Dr. Pal began by highlighting the incredible progress that has been made in advanced RCC over the past five years. In this year’s ESMO alone, there were five phase III RCTs presented.
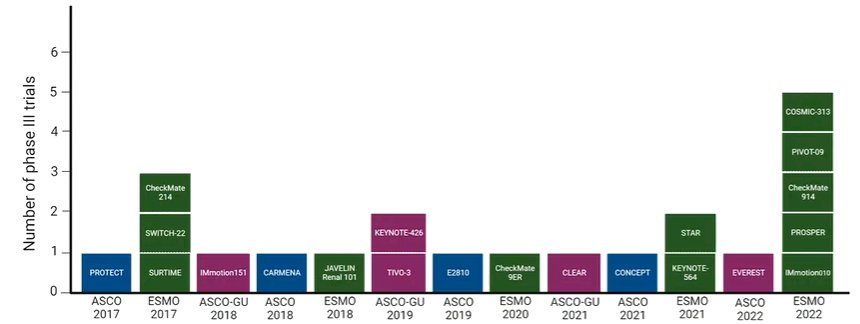
In spite of this dramatic progress over the past few years, the COSMIC-313 trial stands out through a number of relevant “firsts” including:
- The first phase 3 clinical trial to use a contemporary control arm (nivolumab/ipilimumab)
- The first phase 3 trial comparing triplet to doublet therapy in aRCC
- Together, the first trial of its kind to meet its primary endpoint.
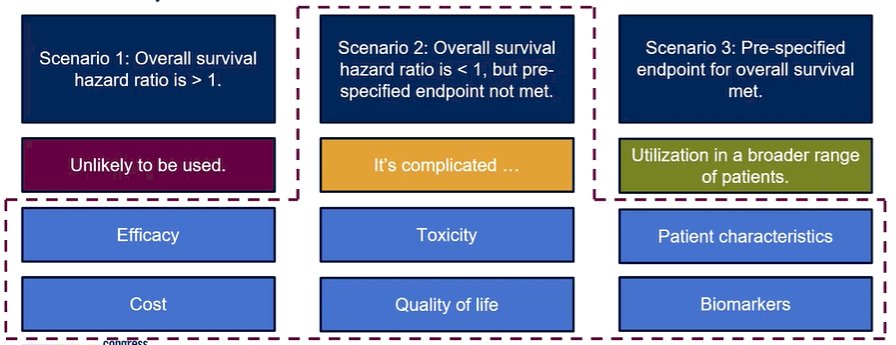
However, Dr. Pal acknowledged the “elephant in the room”: we have not yet seen overall survival data. In the case of poorer overall survival in the triplet arm, he suggested that this approach would be unlikely to be clinically used. In the case of a significant benefit in overall survival of the triplet approach, he anticipated utilization in a broader range of patients with individualized treatment decision-making on the basis of efficacy, toxicity, patient characteristics, cost, quality of life, biomarker, and other considerations. The somewhat difficult intermediary scenario in which overall survival is improved compared to doublet but fails to meet the pre-specified endpoint. In this situation, use is somewhat complicated and may be driven by subgroup analyses.
Given the lack of OS data available, he raised the question as to whether we can make decisions in the absence of this data. First, he noted that there is precedent in other disease. Most recently, adjuvant nivolumab was approved (by both the US FDA and European Commission) in urothelial cancer on the basis of demonstrated improvements in disease-free survival, without available data on overall survival yet.
Moving to clinical decision-making, Dr. Pal then compared results from the COSMIC-313 trial to the other recent trials in first-line aRCC including CheckMate 214, Keynote 426, CheckMate 9ER, and CLEAR. While there are clear issues with cross-trial comparisons, the impulse to do these is natural.
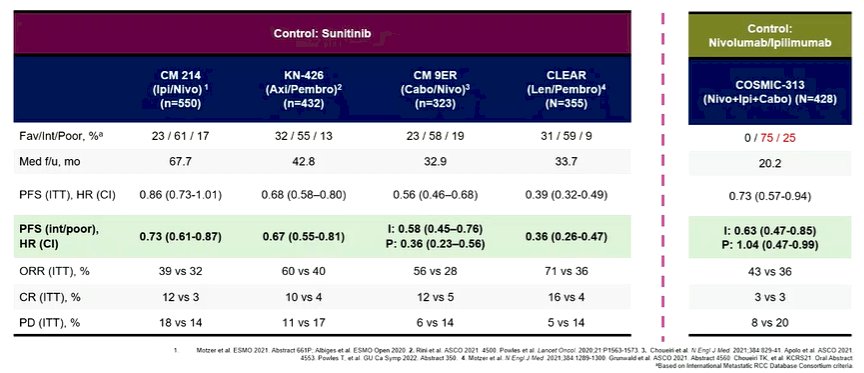
In the context of COSMIC-313 he cautioned particularly against doing this as, while the other trials all used the same control approach, the control arm of COMSIC-313 received combined immune checkpoint inhibition. However, taken on their own, he emphasized that COSMIC-313 met the PFS endpoint with an interesting signal of benefit, particularly in the intermediate risk subset. Additionally, there was less primary progressive disease. However, the response rate was only marginally improved in the triplet, as compared to doublet, arm and there were low complete response rates in both arms.
To explain some of these results, he examined whether there may be differences in the patients enrolled in this trial. Both patients and investigators felt that patients on a triplet therapy trial would be likely to have more aggressive disease than those evaluating doublets. Certainly, compared to CheckMate 214, patients on COSMIC-313 were less likely to have had prior nephrectomy though the distribution of IMDC risk and sites of metastases were comparable.
Dr. Pal then considered whether additive toxicity may get in the way of treatment. Again relying on a cross-trial comparison with CheckMate 214, CheckMate 9ER, and the two arms of COSMIC-313, he noted that the combination arm had somewhat higher rates of grade 3-4 events, with a particularly increased rate of increased liver enzymes.
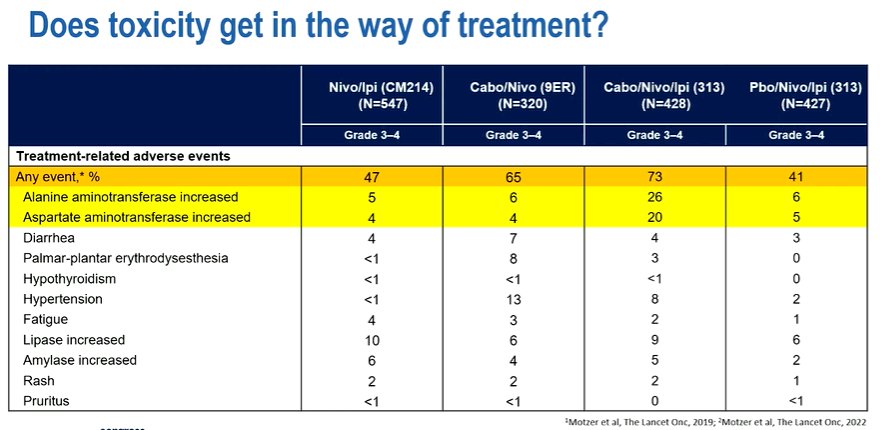
Additionally, a lower proportion of patients in the triplet arm were able to receive four doses of ipilimumab (58% vs 73% or 79% in the doublet arms of the COSMIC-313 and CheckMate 214 trials) and a greater proportion required steroids (58% vs 29% or 35% in the doublet arms of the COSMIC-313 and CheckMate 214 trials). Taken together, Dr. Pal noted that grade 3 or 4 toxicity was substantially higher with the triplet approach. However, due to the overlapping toxicity, it is hard to definitively attribute these to either the TKI or the IO therapy. Either way, the was potentially early discontinuation of ipilimumab and more frequent use of steroids.
Dr. Pal then highlighted efficacy data, examining the waterfall plots. He first noted that we see the expected, and desired, left shift in the plots with a substantially higher proportion of patients having any disease reduction. However, looking at patients who had “deep responses”, there are actually fewer patients with these declines of more than 60% and more than 80%. Looking forward, work from Dr. Suarez has previously shown that depth of response may have a prognostic effect.
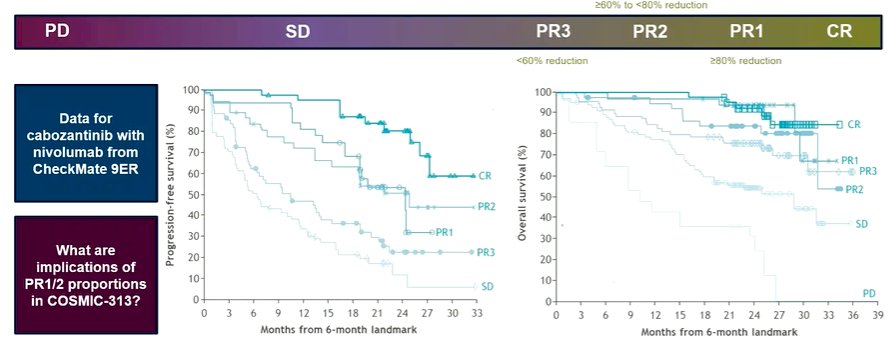
Thus, it will be interesting to see how this translates to the data from COSMIC-313. Moving forward, Dr. Pal highlighted multiple approaches. First, there are trials evaluating other triplet combinations as well as those examining a risk-adapted approach. Looking forward, Dr. Pal considered that the bar set by the TKI + IO combination is quite high. Thus, improving oncologic endpoints without considerable toxicity may be difficult.

While theoretical, he noted that there is likely a real risk of trading off safety for efficacy as we move to higher numbers of agents. Thus, instead, a more targeted approach using biomarker selection may allow for more rational treatment intensification.
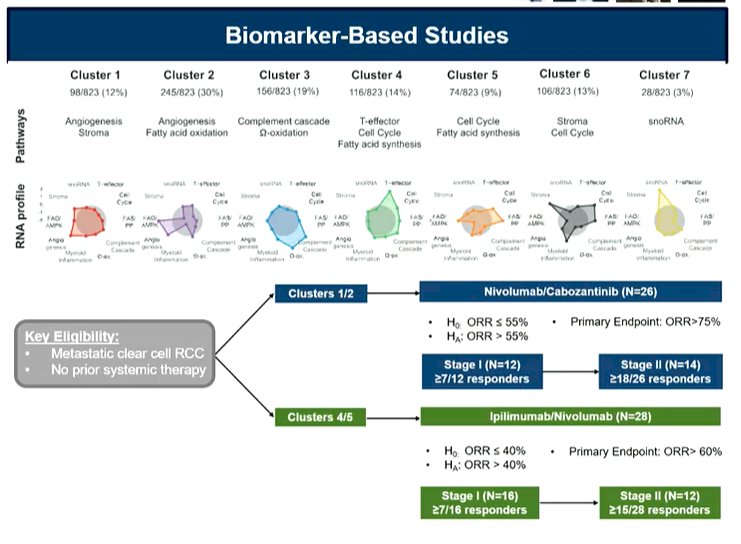
There are myriad biomarker-driven approaches in clear cell RCC. However, he noted that the best biomarker work has been derived from the IMMotion150, IMmotion151, and JAVELIN Renal 101 trials. Ironically, these are based on treatment regimes that failed to demonstrate overall survival benefit and are not routinely used in the clinic.
An alternative approach is to find treatment approaches with non-overlapping toxicity such that more treatment can be given without risks to safety. One such approach, driven by his own work, is the use of a live bacterial product to mediate the gut microbiome. In phase I data, this provided promising data with improved PFS and response rate.
Concluding, he noted that COSMIC-313 is a trial of first, demonstrating the benefit of a triplet approach against a current standard of care control arm. There are however many unanswered questions that remain to be addressed as we look forward to clinical use.
Presented by: Sumanta K. Pal, MD, City of Hope, Duarte, CAWritten by: Christopher J.D. Wallis, University of Toronto Twitter: @WallisCJD during the 2022 European Society for Medical Oncology (ESMO) Annual Congress, 9-13 September 2022.