(UroToday.com) The 2022 ESMO annual meeting included a session focusing on PSMA biology, diagnostics, and treatment and a presentation by Dr. Karim Fizazi discussing PSMA Targeted T cell engagers. Dr. Fizazi started by noting that existing immunotherapies have minimally impacted outcomes of men with mCRPC, even though CTLA-4 inhibition was associated with excess in long-term survivors in a phase 3 trial. T cell engagers are “two-hands molecules” that engage cancer cells (identified by a target protein) and T cells, leading to (i) cancer cell lysis (independent of T cell receptor specificity), (ii) peptide presentation by the MHC system, and (iii) T cell co-stimulation signals. The following clinical efficacy data with PSMA-targeted T cell engagers is available:
- Pasotuxizumab = AMG 212 = BAY 2010112 (Amgen)
- Acapatamab = AMG 160: half-life extended (Amgen)
- HPN424 (Trispecific, Harpoon)
- JNJ-081 (Janssen)
- REGN5678 (Regeneron)
The following are PSMA x CD3 bispecifics, in particular AMG 212 and AMG 160 (both without PSMA selection):

In the phase 1 pasotuxizumab (AMG 212) trial, 47 patients with mCRPC received pasotuxizumab (subcutaneous: n = 31, 0.5-172 μg/d; cIV: n = 16, 5-80 μg/d). The subcutaneous maximum tolerated dose was 172.0 μg/d. PSA responders occurred (>50% PSA decline: subcutaneous, n = 9; cIV, n = 3), including two long-term responders:
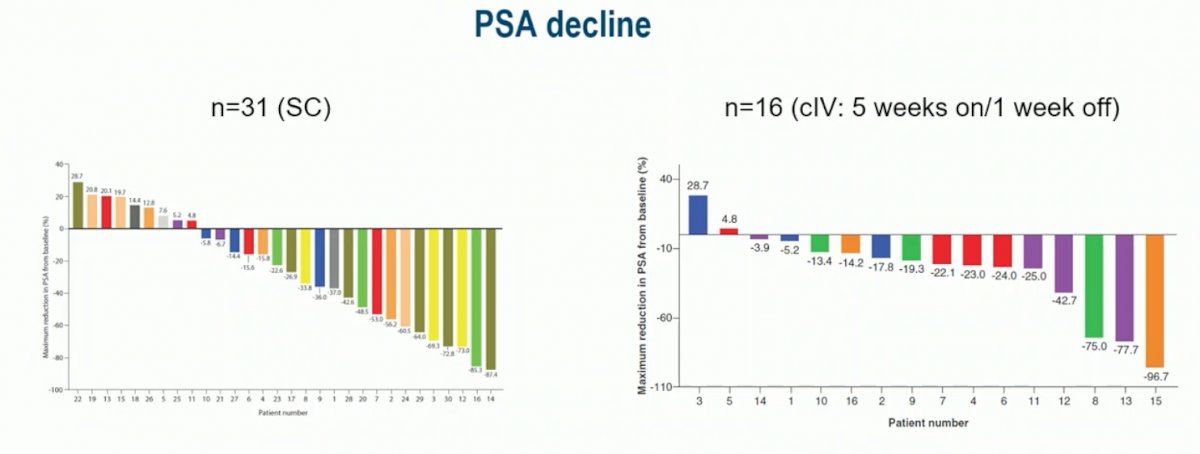
The first issue with this trial was that a neutralizing anti-drug antibody rendered subcutaneous dosing nonviable (responses non-sustained, mitigation with steroid inactive). The second issue with this trial was that continuous IV treatment was too complex to justify further development, in addition to port catheter infections.
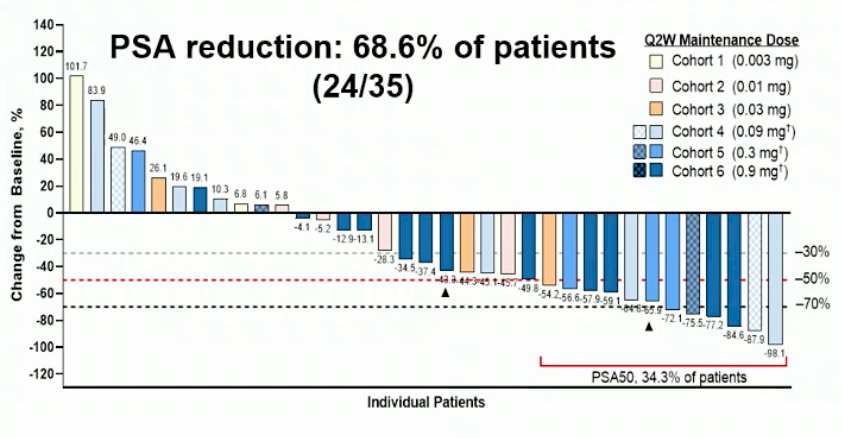
The phase I trial of acapatamab (AMG 160) was first presented at ESMO 2020, with eligible patients having mCRPC refractory to prior novel hormonal therapy and 1–2 taxane regimens, as well as evidence of progressive disease. Acapatamab was administered as a short IV infusion every two weeks at doses of 0.003–0.9 mg. At the data cutoff, the maximum tolerated dose had not been reached. AMG 160 demonstrated efficacy with long-term responses. There was a confirmed PSA response in 27.6% of patients, an unconfirmed PSA response in 11.4% of patients, and a CTC0 response in 23.1% of patients. Among patients with RECIST measureable disease, 13.3% had confirmed partial response, 6.7% had unconfirmed partial response, and 53.3% had stable disease. A summary of efficacy is as follows:

PSA reductions (best response) were dose-dependent and occurred in 24/35 (68.6%) of evaluable patients at the data cutoff of July 20, 2020, whereas PSA reductions >50% occurred in 12/35 (34/3%) of evaluable patients:
However, in addition to the above phase I trial there is one other trial testing acapatamab that is active, but unfortunately not currently recruiting. According to Dr. Fizazi this is secondary to the imbalance of potential benefit with the noted toxicity of this treatment. Additionally, secondary to concerns for cytokine release syndrome, the phase 3 acapatamab trial was recently “deprioritized,” thus it is unlikely to happen.
HPN424 is a PSMA-targeting T cell engager designed to redirect T cells to kill PSMA-expressing prostate cancer cells, and the HPN424 phase 1/2a study is evaluating HPN424 in mCRPC patients who have received > 2 prior systemic therapies. Among 89 patients, were dosed in 15 cohorts with target doses ranging from 1.3 to 160 ng/kg fixed-dose, and up to 300 ng/kg with step dosing to the target dose after the initial priming dose. Patients had received a median of 5 prior systemic regimens (a median of 2 prior novel hormonal agents), with 73% having received prior chemotherapy for mCRPC. Reduction in circulating tumor cells was seen in 36 of 64 patients (56%) with measurable circulating tumor cells at baseline, including 14 patients who had a CTC0 response. Fifteen of 74 patients with at least 6 months of follow-up have remained on treatment beyond 24 weeks, and one patient experienced confirmed partial response at 160 ng/kg. Fifteen of 74 patients (20%) with >=1 post-baseline value had PSA decreases from baseline ranging from -2% to -76%, including four patients with PSA50 response and two patients with PSA30 response. In chemotherapy-naïve patients, 6 of 20 (30%) showed PSA declines post-baseline, including three with PSA50 and one with PSA30 response. Eight of 17 patients (47%) chemotherapy-naïve patients in the castrate-resistant state with at least six months of follow-up have remained on treatment beyond 24 weeks. There were 41 patients of 89 (46%) that had measurable disease at baseline, including 34 patients with >=1 post-treatment protocol scheduled disease assessment. Among these 34 patients, the sum of target lesions in 19 patients (56%) remained stable or showed a reduction, including 1 confirmed partial response.
The phase I dose-escalation study of JNJ-081 included men with mCRPC who had previously progressed on novel oral androgen therapies such as abiraterone, enzalutamide, or apalutamide. Prior chemotherapy was allowed, but not required. There were 39 patients received doses of study drug across 10 cohorts ranging from 10 ug/kg to 3 ug/kg IV and 3 ug/kg to 60 ug/kg subcutaneous. Given concern for cytokine release syndrome, the premedication regimen included high-dose corticosteroids. Preliminary evidence of efficacy included two subjects with PSA decreases of greater than 50%, both of whom received 55 ug/kg doses. No radiographic responses were observed

Dr. Fizazi notes that the main issues with JNJ-081 are cytokine response syndrome, likely inactivity with IV administration, transient PSA responses with subcutaneous delivery, and antidrug-antibodies in 67% of patients, ultimately leading to deprioritization in favor of next generation bispecifics.
Dr. Fizazi highlighted that on August 3, 2022, there was a press release regarding REGN5678 (PSMA x CD28) + PD-1 inhibition. The first clinical data from the ongoing phase 1/2 trial show dose-dependent anti-tumor activity for REGN5678 when combined with standard dose cemiplimab, suggesting potential to overcome mCRPC resistance to PD-1 inhibition. Additionally, anti-tumor activity correlated with immune-related adverse events. At the next three dose levels (cohorts 6-8) evidence of dose-dependent anti-tumor activity was generally seen within 6 weeks of starting combination treatment as follows:
- Cohort 6: 1 of 4 patients experienced a 100% decrease in PSA and a complete response in target lesions based on RECIST 1.1 criteria. The patient discontinued therapy due to a grade 3 immune-related adverse event of the skin, however the patient has maintained the 100% decrease in PSA and complete response in target lesions for approximately 10 months to date per investigator report
- Cohort 7: 3 of 8 patients experienced decreases in PSA of >99%, 44%, and 22%. Two of these three patients had a grade 3 adverse event (aseptic encephalitis and seizure, respectively, both of which have resolved)
- Cohort 8: 3 of 4 patients experienced decreases in PSA of >99%, >99%, an 82%. Of the two patients with >99% PSA reductions, one experienced a grade 3 case of mucositis (resolved) and the other experienced a grade 3 case of acute inflammatory demyelinating polyradiculopathy (ongoing)
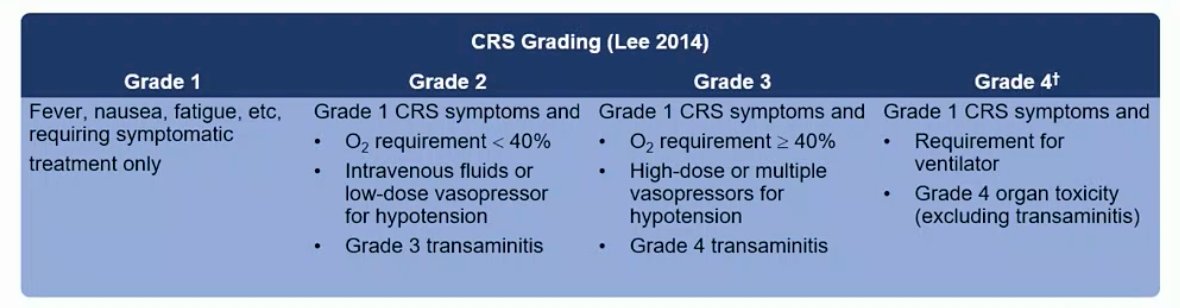
With regards to cytokine release syndrome, typical symptoms include chills/fever, hypotension/tachycardia, major fatigue, and hypoxemia. Mitigation strategies include step dose regimen, prophylactic hydration, corticosteroids, and subcutaneous injections. When cytokine release syndrome is severe, patients may need IV fluids, vasopressors in the ICU, mechanical ventilation, and anti-IL-6 (tocilizumab). The Lee cytokine release syndrome grade criteria is as follows:
Dr. Fizazi notes that the benchmark for PSMA bispecifics for efficacy and safety is the VISION trial.1 Lu-PSMA is generally safe and well tolerated with only 8.1% of patients experiencing grade 3-5 adverse events. So, where do we currently stand with PSMA bispecifics with Lu-PSMA as a benchmark?
- Toxicity – cytokine release syndrome is clearly a limitation for development
- Obviously not enjoyable for patients
- Outpatient use of PSMA bispecifics is challenging
- Requires an ICU nearby
- Hopefully will be seen less with 3rd generation bispecifics
- Efficacy
- Currently based on weak endpoints (PSA, etc)
- Hard to compare with that of Lu-PSMA (no RCT)
- Anecdotal evidence of efficacy (PSA decline) with PSMA-targeted bispecific post progression on Lu-PSMA (more data is needed)
Indeed, we are looking for 3rd generation PSMA x CD3 bi/trispecifics to reach this benchmark, with new constructs designed to reduce cytokine release without compromising cancer cell killing/extend the half life. Dr. Fizazi concluded by highlighting examples of other targets and T cell engagers potentially relevant for prostate cancer treatment:
- DLL3 in NEPC (AMG 757)
- STEAP1 (AMG 509)
- Human Kallikrein-2 (KLK2) (Janssen)
- TMEFF2 (Janssen): ESMO 2022 poster
- PD-1 x CTLA-4 (Vudalimab = XmAb20717)
Presented by: Karim Fizazi, MD, Ph.D., is a medical oncologist, Head of the Department of Cancer Medicine at the Institute Gustave Roussy (IGR), Villejuif, France and a Professor in Oncology at the University of Paris
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 European Society for Medical Oncology (ESMO) Annual Congress, 9-13 September 2022.
References:
- Hummel HD, Kufer P, Grullich C, et al. Pasotuxizumab, a BiTE immune therapy for castration-resistant prostate cancer: Phase I, dose-escalation study findings. Immunotherapy. 2021 Feb;13(2):125-141.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.