(UroToday.com) The 2025 ESMO annual meeting featured a urothelial carcinoma mini oral session and a discussant presentation by Dr. Stefanie Zschäbitz discussing three abstracts “Randomized Comparison of upfront MRI Versus Transurethral Resection for Staging New Bladder Cancers: Final survival analysis from the BladderPath trial” by Dr. Nicholas James, “Disitamab Vedotin + Tislelizumab as Nephron-Sparing Therapy for High-Risk Upper Tract Urothelial Carcinoma: The Phase II DISTINCT-I Trial” by Dr. Jiwei Huang, and “Neoadjuvant gemcitabine intravesical system (TAR-200) + cetrelimab or cetrelimab alone in patients with muscle-invasive bladder cancer: SunRISe-4 (SR-4) primary analysis and biomarker results” by Dr. Andrea Necchi.
Dr. Zschäbitz started her presentation by discussing BladderPath, which sought to answer whether TURBT can be replaced by mpMRI? And, does delaying the correct definitive treatment affect prognosis? Previously, the BladderPath trial noted that the median time to chemotherapy for participants with muscle-invasive bladder cancer was significantly shorter with initial mpMRI (n = 12, 53 days, 95% CI 20-89) versus TURBT (n = 14, 98 days, 95% CI 72-125; p = 0.02).
In this analysis of BladderPath, for progression-free survival, there appeared to be a clinically meaningful benefit for the MRI pathway among non-muscle invasive bladder cancer patients:
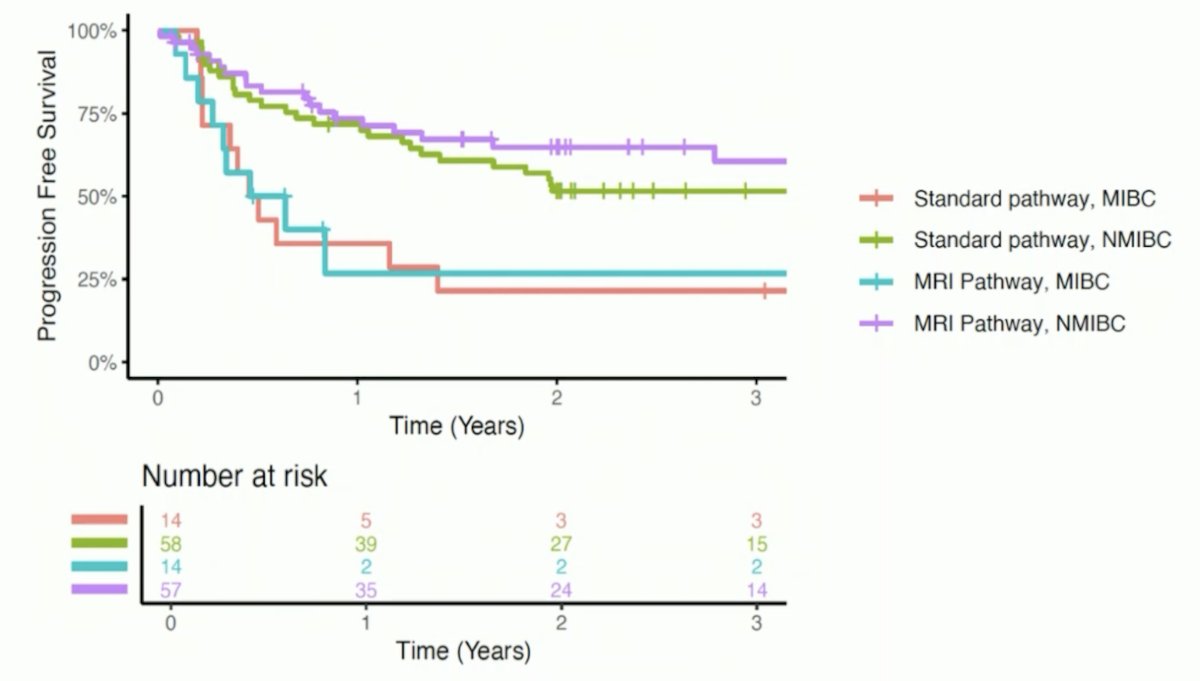
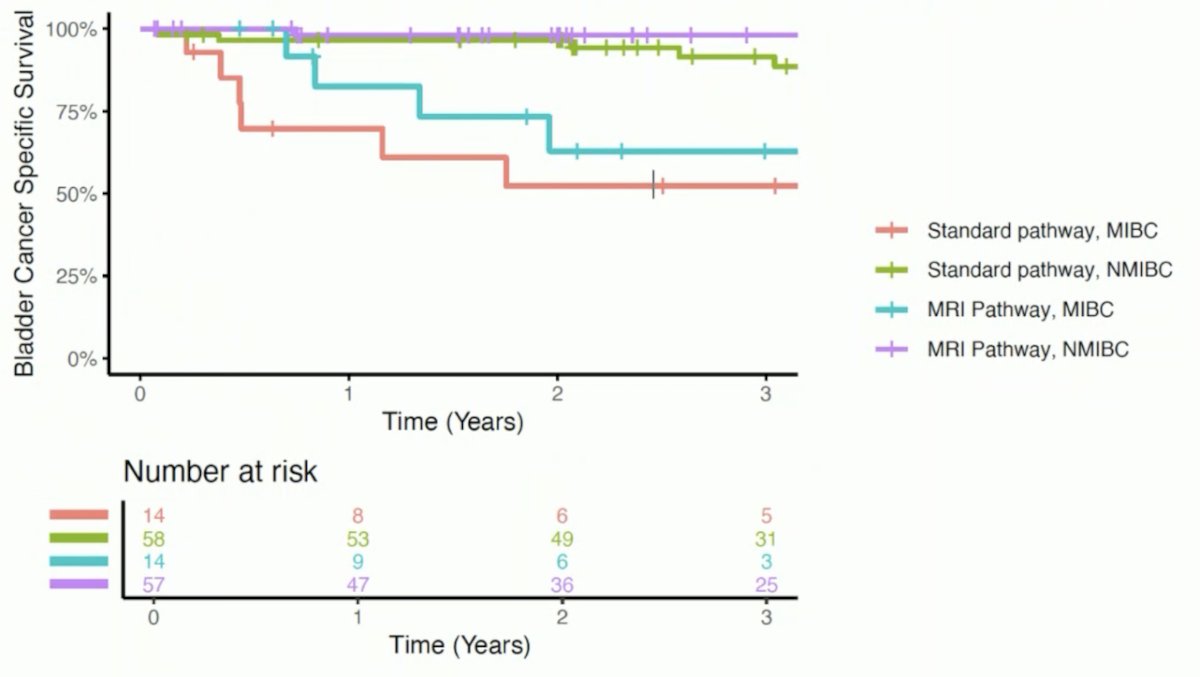
Similarly, there also appeared to be a clinically meaningful benefit for bladder cancer-specific survival for the MRI pathway among muscle-invasive bladder cancer patients:
Is this practice changing? No, but imaging is recommended in localized (>=T1) bladder cancer. The EAU guidelines state that if an MRI is performed for local staging of bladder cancer, it should be done before a TURBT. The ESMO guideline states that for muscle-invasive bladder cancer and high-risk non-muscle invasive bladder cancer, CT/MRI urography (to screen for synchronous upper tract urothelial carcinoma) should be performed. Additionally, for >=pT2 disease, CT of the chest/abdomen/pelvis or MRI of the abdomen/pelvis should be combined with chest CT. Moreover, imaging is recommended before TURBT. The NCCN guidelines state the following:
- CT urography (MR urography) should be performed
- Consider an additional MRI of the pelvis
- Perform a CT chest
- FDG-PET/CT may be performed in certain instances
The strengths of mpMRI in the future of bladder cancer care are its diagnostic accuracy (~90% sensitivity, ~85% specificity), precise anatomic + functional staging, standardized reporting (VI-RADS), and improvement of multidisciplinary communication:
Weaknesses of mpMRI in bladder cancer include (i) its limited availability and heterogeneous protocols, (ii) the learning curve and training gaps, (iii) added cost and time versus a CT scan, and (iv) under-reimbursement in many healthcare systems. Opportunities include integration into bladder sparing strategies, AI/radiomics for predictive modeling, and imaging-molecular biomarker synergy. Finally, threats to mpMRI in bladder cancer include (i) slow adoption, (ii) competing modalities (CT, PET/MRI), (iii) economic + workflow constraints, (iv) limited capacities, and (v) resistance to change.
Second, Dr. Zschäbitz discussed the phase 2 DISTINCT-I trial. This ongoing study enrolled high-risk upper tract urothelial carcinoma patients (N0-1[M0] with absolute/relative renal preservation indications: solitary kidney or eGFR <60 mL/min/1.73m2). The protocol for this trial included endoscopic biopsy followed by 2-4 cycles of disitamab vedotin (2.0 mg/kg) + tislelizumab (200 mg) every 3 weeks for induction therapy, then kidney-sparing surgery. The primary endpoint was 1-year kidney-intact event-free survival (events: local recurrence, metastasis, death), and secondary endpoints included clinical complete response, renal function preservation, and safety (CTCAE v5.0). The trial design for DISTINCT-I is as follows:
![Second, Dr. Zschäbitz discussed the phase 2 DISTINCT-I trial. This ongoing study enrolled high-risk upper tract urothelial carcinoma patients (N0-1[M0] with absolute/relative renal preservation indications: solitary kidney or eGFR <60 mL/min/1.73m2). The protocol for this trial included endoscopic biopsy followed by 2-4 cycles of disitamab vedotin (2.0 mg/kg) + tislelizumab (200 mg) every 3 weeks for induction therapy, then kidney-sparing surgery. The primary endpoint was 1-year kidney-intact event-free survival (events: local recurrence, metastasis, death), and secondary endpoints included clinical complete response, renal function preservation, and safety (CTCAE v5.0). The trial design for DISTINCT-I is as follows:](/images/com-doc-importer/233-esmo-2025/esmo-2025-discussant-individualizing-care-for-patients-with-localized-urothelial-carcinoma/image-3.jpg)
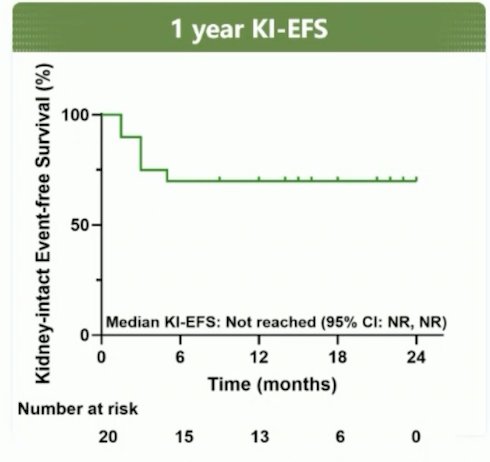
The kidney-intact event-free survival at 1 year was 70%, and the clinical complete response rate increased from 25% after induction therapy to 75% following subsequent kidney-sparing surgery (4-month assessment):
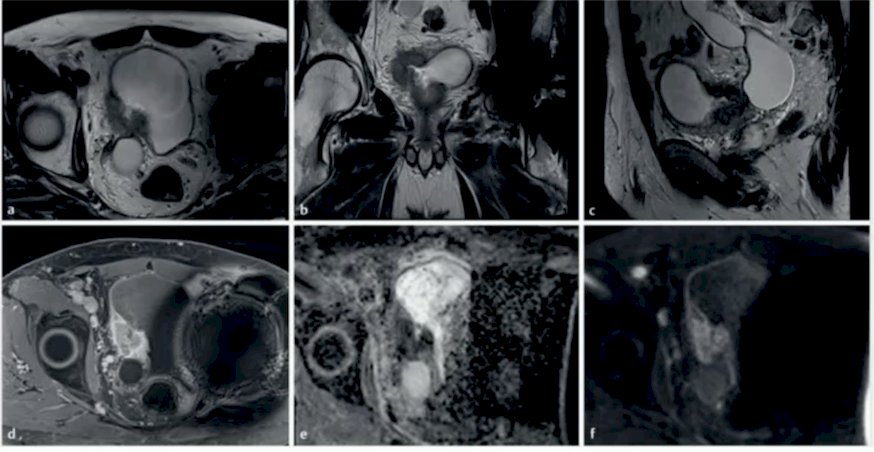
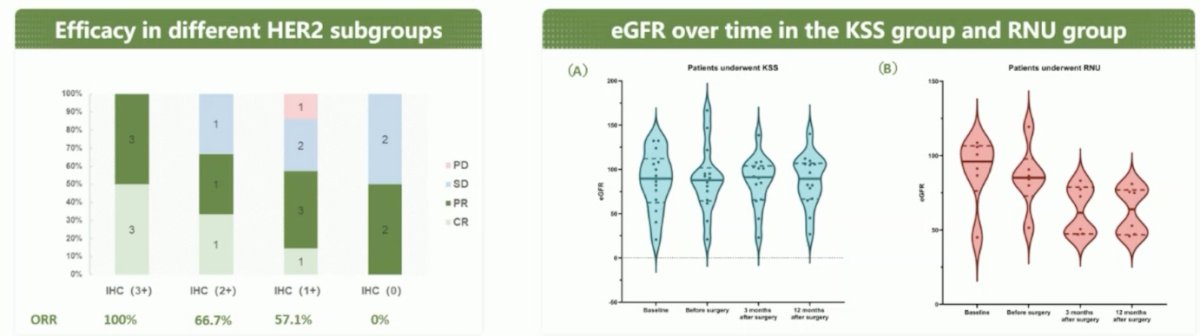
Tumor responses to induction therapy among the 20 patients included complete response (n = 5), partial response (n = 9), stable disease (n = 5), and progressive disease (n = 1), yielding an objective response rate of 70% and a disease control rate of 95%. Pathological examination confirmed a complete response in all 5 patients who had an achieved a clinical complete response. Treatment efficacy was strongly linked to higher levels of HER2 overexpression (2+/3+). The following figures highlight the efficacy in different HER2 subgroups and eGFR over time in the kidney-sparing surgery group and the radical nephroureterectomy group:
Is this practice changing with regard to nephron-sparing procedures for high-risk upper tract urothelial carcinoma patients? No, not currently. The EAU guidelines state that distal ureterectomy with concomitant lymph node dissection for high-risk upper tract urothelial carcinoma in the distal ureter should only be used in highly selected cases where the benefits may be greater than the potential risks. Ureterorenoscopy with laser ablation or segmental ureterectomy can be considered on a case-by-case basis for patients with high-risk disease and imperative kidney-sparing indications. This includes situations such as a solitary kidney, bilateral upper tract urothelial carcinoma, even those harboring high-grade disease and/or infiltrative features, but only in the presence of severe chronic kidney disease or any other comorbidity compromising the use of radical nephroureterectomy. Oncologic safety of nephron-sparing procedures is reasonably established, with the caveat that these are retrospective studies, there is selection bias (patient populations), and there is heterogeneity of inclusion criteria:

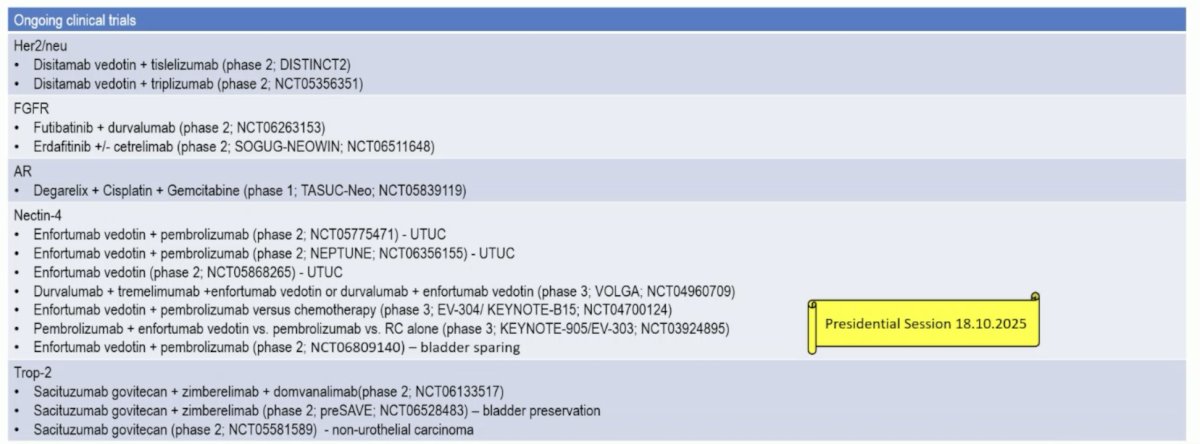
There are several actionable targets in the perioperative disease space, as highlighted in the following table:
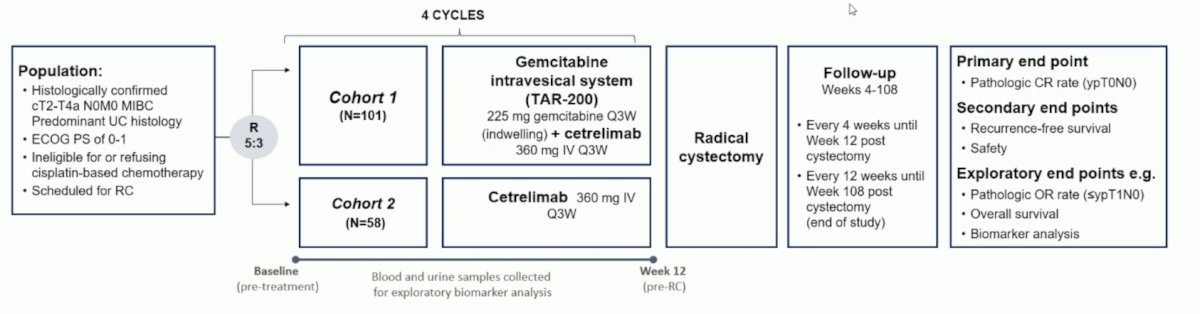
Finally, Dr. Zschäbitz discussed the SunRISe-4 trial. In SunRISe-4, eligible patients planned for radical cystectomy had age ≥18 years, an ECOG performance status of 0-1, cT2-T4a N0M0 muscle-invasive bladder cancer, and were ineligible/refusing neoadjuvant platinum-based chemotherapy. Patients were randomized 5:3, stratified by TURBT completeness (residual tumor ≤3 cm permitted) and T stage, to receive TAR-200 + cetrelimab (cohort 1) or cetrelimab alone (cohort 2). The primary endpoint was the pathologic complete response rate at radical cystectomy. Additional endpoints included pathologic overall response (defined as ≤ypT1) rate, recurrence-free survival, safety, and utDNA/ctDNA:
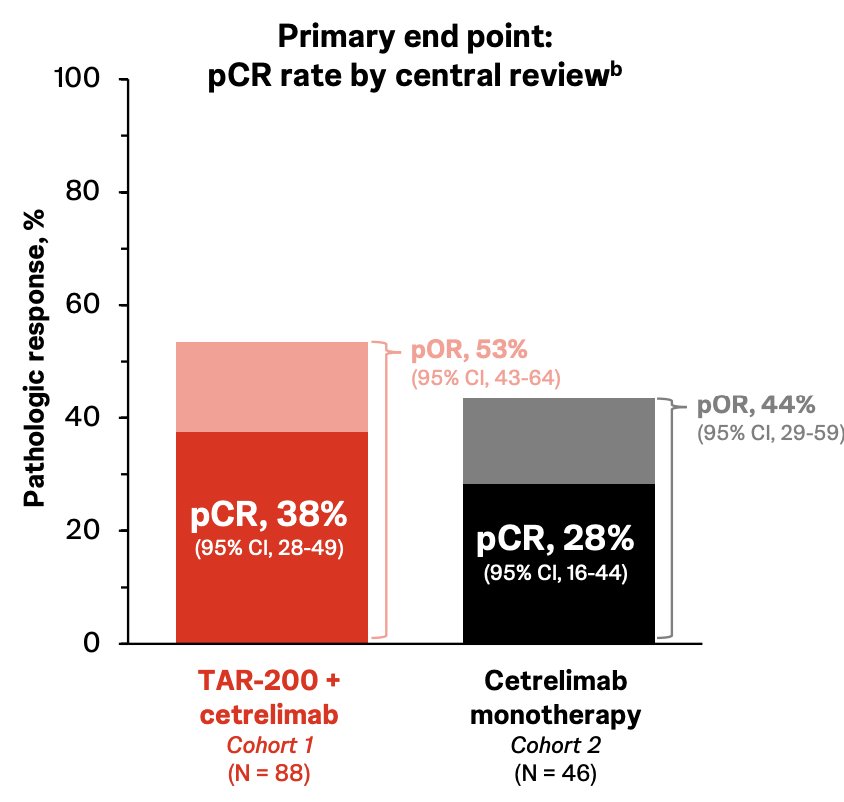
Pathologic complete response was 38% in cohort 1 versus 28% in cohort 2, which was also associated with an improved pathologic overall response in cohort 1 (53%) versus cohort 2 (44%):
The 1-year recurrence-free survival rate was higher in cohort 1 (77%, 95% CI 67-85) than in cohort 2 (64%, 95% CI 47-77):
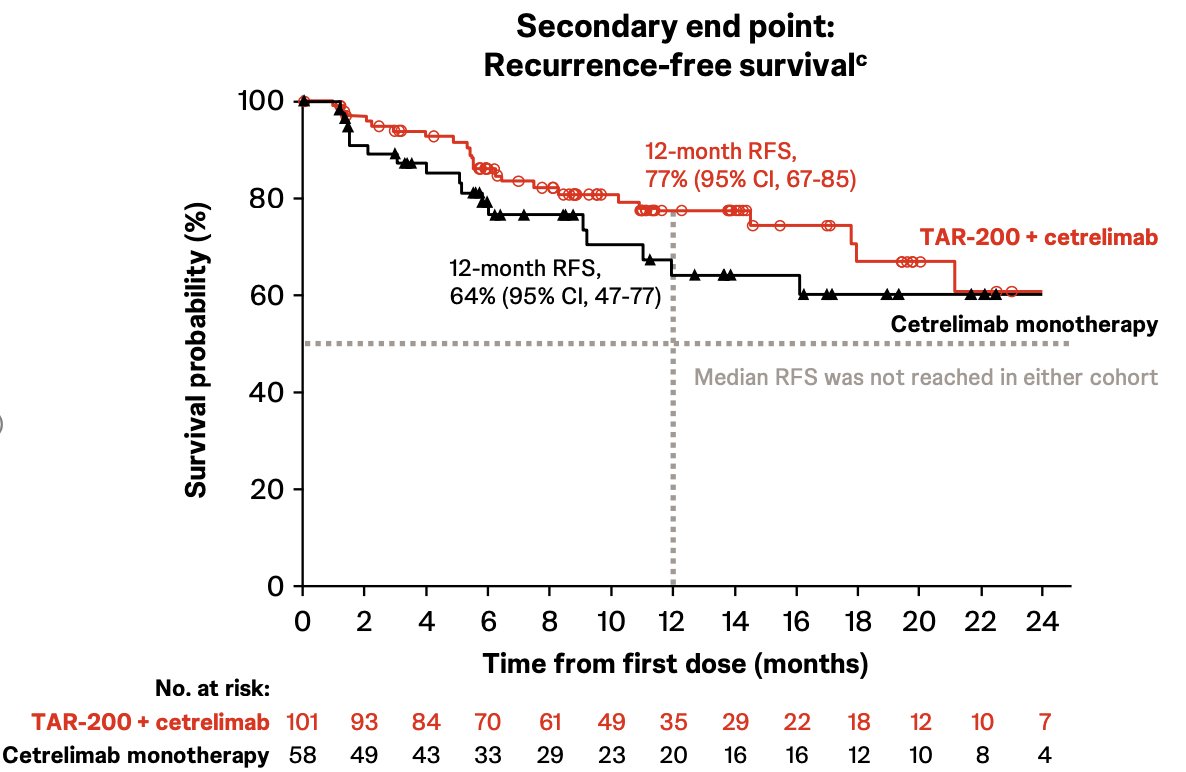
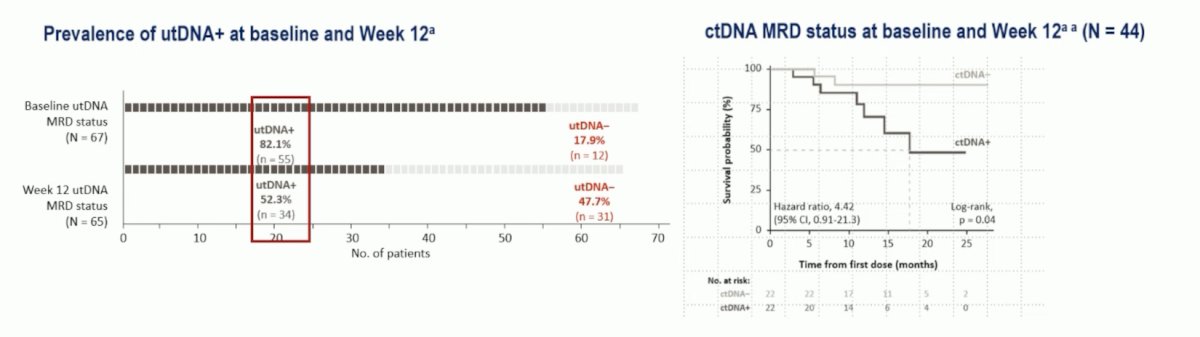
Dr. Zschäbitz emphasized that the absolute difference in pathologic complete response was 10%, and the absolute difference in 1-year recurrence-free survival rate was 13%. This analysis also showed that utDNA may also be a potential marker of local disease, specifically a utDNA-negative status at week 12 was strongly associated with pathological complete response, but not recurrence-free survival. cDNA may be a potential marker of non-local disease, specifically ctDNA negative status was strongly associated with longer recurrence-free survival, but not with pathologic complete response:
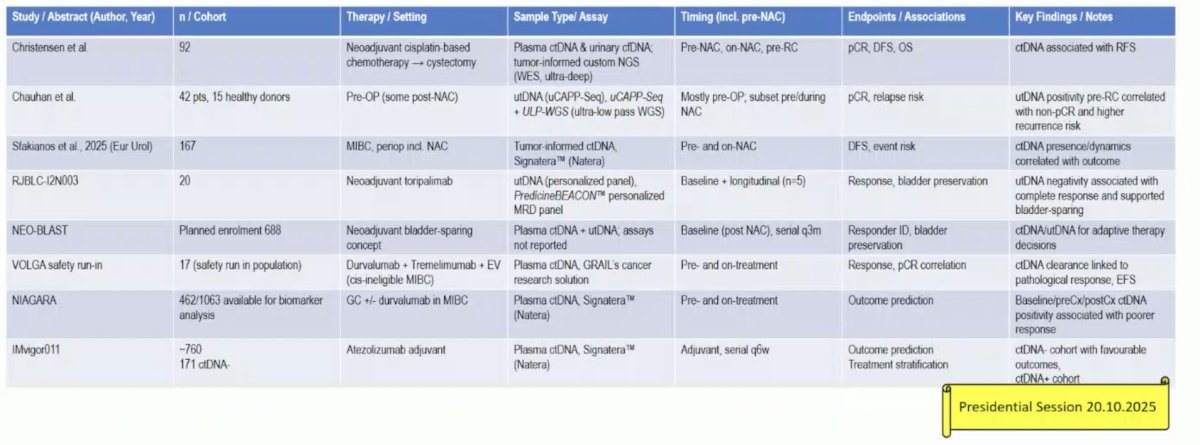
The following table highlights the current literature for utDNA and ctDNA:
Dr. Zschäbitz concluded by highlighting open questions in the perioperative setting +/- organ preservation, specifically identifying the optimal:
- Candidate for organ preservation
- Duration of therapy
- Choice of systemic therapy
- Interval/method of follow-up care (endoscopy, imaging, ctDNA, utDNA)
- Process of shared decision-making with patients
Presented by: Stefanie Zschäbitz, MD, National Center for Tumor Diseases Heidelberg, Heidelberg, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.