The 2025 ESMO annual meeting featured a urothelial carcinoma mini oral session and a presentation by Dr. Sun Young Rha discussing results from the phase 2 TROPION-PanTumor03 study assessing datopotamab deruxtecan + rilvegostomig in patients with locally advanced or metastatic urothelial cancer. Both first-line and second-line treatment of locally advanced or metastatic urothelial cancer have evolved; however, a need for novel therapies remains.
Datopotamab deruxtecan, a TROP2-directed antibody drug conjugate, is approved for the treatment of HR+/HER2- advanced breast cancer and recently received accelerated approval in the USA for the treatment of locally advanced or metastatic EGFR-mutated lung cancer. Rilvegostomig, an Fc-reduced, monovalent, bispecific IgG1 antibody against PD-1 and TIGIT receptors, has demonstrated enhanced efficacy in freshly isolated NSCLC tumors compared with anti-PD-L1 or anti-TIGIT treatment (alone or in combination) and also showed encouraging efficacy in patients with advanced or metastatic NSCLC. Combining immune checkpoint inhibitors with broad antitumor activity, such as antibody drug conjugates, has shown improved clinical efficacy in patients with locally advanced or metastatic urothelial cancer. TROPION-PanTumor03 (NCT05489211), a phase 2, multicenter, open-label trial is evaluating datopotamab deruxtecan, as monotherapy or in combination, in several tumor types. At ESMO 2025, Dr. Rha and colleagues presented results from patients with locally advanced or metastatic urothelial cancer who received datopotamab deruxtecan + rilvegostomig.
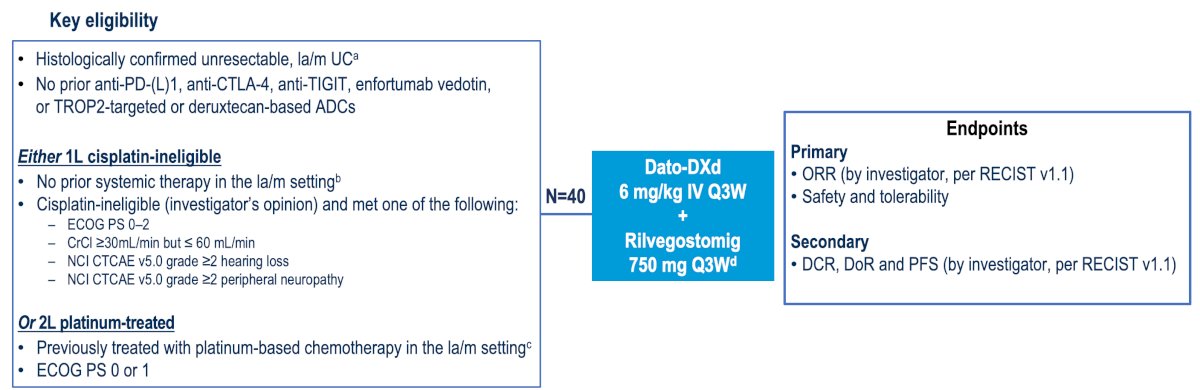
Patients with histologically documented unresectable locally advanced or metastatic urothelial cancer were enrolled in two eligible populations:
- First line population: no prior systemic therapy in the locally advanced or metastatic urothelial cancer setting (progression >12 months after platinum-based neoadjuvant or adjuvant therapy permitted), and ineligible for cisplatin-based chemotherapy
- Second line population: had received previous platinum-based chemotherapy in the locally advanced or metastatic urothelial cancer setting or progressed <12 months after platinum-based neoadjuvant or adjuvant therapy
All patients received datopotamab deruxtecan 6 mg/kg every 3 weeks IV + rilvegostomig. The primary endpoints were confirmed objective response rate and safety/tolerability. Secondary endpoints included progression-free survival, duration of response, and disease control rate. The TROPION-PanTumor03 study design is as follows:
At data cut-off (June 27, 2025), 22 and 18 patients had received datopotamab deruxtecan + rilvegostomig in the first-line and second-line populations, respectively. The median patient age was (first line) 71 (range: 53-85) and (second line) 66 (range: 56-78) years. The remaining baseline characteristics and demographics are in the table:

The median duration of follow-up was 6.7 months in the first line (range 2.6–15.3 months), and 6.9 months (range 4.1–13.6 months) in the second line. In the first line population, the objective response rate was 68.2% (95% CI 45.1-86.1), and the disease control rate was 95.5% (80% CI 83.4-99.5) at 12 weeks: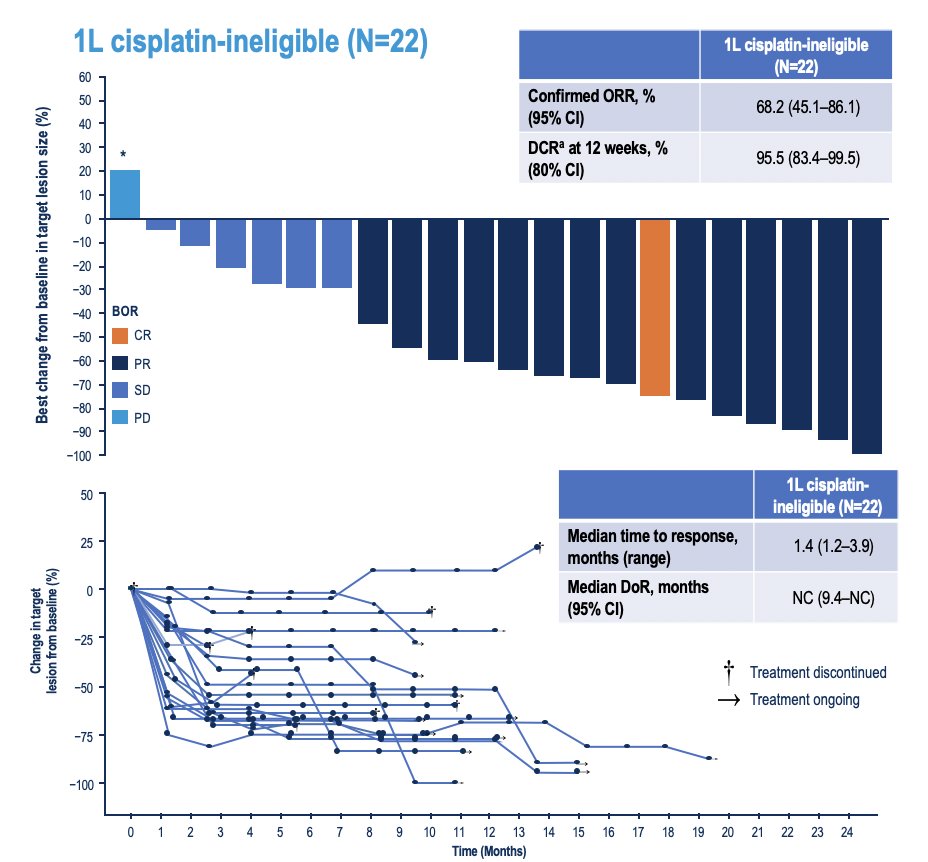
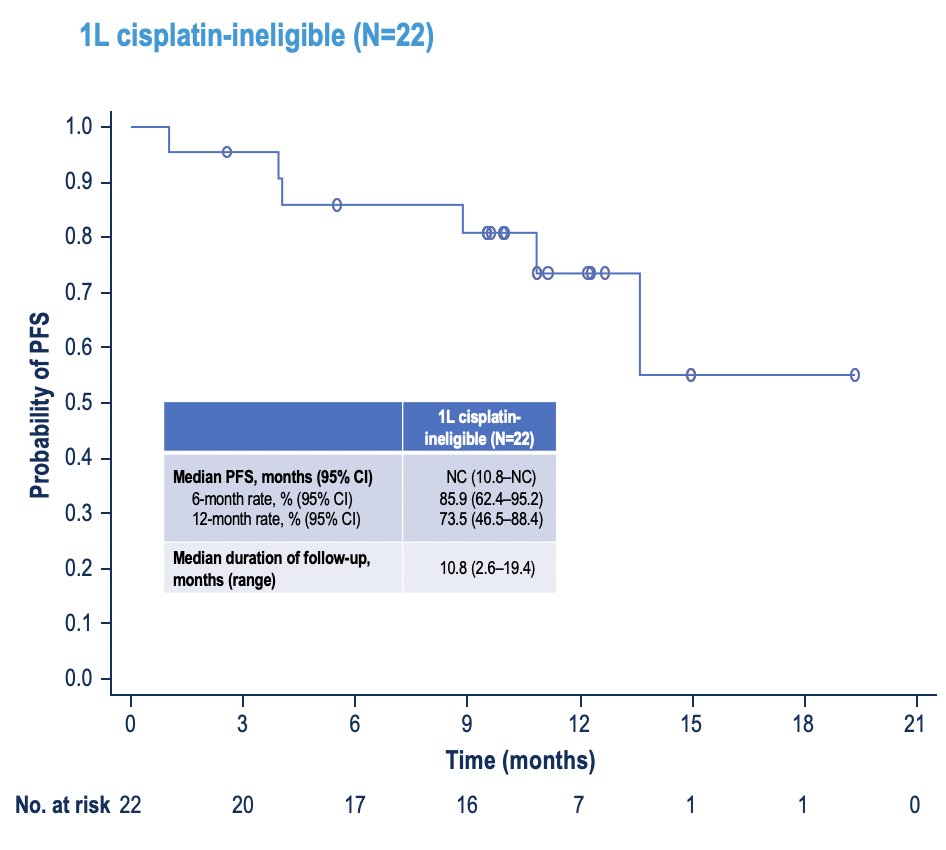
The median duration of response and median progression-free survival were not reached:
In the second line population, the confirmed objective response rate was 38.9% (95% CI 17.3-64.3), and the disease control rate was 83.3% (80% CI 66.6-93.7) at 12 weeks:
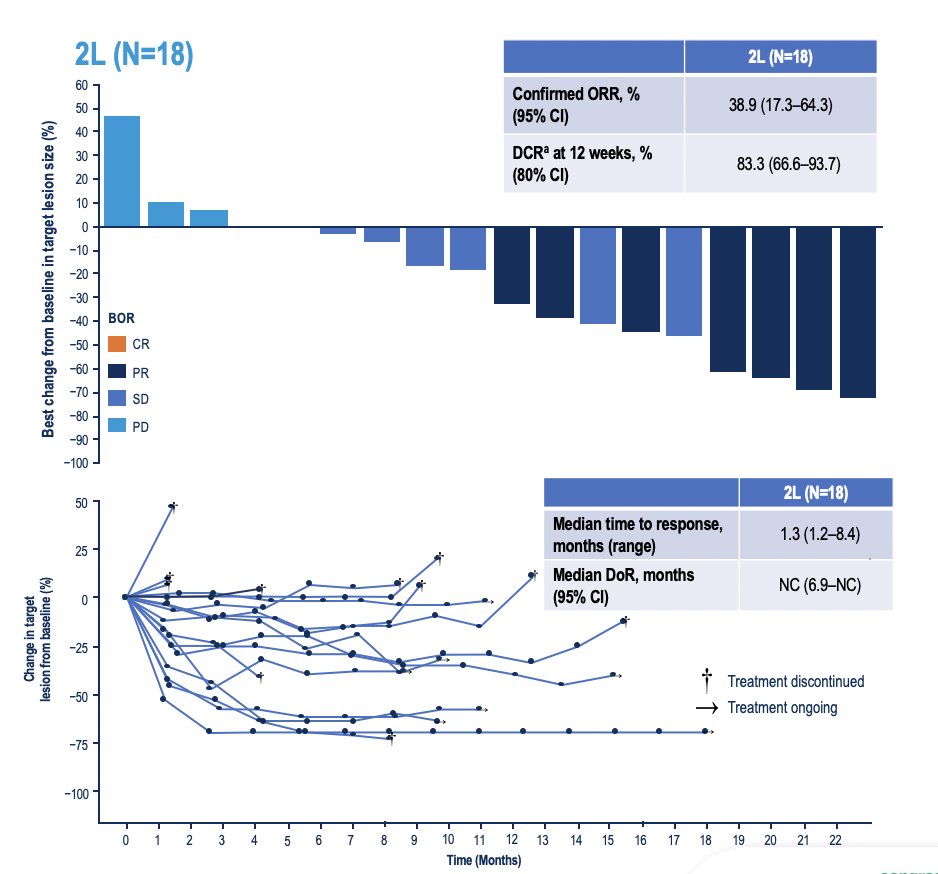
The median duration of response was not reached, and the median progression-free survival was 12.5 months (95% CI 4.2 to not reached):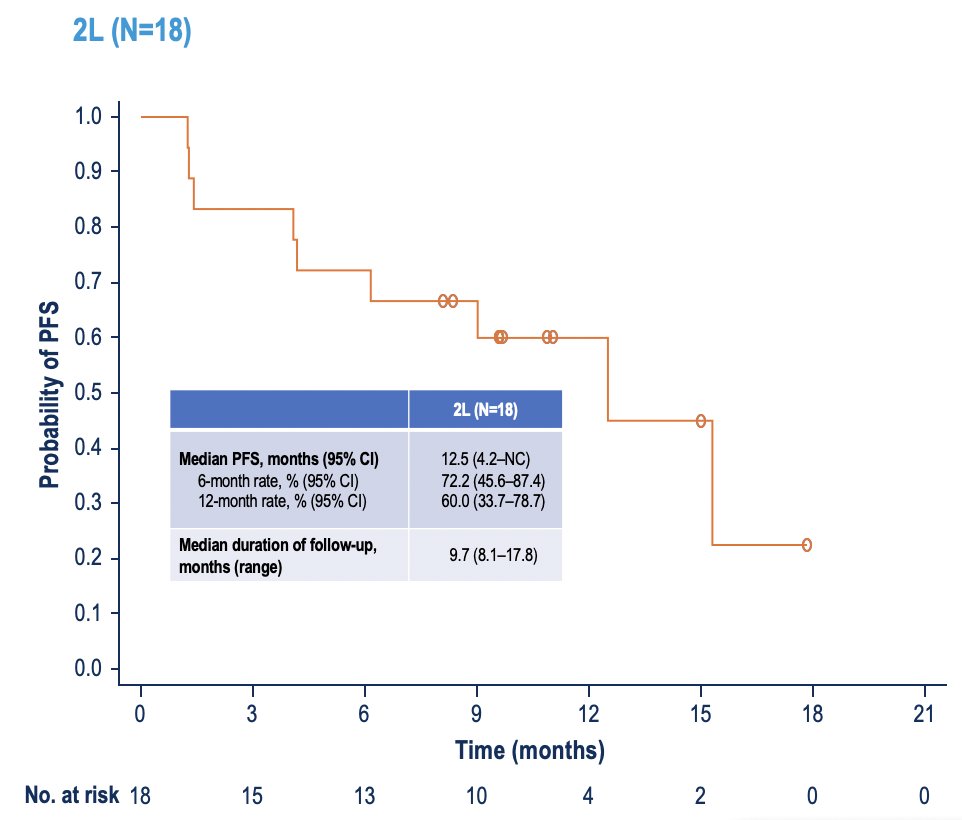
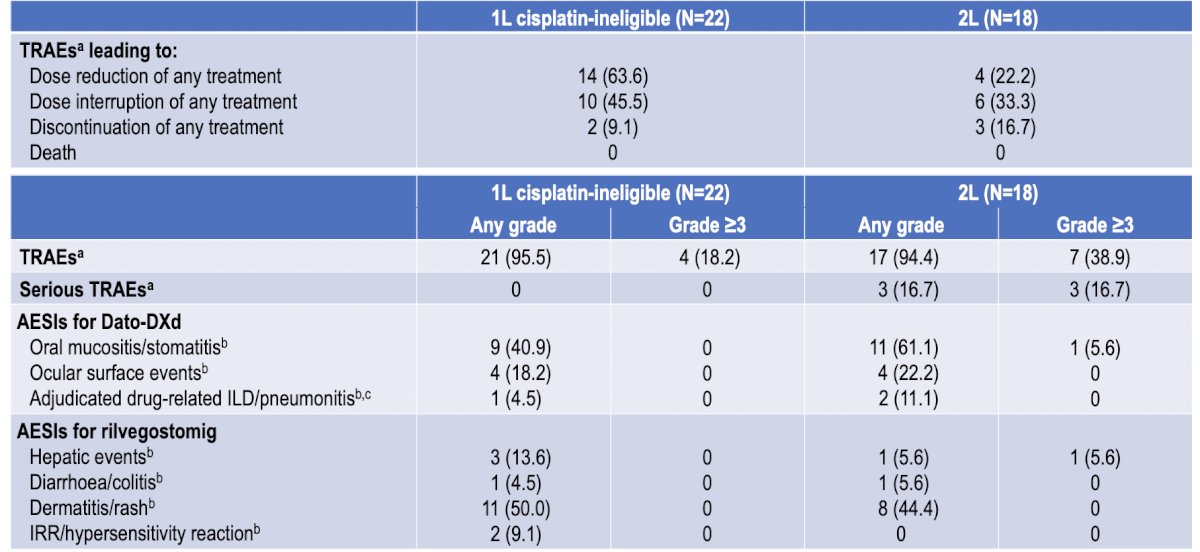
The overall safety summary is highlighted in the following table, notably with no serious treatment adverse events in the first line setting, and 16.7% in the second line setting:
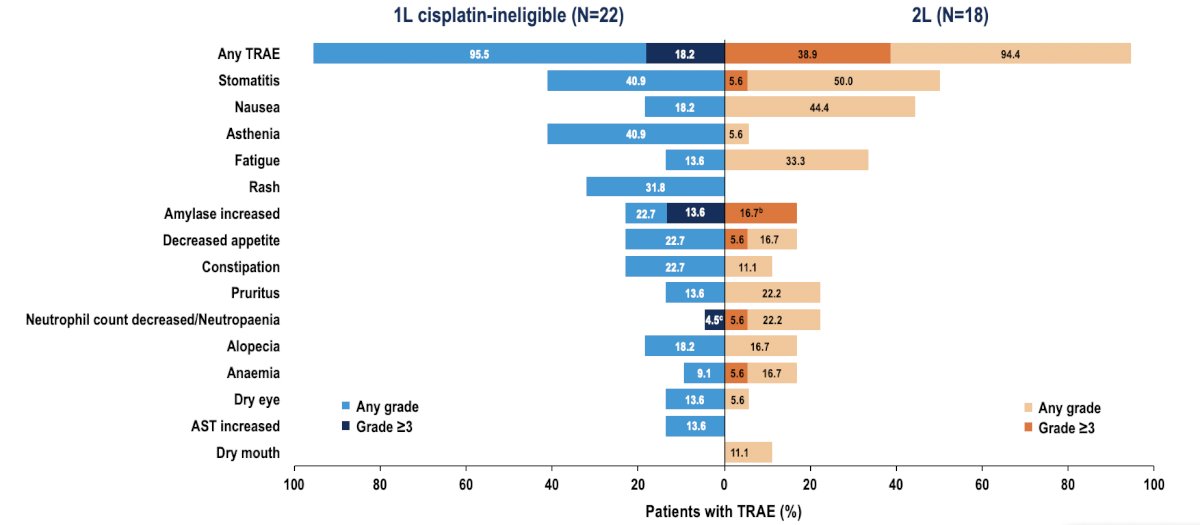
The most common treatment-related adverse events were stomatitis, nausea, and asthenia:
Dr. Rha concluded her presentation discussing results from the phase 2 TROPION-PanTumor03 study with the following take-home points:
- The combination of datopotamab deruxtecan + rilvegostomig demonstrated promising efficacy in patients with locally advanced or metastatic urothelial cancer who were cisplatin-ineligible and patients who had progressed on prior platinum-based chemotherapy
- The safety profile of datopotamab deruxtecan + rilvegostomig was consistent with previous reports of this combination. No new safety signals were identified
- These results warrant further exploration of datopotamab deruxtecan + rilvegostomig in the first-line locally advanced or metastatic urothelial cancer setting
Presented by: Sun Young Rha, MD, Yonsei Cancer Center, Seoul, Republic of Korea
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.