(UroToday.com) The 2025 ESMO annual meeting featured a urothelial carcinoma proffered paper session and a discussant presentation by Dr. Clara Steiner discussing three abstracts “DISCUS: A phase II study comparing 3 vs 6 cycles of platinum-based chemotherapy prior to maintenance avelumab in advanced urothelial cancer” by Dr. Enrique Grande, “Adjuvant nivolumab vs placebo for high-risk muscle-invasive urothelial carcinoma: 5-year efficacy and ctDNA results from CheckMate 274” by Dr. Matthew Galsky, and “A blinded, exploratory phase 2 trial of nivolumab and the GDF-15 neutralizing antibody visugromab or placebo as neoadjuvant treatment of patients with muscle-invasive bladder cancer (MIBC): Primary results of the GDFather-NEO trial” by Dr. Andrea Necchi.
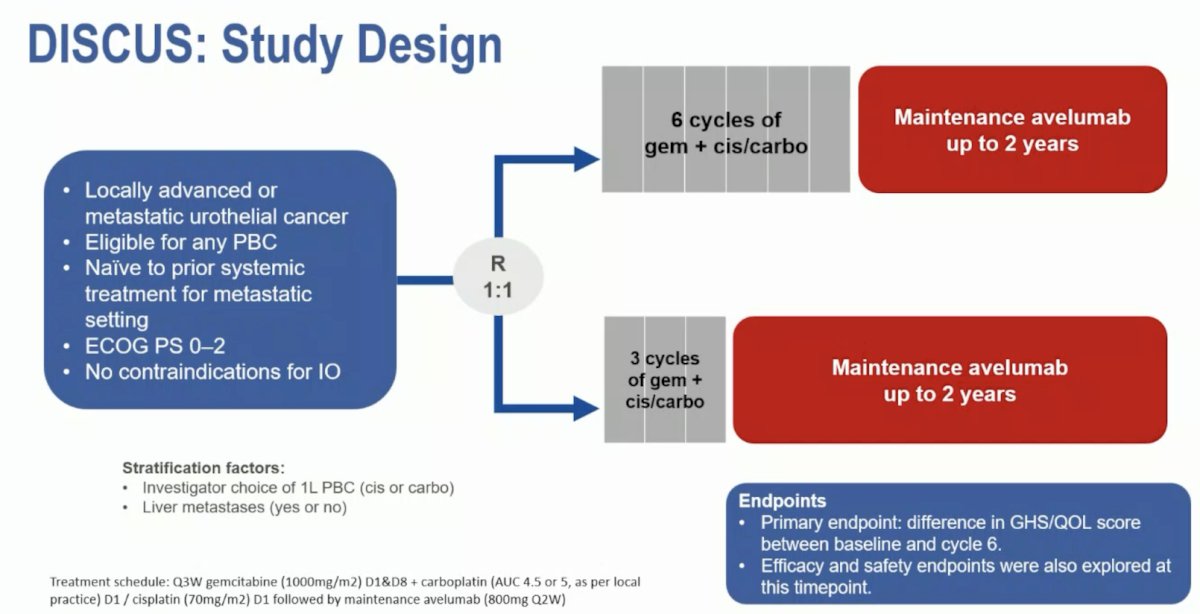
In DISCUS, patients with previously untreated advanced urothelial carcinoma were randomized 1:1 to receive 3 or 6 cycles of gemcitabine/cisplatin or gemcitabine/carboplatin, followed by maintenance avelumab. The dual primary endpoints were patient-reported outcomes (EORTC QLQ-C30 GHS/quality of life scale score; change in quality of life at cycle 6 of treatment versus baseline) and overall survival. Secondary endpoints included additional patient-reported outcomes analysis, progression-free survival, and safety. The trial design for DISCUS is as follows:
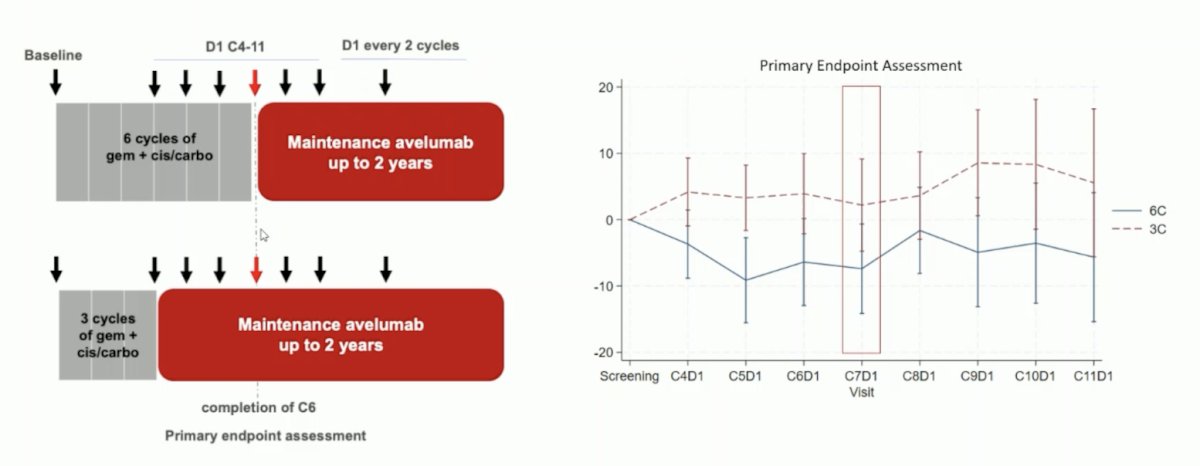
The mean quality of life change between baseline and cycle 6 was 0.0 (95% CI: -5.9, 5.2) in the 3 cycle arm versus -8.5 (95% CI: -14.1, -2.9) in the 6 cycle arm, with a clinically significant difference favoring the 3 cycle arm (+8.5 points, 95% CI: 0.7–16.3; p = 0.016). The median overall survival was 18.9 months in both arms (HR 1.15, 95% CI 0.72–1.86; p = 0.56). For the key secondary endpoint of progression-free survival, which was 8 months for 6 cycles of chemotherapy (95% CI 6.7–11.9) versus 9.0 months for 3 cycles of chemotherapy (95% CI 6.9–12.7); HR 1.05 (95% CI 0.73–1.53; p = 0.79). Dr. Steiner questions the specific timing of quality of life assessment data collection, specifically that for the 6-cycle arm, this occurred right after the last dose of chemotherapy, whereas for the 3-cycle arm, this occurred after chemotherapy and during maintenance avelumab:
How does the DISCUS data fit into the first-line treatment for metastatic urothelial carcinoma landscape? Notably, 74% of patients receiving 3 cycles of chemotherapy reached maintenance avelumab versus 56% of patients receiving 6 cycles of chemotherapy:

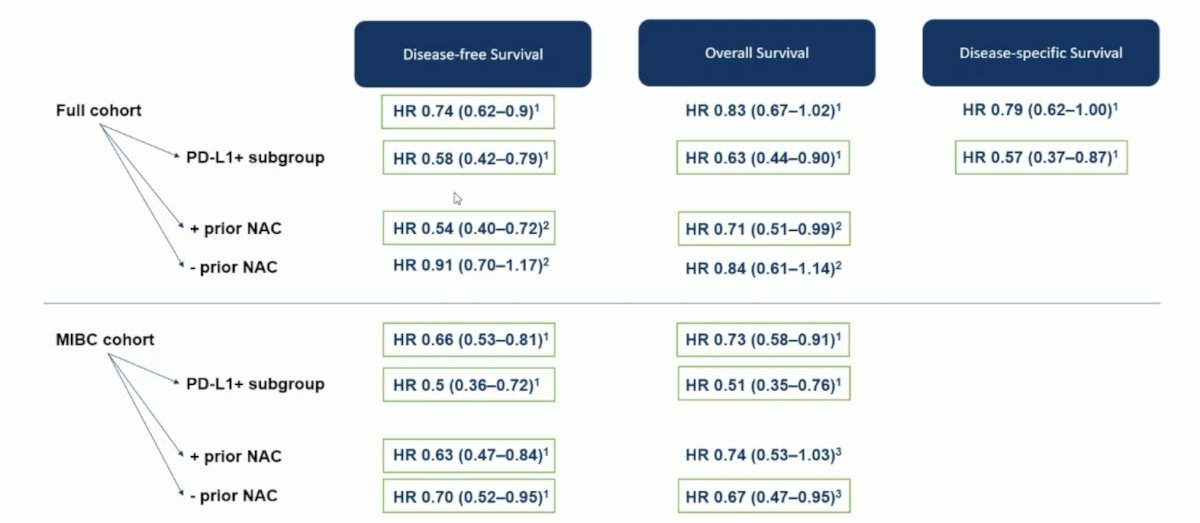
Next, Dr. Steiner discussed the 5-year outcomes of CheckMate 274, highlighting the disease-free survival, overall survival, and disease-specific survival outcomes amongst the full cohort and muscle-invasive bladder cancer cohort:
How does the updated CheckMate 274 data fit into the increasingly busy adjuvant/perioperative disease space?

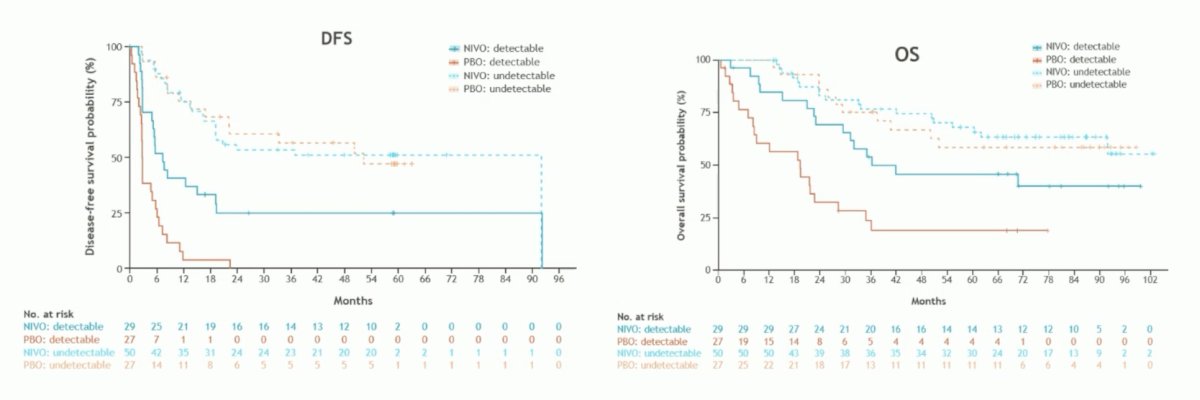
Dr. Steiner notes that ctDNA helps select patients who benefit from adjuvant nivolumab. Within the ctDNA detectable subgroup, nivolumab improved median disease-free survival (HR 0.35, 95% CI 0.18-0.66) and overall survival (HR 0.41, 95% CI 0.20-0.83) versus placebo. Additionally, despite a small number of samples analyzed, the trend of improvement for disease-free survival and overall survival is evident in patients with undetectable ctDNA:
Notably, at ESMO 2025, the biomarker-based IMvigor011 trial will present data at the Presidential Symposium 3:

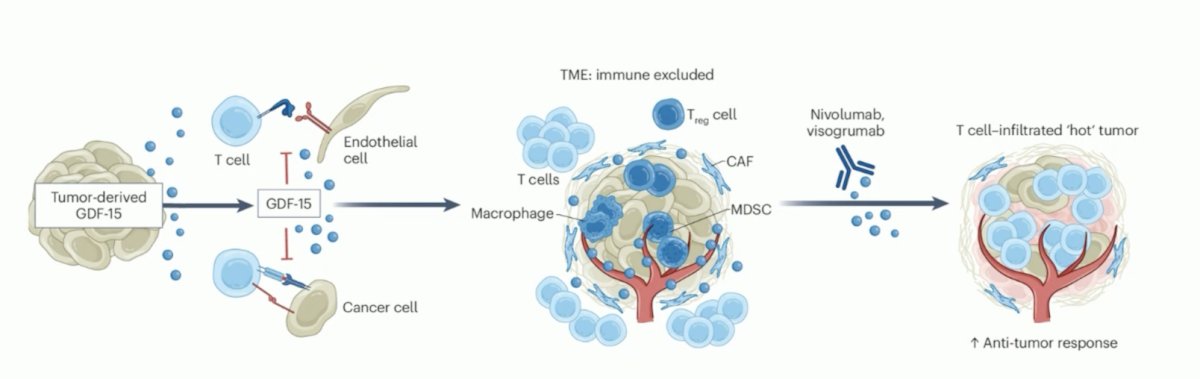
Finally, Dr. Steiner discussed the GDFather-NEO phase 2 trial. GDF-15 is a potent local immunosuppressor in the tumor microenvironment:
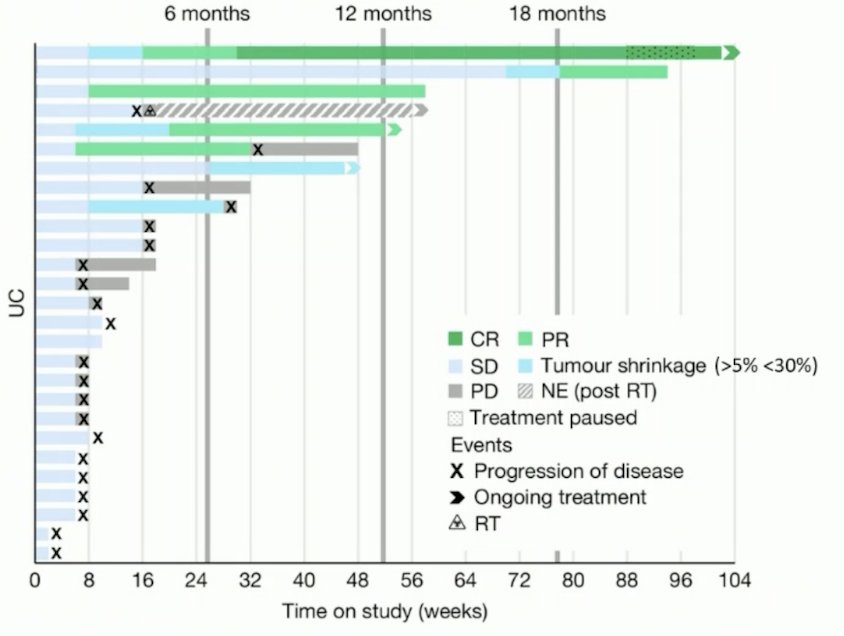
Looking back at the GDFather 1/2a trial,1 this included patients with metastatic urothelial carcinoma with a median of 3 lines of prior therapy, including those receiving previous immunotherapy. The median duration of response was 14.4 months, with 1 ongoing complete response > 20 months:
In urothelial carcinoma and NSCLC, >= 50 % of the responders achieved better outcomes versus prior PD-1/PD-L1 treatments.
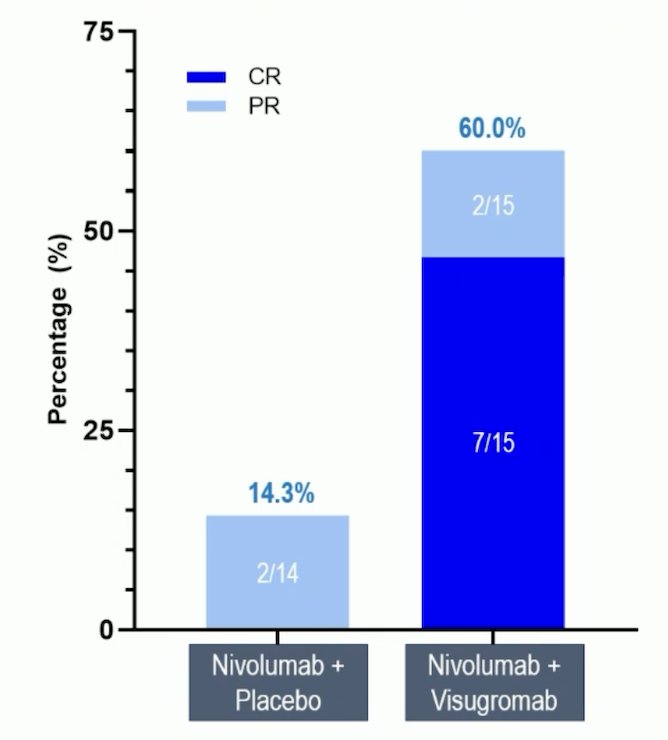
In GDFather-NEO, the objective response rate as per RECIST v1.1 was 60.0% (7 complete responses, 2 partial responses) versus 14.3% (no complete responses, 2 partial responses) for nivolumab + visugromab versus nivolumab + placebo:
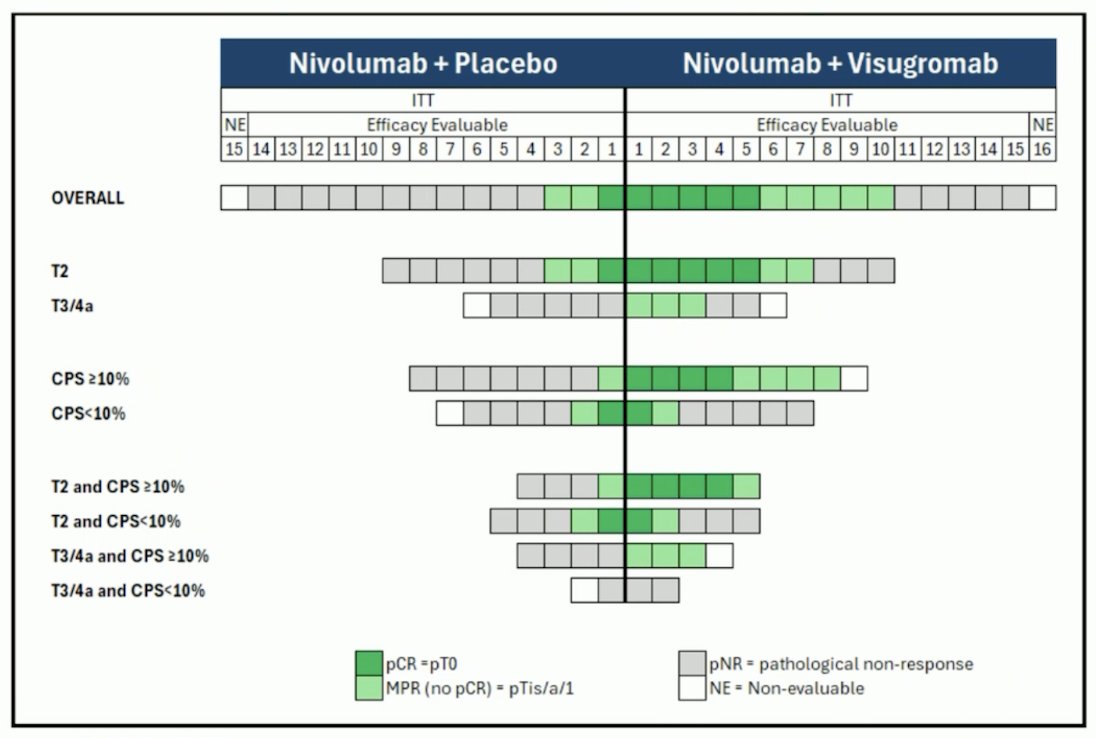
Moreover, nivolumab + visugromab was superior across all T stages and dominantly in CPS≥ 10%:
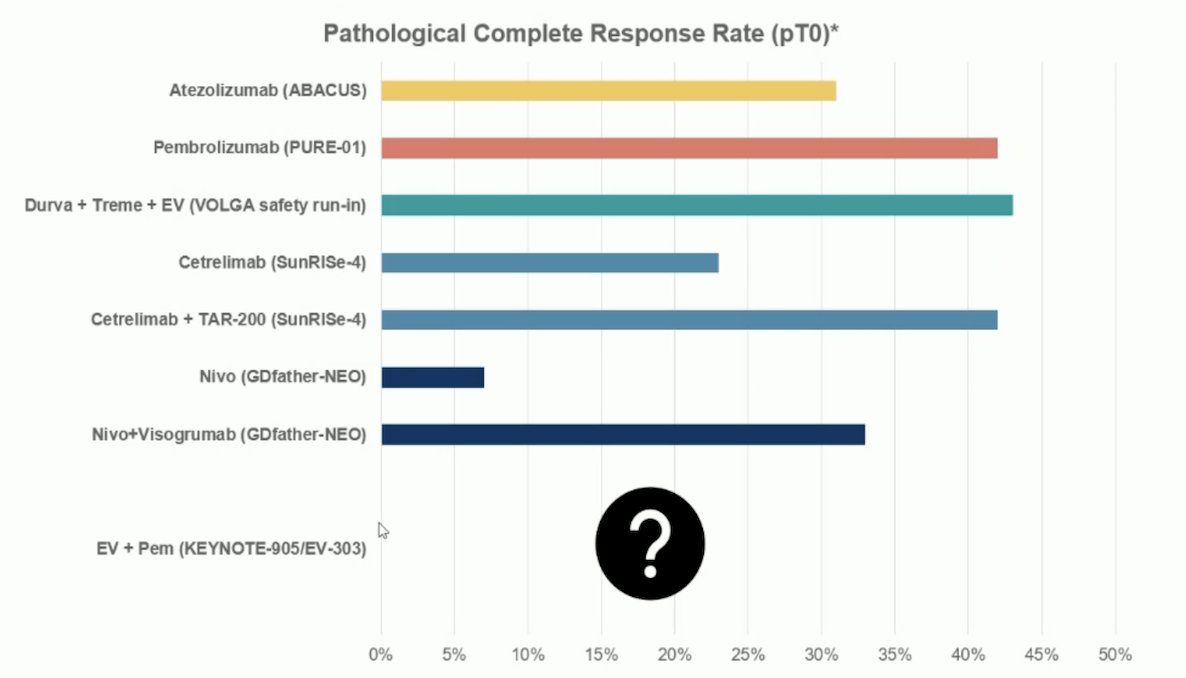
How does nivolumab + visugromab fit into the platinum-ineligible patients or those refusing chemotherapy landscape? The following highlights pT0 rates, with the caveat that the EV-303/KEYNOTE-905 trial will have data presented at the ESMO 2025 Presidential Symposium 1 session:
Dr. Steiner concluded her discussant presentation with the following key takeaways:
- Starting maintenance after a few cycles of chemotherapy improves quality of life
- ctDNA refines patient selection for adjuvant therapy
- Targeting GDF-15 may be an emerging approach to enhance immunotherapy effectiveness
Presented by: Clara Steiner, Postdoctoral Research Fellow, Dana-Farber Cancer Institute, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
Reference:
- Melero I, de Miguel Luken M, de Velasco G, et al. Neutralizing GDF-15 can overcome anti-PD-1 and anti-PD-L1 resistance in solid tumours. Nature. 2025 Jan;637(8048):1218-1227.
Adjuvant Nivolumab Versus Placebo for High-Risk Muscle-Invasive Urothelial Carcinoma: 5-Year Efficacy and ctDNA Results from CheckMate 274.
ESMO 2025: Adjuvant Nivolumab versus Placebo for High-Risk Muscle Invasive Urothelial Carcinoma: 5-Year Efficacy and ctDNA Results from CheckMate 274