(UroToday.com) The 2023 European Society of Medical Oncology (ESMO) Annual Congress held in Madrid, Spain between October 20th and 24th, 2023 was host to a non-prostate, genitourinary tumors mini oral session. Dr. Patrizia Giannatempo delivered the discussant for the preceding two presentations:
- Impact of Positron Emission Tomography (PET) Imaging on Staging of Muscle-Invasive Bladder Cancer (MIBC) [PET-MUSE]
- Erdafitinib vs Chemotherapy in Patients With Advanced or Metastatic Urothelial Cancer With Select FGFR Alterations: Subgroups From the Phase 3 THOR Study
Dr. Giannatempo began by discussing the PETMUSE study, which included patients with cT2-4aN0-3M0 urothelial cancer, staged using CT scan and TURBT, and were planned for radical cystectomy or trimodality therapy. This patient population (n=292) was planned for a 2:1 randomization to the FDG PET-CT experimental arm (n=194) or no FDG PET-CT control arm (n=98). Following imaging, patients proceeded to neoadjuvant chemotherapy (if clinically indicated), followed by surgery or radiotherapy. The primary outcome was proportion of patients not receiving the expected treatment, with secondary outcomes including change in treatment plan, disease-free survival, overall survival, and quality of life outcomes.
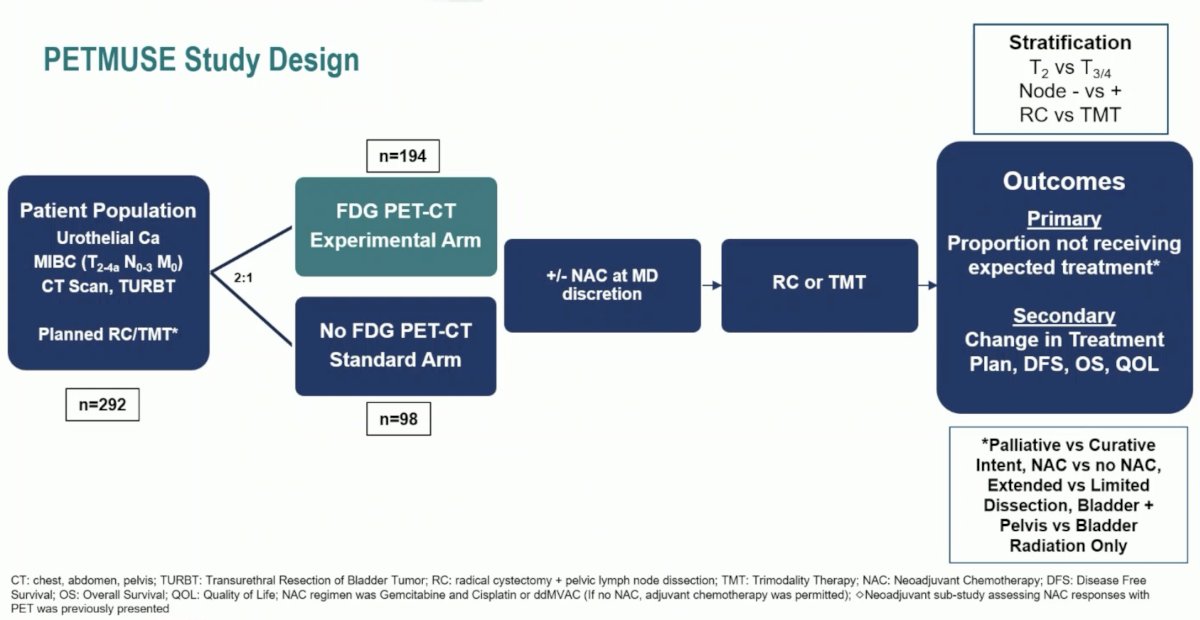
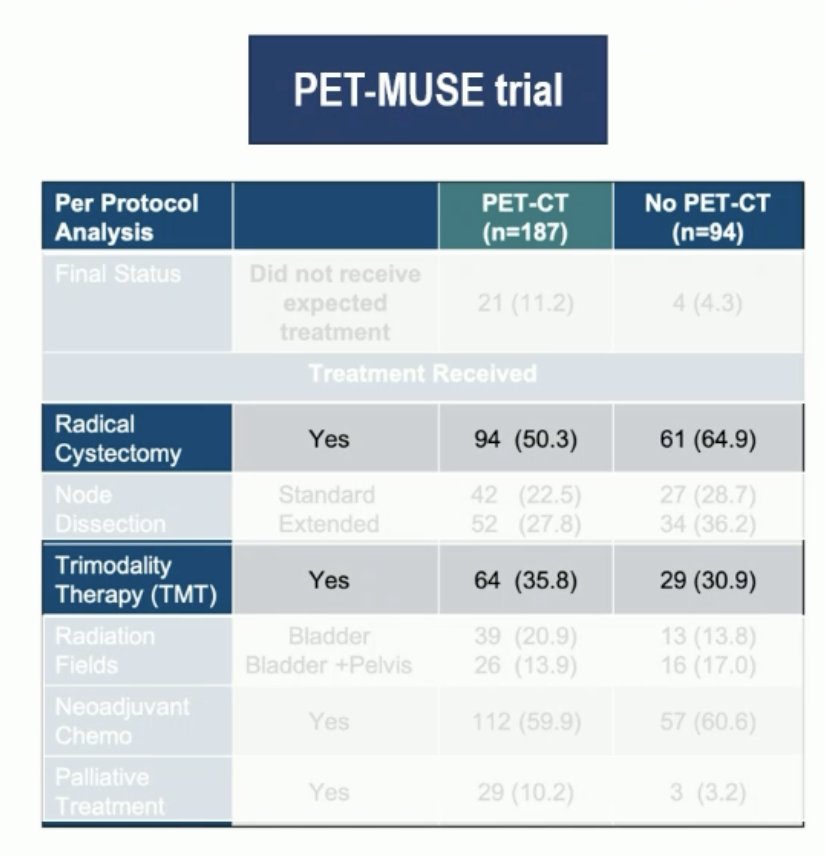
In this trial, 11.2% of patients in the PET-CT arm did not receive the expected treatment, compared to 4.3% in the no PET-CT arm (OR 2.87, 95% CI: 0.95 - 8.70, p=0.062). Fewer patients in the PET-CT arm underwent a radical cystectomy (50% versus 65%) and with more undergoing trimodality therapy compared to those in the no PET-CT arm (36% versus 31%). 60% of patients in both arms received neoadjuvant chemotherapy. Notably, 10.2% of patients in the PET-CT arm were treated with a palliative intent, compared to 3.2% in the no PET-CT arm.
Taking these results into consideration, should nodal stage change the treatment plan for patients with MIBC, particularly those with cN1-2 disease? Dr. Giannatempo argued that there is no conclusive evidence currently regarding the management of cN+ patients, with a multi-modal approach likely key in this setting.
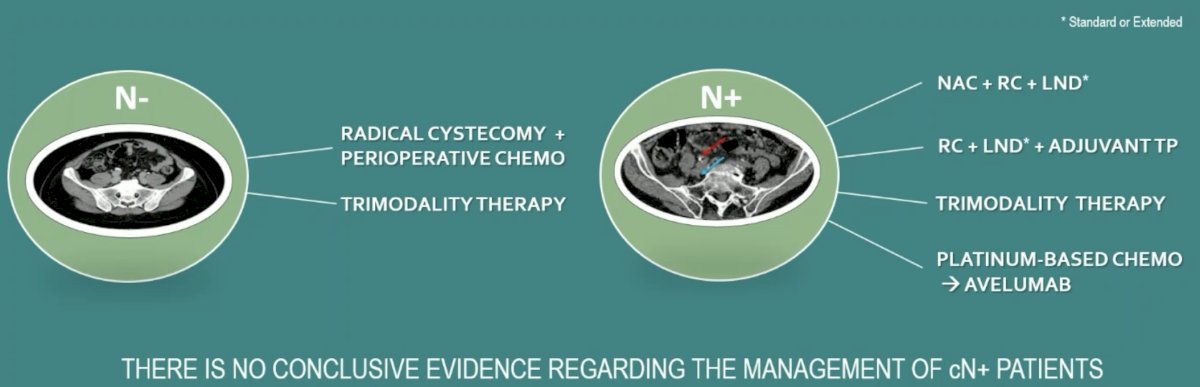
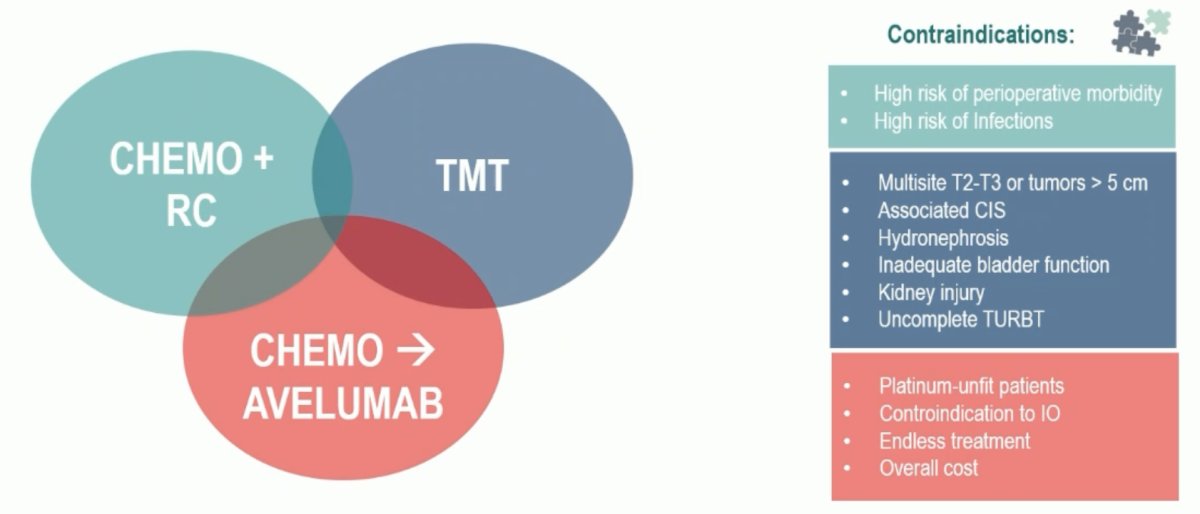
Whether patients proceed with definitive local therapy (radical cystectomy + neoadjuvant chemotherapy or trimodality therapy) or chemotherapy followed by maintenance avelumab, there are important patient conditions and physician preferences to consider, summarized below:
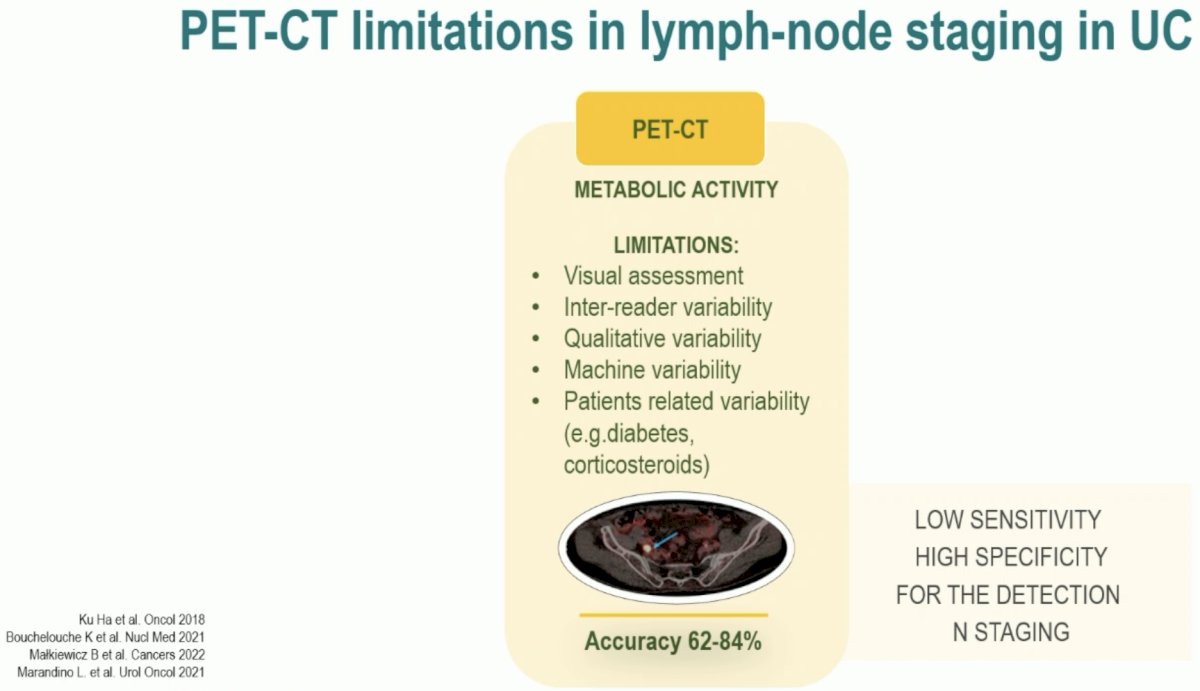
What about PET-CT as a lymph node staging tool in urothelial carcinoma? PET-CT has important limitations including:
- Limited visual assessment
- Inter-reader variability
- Qualitative variability
- Machine variability
- Patient-related variability (e.g., diabetes and corticosteroids).
As such, PET-CT may have limited sensitivity, with high specificity, for the detection of node positive disease (overall accuracy: 62 – 84%).
Looking at the treatment choices by imaging arm in this trial, use of PET-CT was associated with a 15% decrease in the use of radical cystectomy (65% to 50%), with a higher proportion of patients undergoing trimodality therapy (36% versus 31%).
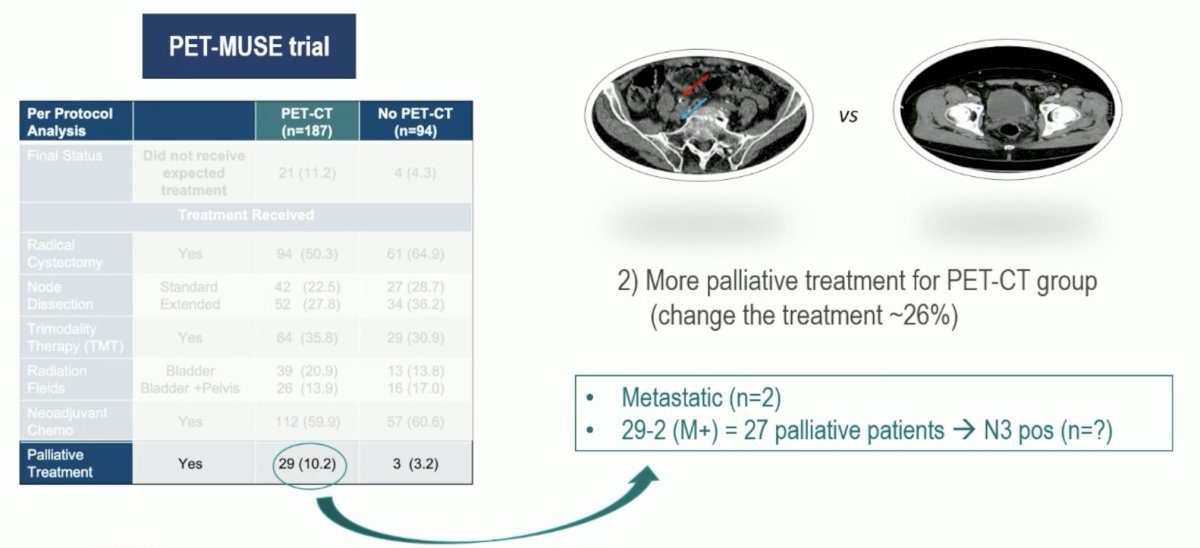
While only 2 patients (1%) were found to have metastatic disease with PET-CT, 29 (10.2%) were treated with a palliative intent. Dr. Giannatempo argued that there appears to be a discord here, given that for the 27 patients with non-metastatic disease, why was treatment with curative intent not offered? Was it possible that all of these 27 patients had cN3+ disease, a population of patients unlikely to benefit from definitive therapy? It appears unlikely, but nonetheless, it is worth further exploring the reasons for palliative instead of definitive therapy in this subgroup of patients.
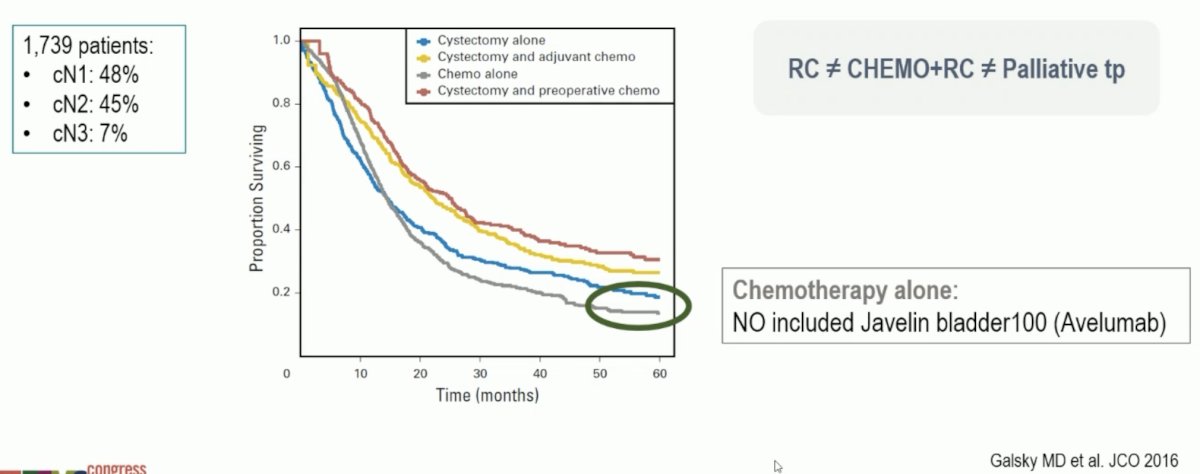
Dr. Giannatempo did acknowledge that with the emergence of avelumab as maintenance therapy following platinum-based chemotherapy for patients without disease progression, we may see more patients with cN+ disease treated with systemic therapy alone.
Were patients in the no PET/CT group undertreated or were those in the PET/CT group over-treated? While a treatment change was noted in ~17% of patients, we await additional DFS and OS data to further address this question. However, what remains clear is that patients with cN+ disease benefit from a multimodal treatment approach:
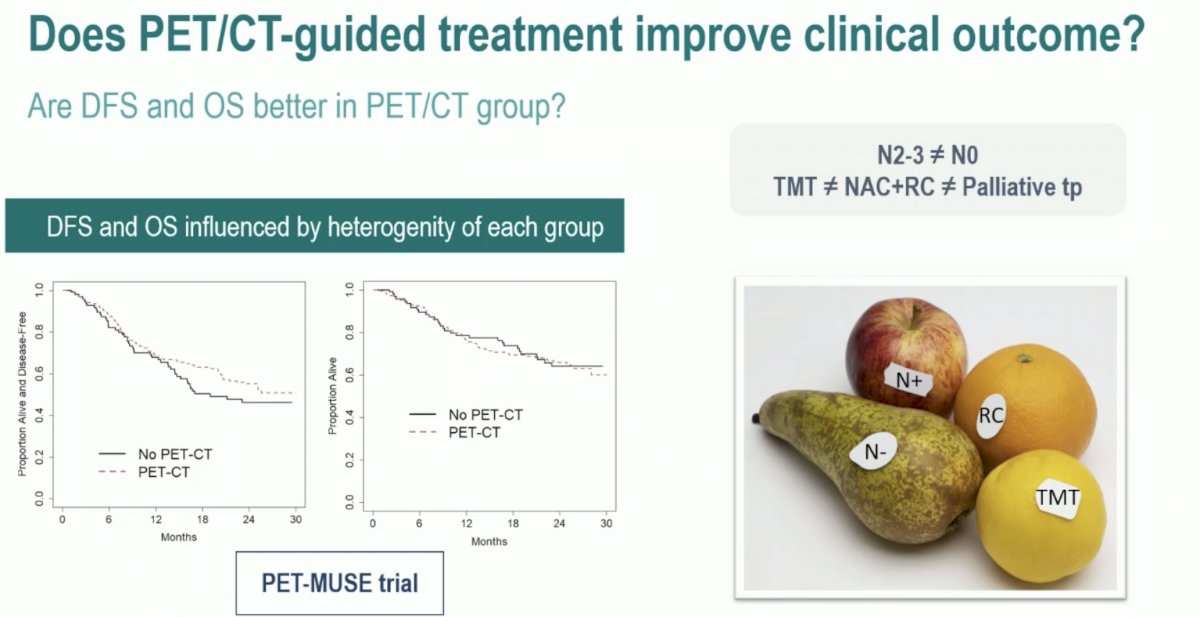
Does PET/CT -guided treatment improve clinical outcomes? This remains unclear from the PET-MUSE trial data. While DFS and OS outcomes to date appear similar between the two imaging arms, this was a heterogenous population of patients with cN0 and cN+ patients who were treated with trimodality therapy, radical cystectomy +/- neoadjuvant chemotherapy, and palliative intent.
Dr. Giannatempo’s take home messages from the PET-MUSE trial were as follows:
- Use of PET/CT imaging for staging is associated with less cystectomy with an increased utilization of trimodality therapy and palliative therapy
- Disease-free survival is partially informative, given the heterogenous population of patients treated with various approaches
- Overall survival, although influenced by many factors, shows no differences
- The PET-MUSE trial did not lead to change in management under the current guidelines (18FDG-PET not routinely used for staging in MIBC)
- The best imaging for staging nodal disease for MIBC remains unclear
Next, Dr. Giannatempo discussed the results of the THOR trial, asking the question: What is the optimal 2nd – 3rd line therapy in FGFR positive patients with metastatic urothelial cancer, noting that only ~20% of such patients have FGRG mutations?
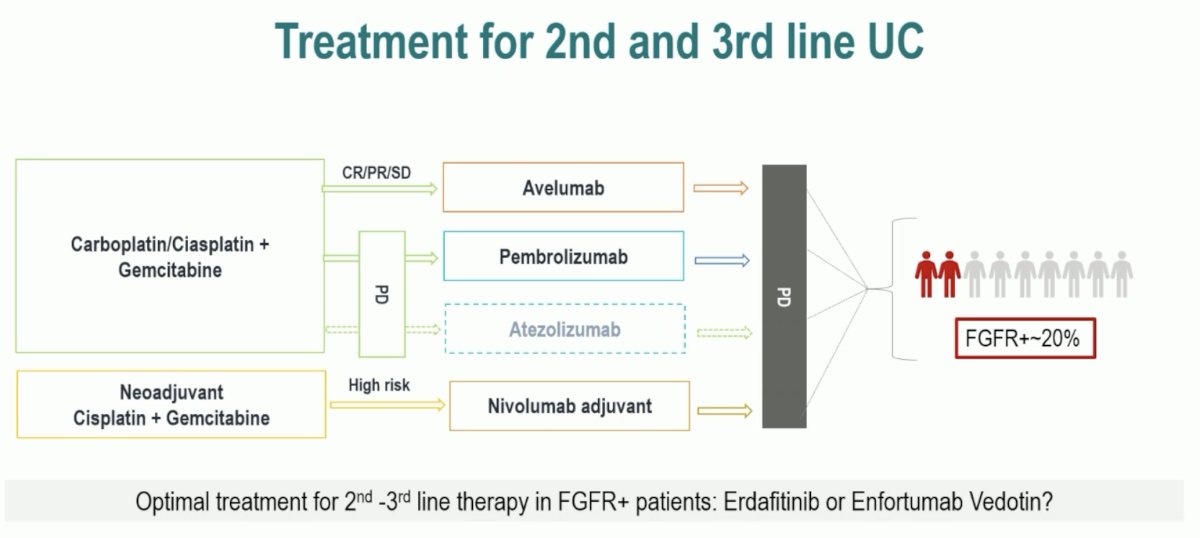
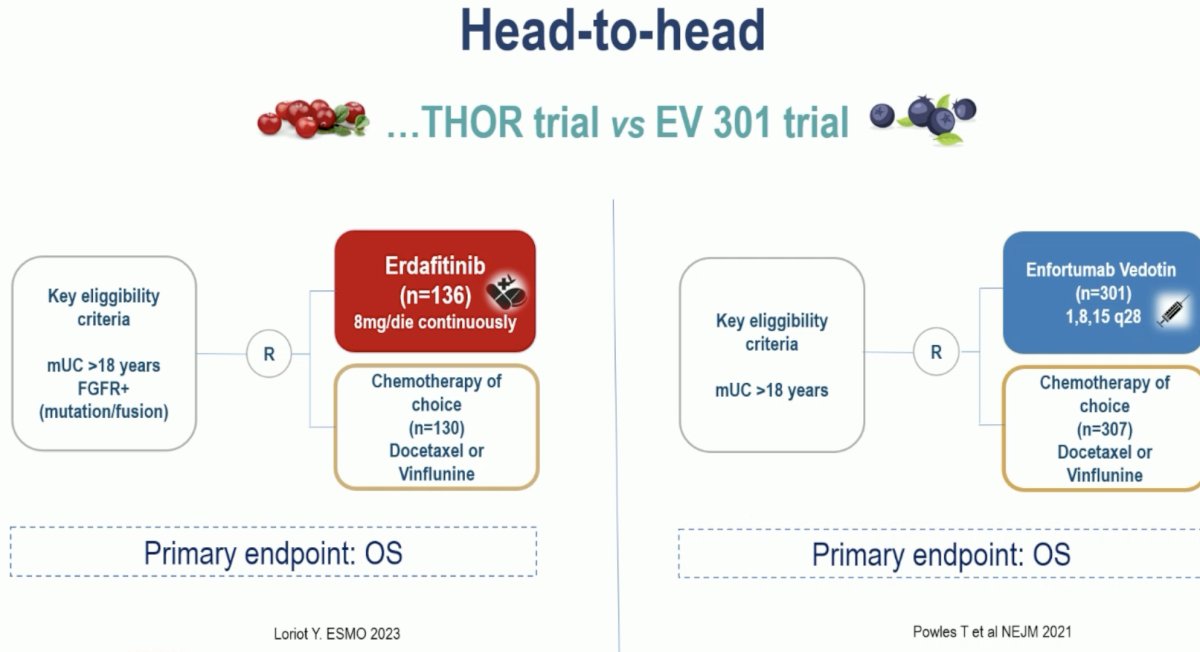
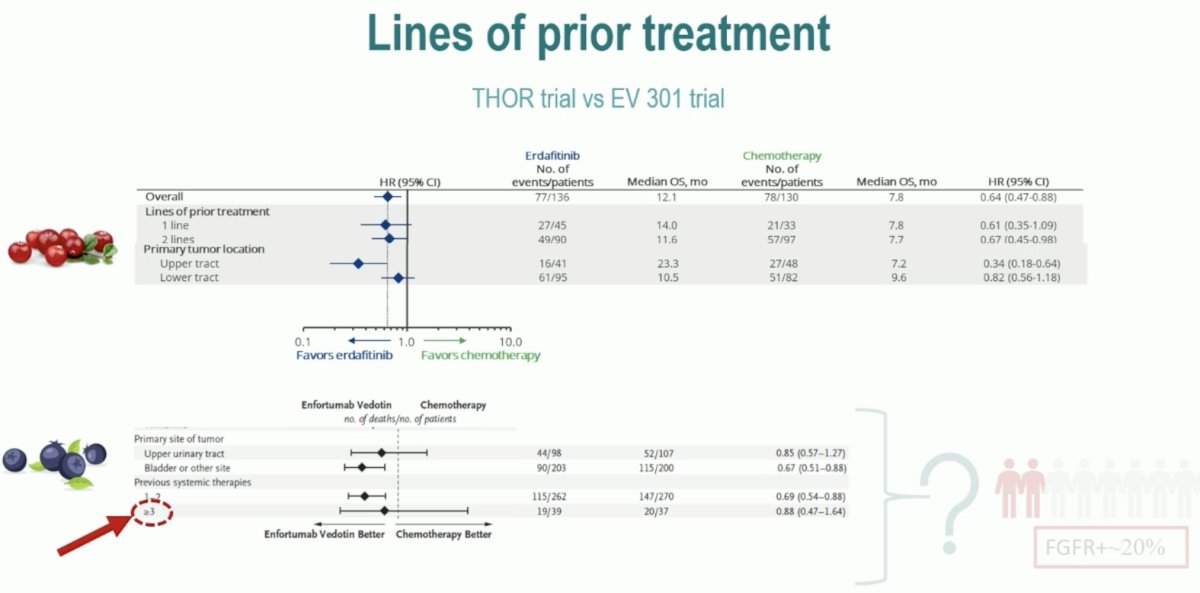
While between-trial comparisons are fraught with biases and other important limitations, Dr. Giannatempo next compared results from THOR and EV-3011 to help contextualize the available treatment options in this setting (erdafitinib and enfortumab vedotin) for FGFR+ patients.
Erdafitinib was tested in the THOR trial and included adult patients specifically with FGFR+ mutations who progressed following PD-(L)1 therapy and had received 1 – 2 prior lines of therapy. Conversely, EV-301 included ‘all-comer’ patients who had previously received platinum-containing chemotherapy and had had disease progression during or after treatment with a PD-(L)1 inhibitor.
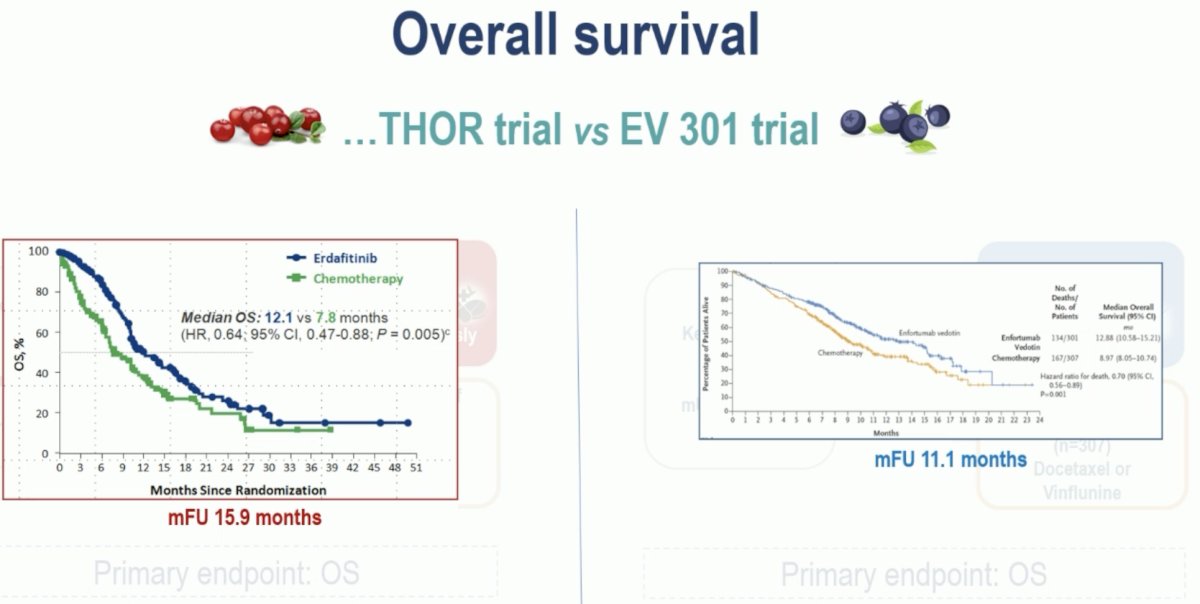
To date, the available median follow-up is longer in the THOR trial (15.9 months), compared to EV-301 (11.1 months). Both trials have demonstrated an OS benefit in the experimental arms:
- THOR: Median OS 12.1 versus 7.8 months in favor of erdafitinib (HR: 0.64, 95% CI: 0.47 – 0.88, p=0.005)
- EV-301: Median OS 12.9 versus 9.0 months in favor of enfortumab vedotin (HR: 0.79, 95% CI: 0.56 – 0.89, p=0.001)
Dr. Giannatempo highlighted that the THOR trial is the first to demonstrate that there is a benefit to 2nd – 3rd line therapy, irrespective of bone metastatic status:
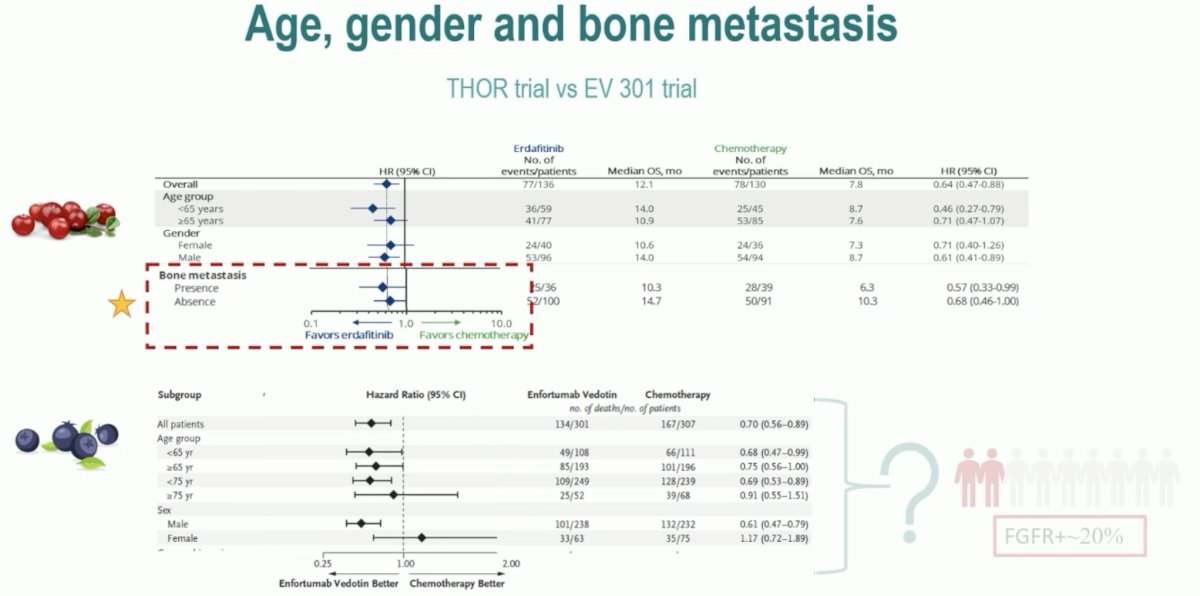
It is also important to note that THOR included patients with a less than ideal performance status (ECOG PS 2: n=11), with the EV-301 trial limited to those with an excellent performance status (ECOG 0 – 1). Conversely, while THOR was limited to patients with 1 – 2 prior lines of therapy, EV-301 included more heavily pre-treated patients receiving 3 or more prior lines of therapy.
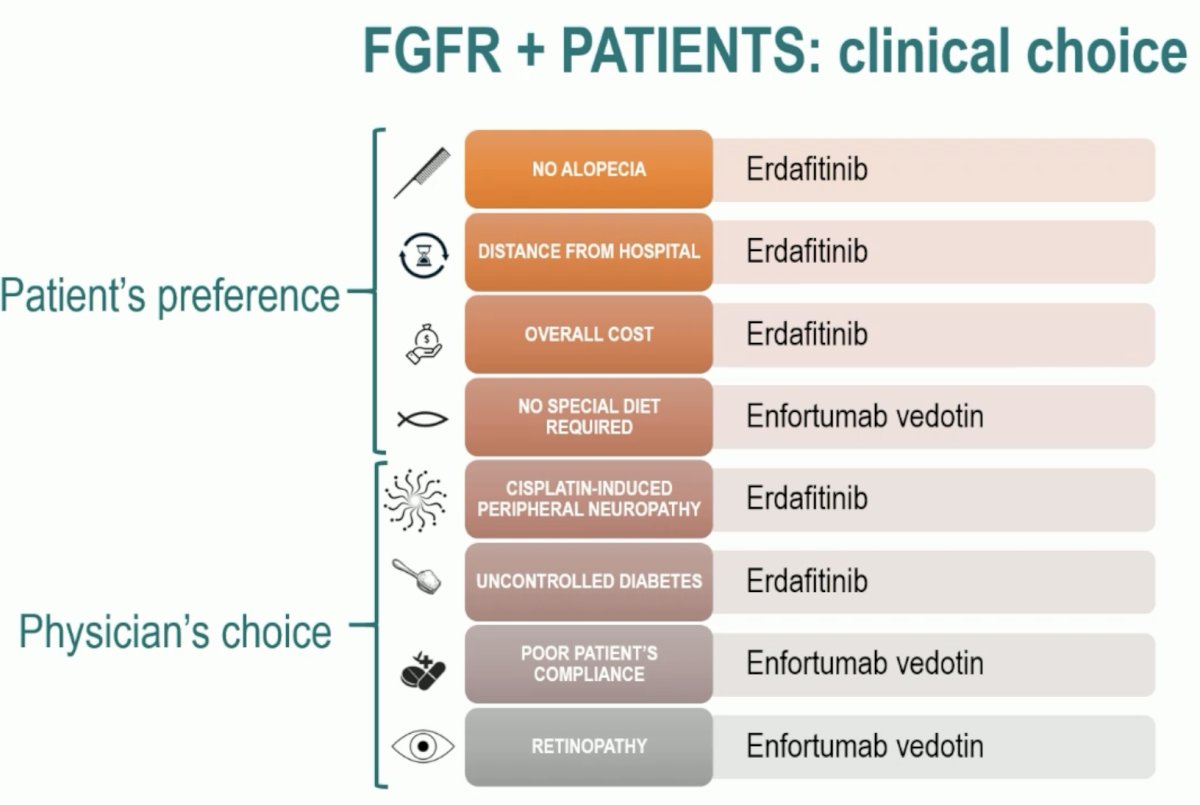
From a safety standpoint, there are differences in the adverse event profiles. Given these known differences, along with practical considerations for the administration of these treatments (erdafitinib: oral; enfortumab vedotin: intravenous), Dr. Giannatempo suggested the following rationale patient and physician-centered rationale for choosing between these two drugs:
Dr. Giannatempo concluded this discussant session as follows:
- Cross-trial comparisons between subgroup results must be avoided
- Caution is advised when interpreting subgroup analyses, particularly for upper tract disease
- We need to develop a personalized approach based on individual patient preference and physician choice
- The optimal treatment choice for FGFR+ patients in the 2nd – 3rd line setting remains unclear
- The optimal sequence for FGFR+ patients remains under investigation
1. Powles T, Rosenberg JE, Sonpavde GP, et al. Enfortumab Vedotin in Previously Treated Advanced Urothelial Carcinoma. N Engl J Med 2021 Mar 25;384(12):1125-1135.
Presented by: Dr. Patrizia Giannatempo, MD, Medical Oncology, IRCCS Istituto Nazionale dei Tumori Foundation, Milan, Italy
Written by: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 European Society of Medical Oncology (ESMO) Annual Meeting, Madrid, Spain, Fri, Oct 20 – Tues, Oct 24, 2023.
ESMO 2023: Staging of Muscle-Invasive Bladder Cancer: The Impact of PET Imaging [PET-MUSE]
ESMO 2023: Erdafitinib vs Chemotherapy in Patients With Advanced or Metastatic Urothelial Cancer With Select FGFR Alterations: Subgroups From the Phase 3 THOR Study