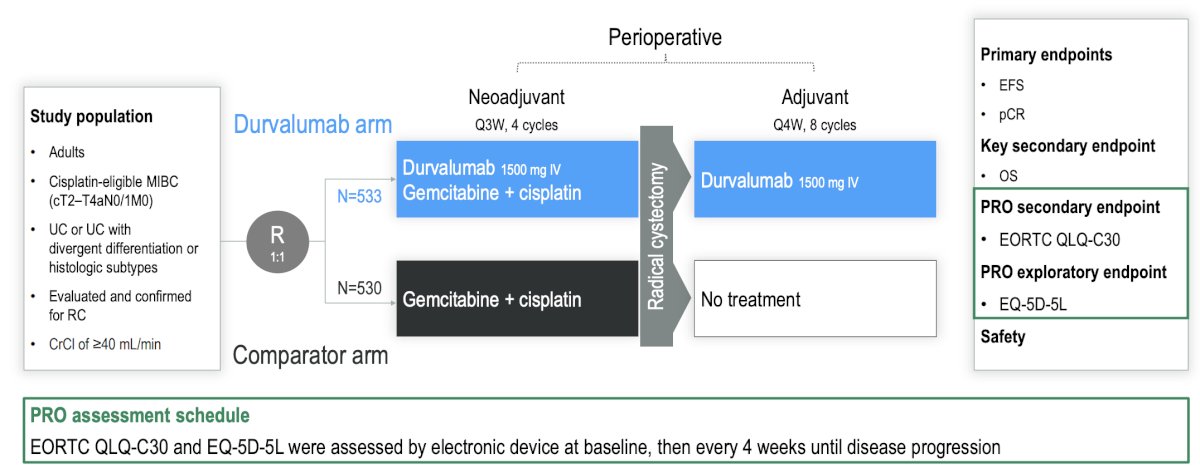
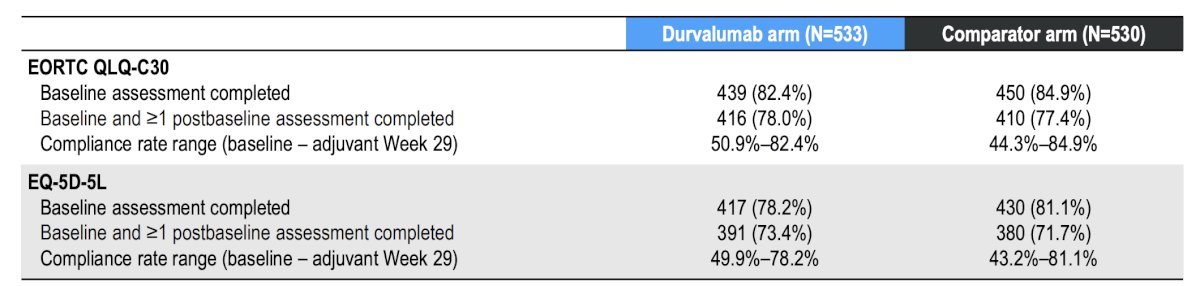
Health-related quality of life was measured using the EORTC QLQ-C30 as a secondary endpoint. Global health status/quality of life, physical functioning, fatigue, and pain were the prespecified priority subscales. Change from baseline and time to definitive deterioration were all assessed. Additionally, health-related quality of life per the EQ-5D-5L visual analog scale was an exploratory endpoint. QLQ-C30 baseline compliance was ≥82% in both arms, and mean baseline scores were similar between arms:
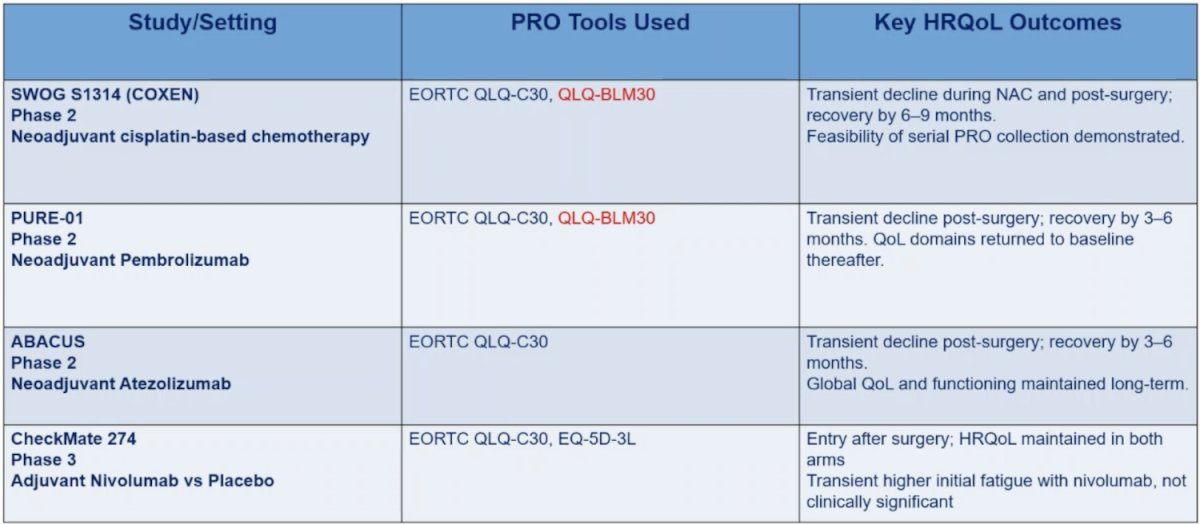
The following table highlights the health-related quality of life evidence from neoadjuvant and adjuvant trials in muscle-invasive bladder cancer trials, pre-NIAGARA:
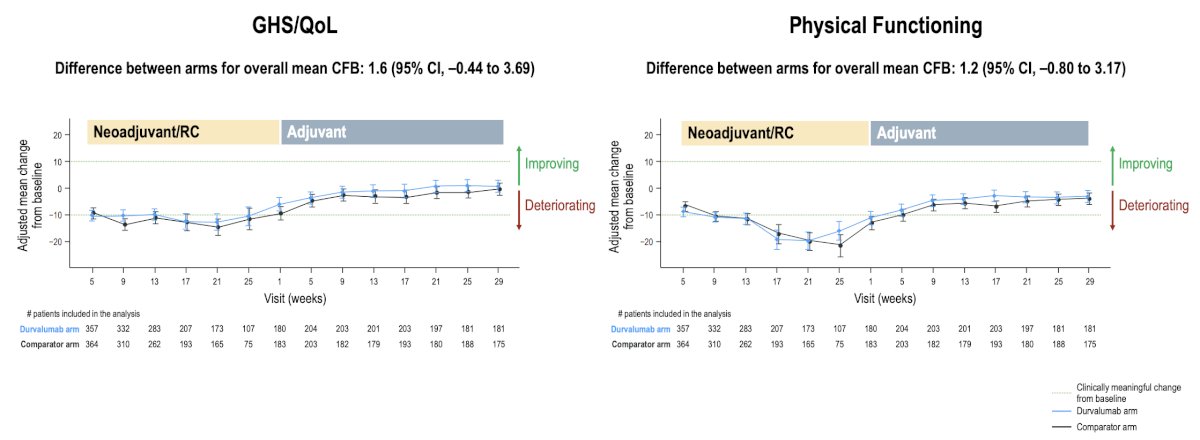
The addition of perioperative durvalumab to neoadjuvant chemotherapy did not adversely impact global health status/quality of life (difference between arms for overall mean CFB: 1.6, 95% CI -0.44 to 3.69), or physical functioning subscale scores (difference between arms for overall mean CFB: 1.2, 95% CI -0.80 to 3.17):
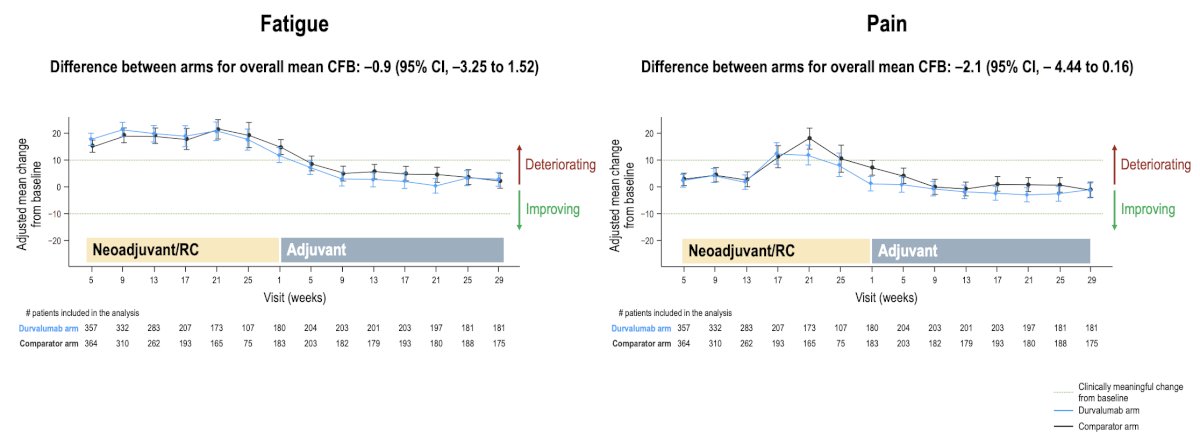
Furthermore, the addition of perioperative durvalumab to neoadjuvant chemotherapy did not adversely impact fatigue (difference between arms for overall mean CFB: -0.9, 95% CI -3.25 to 1.52) or pain subscale scores difference between arms for overall mean CFB: -2.1, 95% CI -4.44 to 0.16):
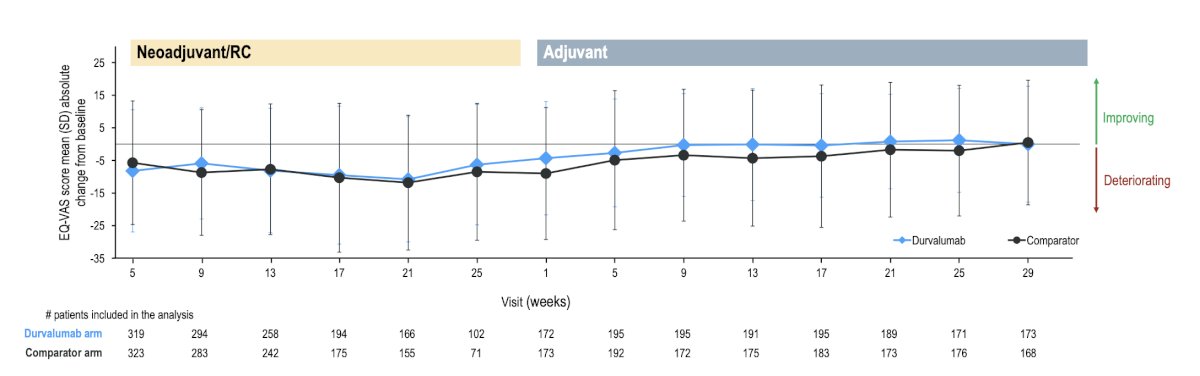
The addition of perioperative durvalumab to neoadjuvant chemotherapy did not adversely impact the EQ-visual analog scale score. The mean baseline EQ-visual analog scale score was 77.3 (SD 15.9) in the durvalumab arm and 74.9 (SD 16.9) in the comparator arm:
Dr. Gupta concluded her assessment of the NIAGARA trial quality of life outcomes, with the following takeaway points:
- NIAGARA, the first and largest perioperative phase 3 trial in muscle-invasive bladder cancer, demonstrated that perioperative durvalumab did not worsen health-related quality of life; transient changes reflected surgical recovery rather than treatment effect
- Overall health-related quality of life remained stable across domains, with comparable outcomes between arms, supporting the tolerability of perioperative immunotherapy in muscle-invasive bladder cancer
- There are several remaining unmet needs:
- Develop contemporary patient-reported outcome tools to capture the unique toxicities of modern therapies
- Harmonize patient-reported outcome assessment across trials and elevate beyond exploratory endpoints to inform regulatory and clinical decisions
- Incorporate digital technologies — including wearable devices and artificial intelligence-based analytics — to track real-world recovery and minimize survey fatigue
Dr. Gupta then discussed the FORAGER-1 phase 1 trial. First-generation FGFR inhibitors (ie, erdafitinib) are non-specific, have multiple off-target toxicities, and have early resistance. The next generation selective FGFR3 inhibitors include (i) vepugratinib: high specificity, improved tolerability, and broader resistance coverage N540K, V553L, etc (non-gatekeeper mutations); (ii) dabogratinib: high specificity, improved tolerability, broader resistance coverage including gatekeeper mutations.
In FORAGER-1, the 200 mg BID dose of vepugratinib was optimal in terms of efficacy and tolerability in a heavily pre-treated metastatic urothelial carcinoma population, including 24% with prior FGFR inhibitor exposure and >60% with enfortumab vedotin exposure (alone or with enfortumab vedotin + pembrolizumab). The objective response rate was 34%, with 50% (6/12) remaining on treatment at a median of 8 months.
For vepugratinib + enfortumab vedotin + pembrolizumab, is this translational rationale or overreach? Previous work has shown that there is modest in vitro NECTIN-4 upregulation and incremental tumor growth delay with combination therapy. There is likely an additive, not synergistic effect, but there is uncertain clinical relevance, particularly in the context of enfortumab vedotin + pembrolizumab benefit regardless of NECTIN-4 expression in EV-302 [2].
What are the gains of adding an FGFR inhibitor to enfortumab vedotin + pembrolizumab? To date, in FORAGER-1, 5 patients have been treated with vepugratinib 200 mg BID in combination with enfortumab vedotin + pembrolizumab, of which 4 out of 5 patients responded at the first scan with 3 partial responses and 1 complete response. The overall safety is consistent with that observed with the individual treatment, with the most common treatment-related adverse events including nausea, diarrhea, fatigue, decreased appetite, and dry mouth (40% each). Dr. Gupta notes that the detailed safety data is not shown; thus, potential toxicities may not be addressed.
Dr. Gupta concluded her assessment of the FORAGER-1 phase 1 trial, with the following takeaway points:
- Next-generation FGFR inhibitors represent a step in the right direction, designed for improved selectivity, better tolerability, and the potential to overcome resistance to erdafitinib
- Vepugratinib 200 mg BID showed clinically meaningful activity and acceptable tolerability in heavily pretreated patients with metastatic urothelial carcinoma
- Combination strategies (FGFR inhibitor + enfortumab vedotin + pembrolizumab) remain exploratory, with risk of added toxicity and impact on patients’ quality of life, and it is difficult to demonstrate incremental efficacy beyond enfortumab vedotin + pembrolizumab without randomized trials
- Future efforts should focus on biomarker-driven patient selection, optimized sequencing, and tolerable dosing strategies
Finally, Dr. Gupta discussed the phase 2 TROPION-PanTumor03 study. The first line and beyond treatment landscape in the enfortumab vedotin + pembrolizumab era is highlighted in the following figure:
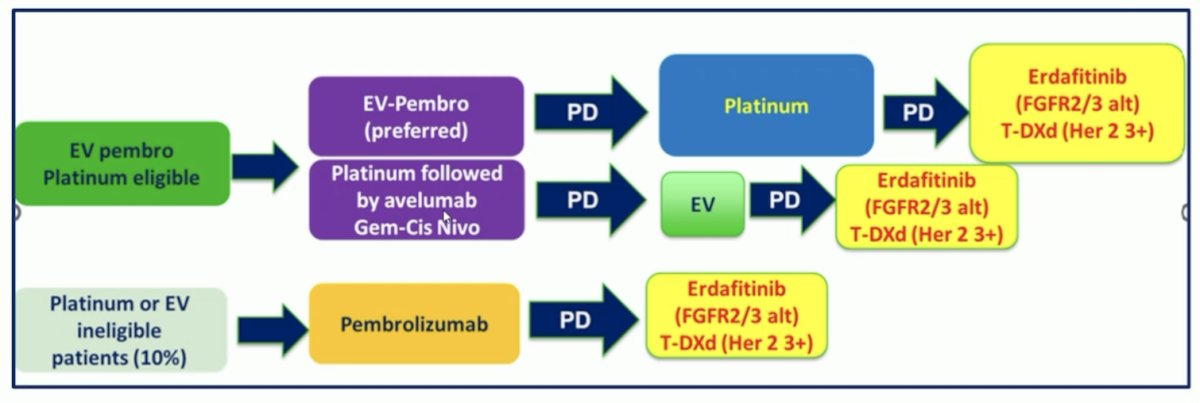
With enfortumab vedotin + pembrolizumab, subsequent lines of therapy increasingly rely on platinum chemotherapy and biomarker-driven agents (ie. FGFR2/3, HER2). Thus, there is a need for new mechanisms and non-overlapping toxicities beyond enfortumab vedotin. To date, anti-TIGIT antibodies have not been delivered in solid tumors. Multiple phase III trials in NSCLC have been negative with monospecific anti-TIGIT antibodies, including: tiragolumab + atezolizumab, vibostolimab + pembrolizumab, ociperlimab + tislelizumab, and belrestotug + dostarlimab. Bispecific PD-1/TIGIT approaches include rilvegostomig testing in TROPION-Lung02 and TROPION-PanTumor03 combinations with datopotamab deruxtecan. Early data shows response signals, but it is unclear if TIGIT adds efficacy beyond PD-1.
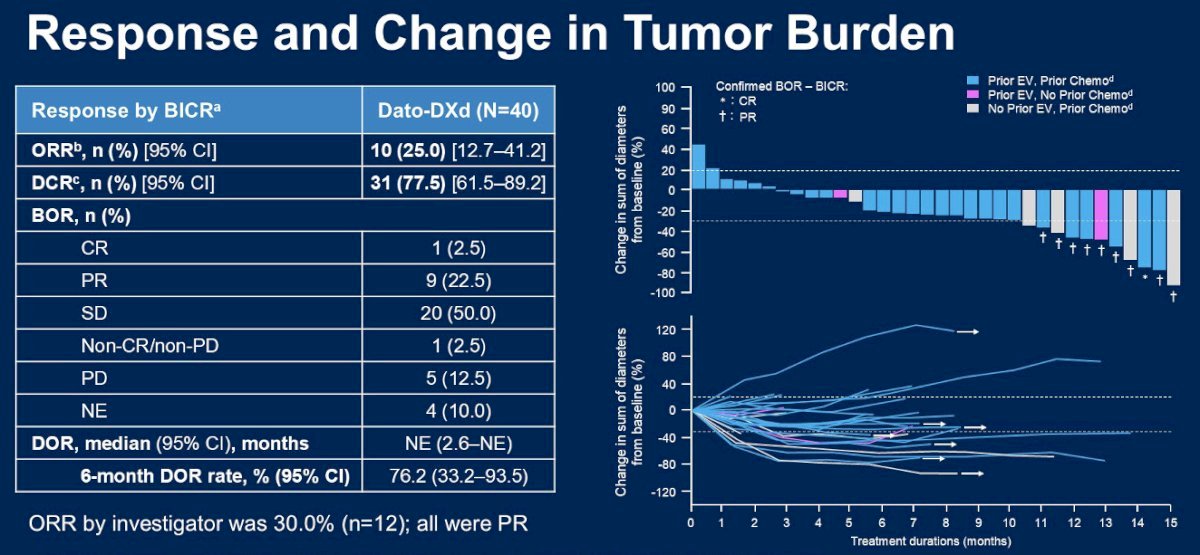
Presented at ASCO GU 2025, the phase 1 TROPION PanTumor01 study of datopotamab deruxtecan in locally advanced/metastatic urothelial carcinoma reported an objective response rate of 25% and a disease control rate of 77.5%. One patient (2.5%) had a complete response, and nine patients had a partial response (22.5%). The median duration of response was not evaluable at this interim analysis, but the 6-month duration of response rate was 76.2%:
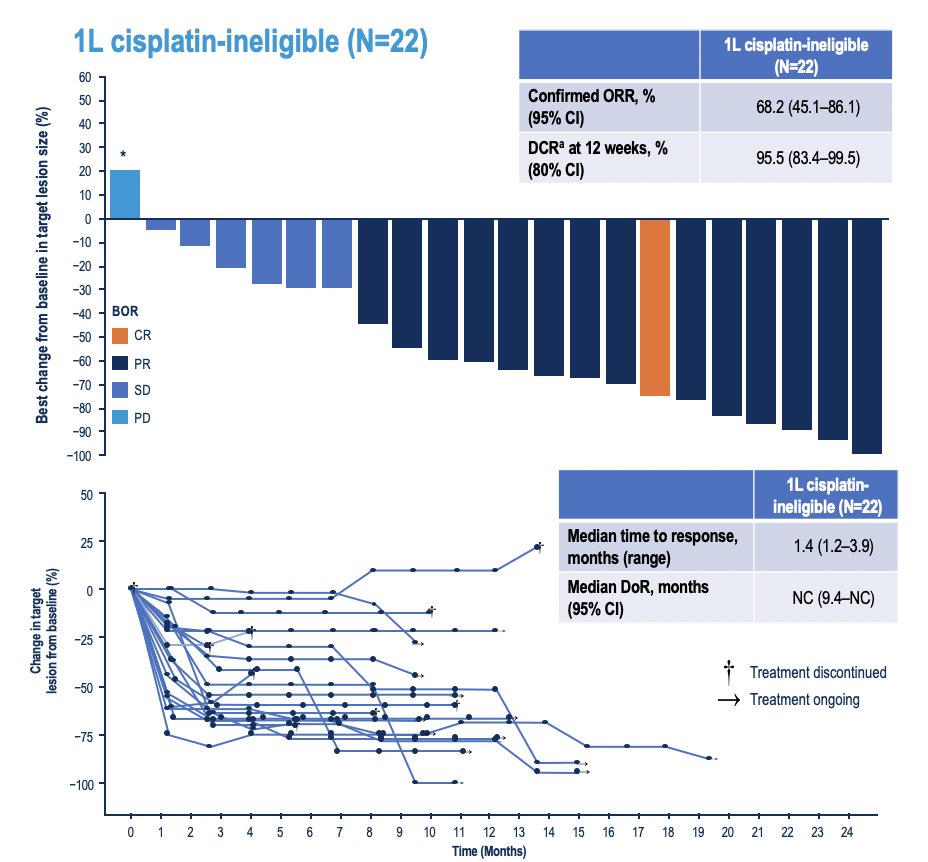
In TROPION-PanTumor03, in the first-line population, the objective response rate was 68.2% (95% CI 45.1-86.1), and the disease control rate was 95.5% (80% CI 83.4-99.5) at 12 weeks:
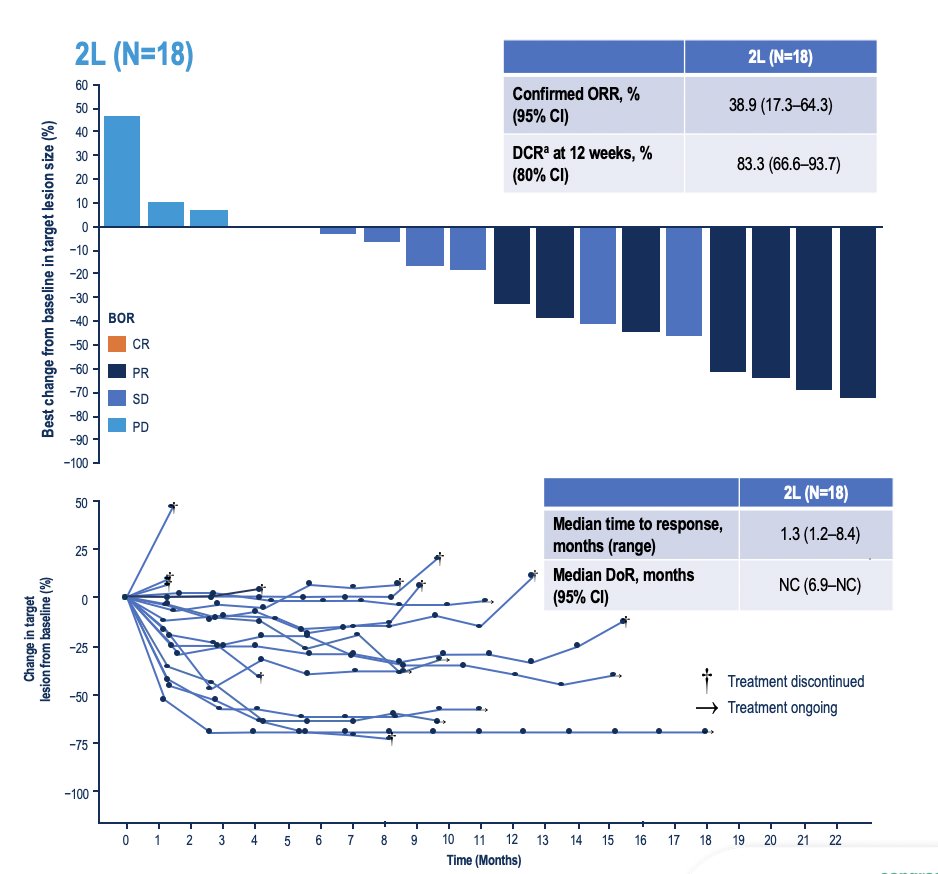
In the second line population, the confirmed objective response rate was 38.9% (95% CI 17.3-64.3), and the disease control rate was 83.3% (80% CI 66.6-93.7) at 12 weeks:
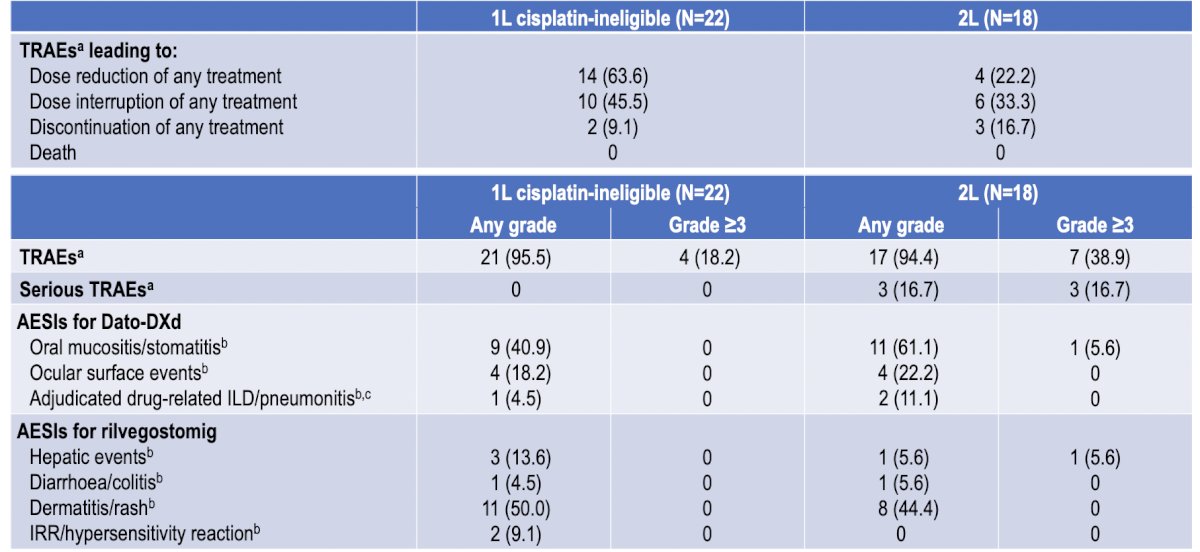
The overall safety summary is highlighted in the following table, notably with no serious treatment adverse events in the first line setting, and 16.7% in the second line setting:
Dr. Gupta concluded her assessment of the TROPION-PanTumor03 study with the following takeaway points:
- Datopotamab deruxtecan + rilvegostomig showed encouraging activity with a manageable safety profile in the first-line cisplatin-ineligible and second-line metastatic urothelial carcinoma setting
- There is no clear incremental benefit from TIGIT blockade; immunotherapy toxicity is minimal
- Further development needs to have a randomized comparison versus datopotamab deruxtecan monotherapy to clarify immunotherapy contribution and avoid unnecessary treatment and financial toxicity
- Cisplatin-ineligible cohort and second-line post-platinum cohort are increasingly moot in the enfortumab vedotin + pembrolizumab era, limiting the relevance of this population
- Datopotamab deruxtecan could be a useful salvage therapy post-enfortumab vedotin + pembrolizumab, with future work defining mechanistic biomarkers and resistance pathways
Presented by: Shilpa Gupta, MD, Director, Genitourinary Medical Oncology, Taussig Cancer Institute, Co-Leader of the Genitourinary Oncology Program, Department of Hematology and Medical Oncology, Cleveland Clinic, Cleveland, OH
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
References:
- Powles T, Catto JWF, Galsky MD, et al. Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer. N Engl J Med. 2024 Nov 14;391(1):1773-1786.
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024 Mar 7;390(10)875-888.