A number of other randomized trials have demonstrated that immune checkpoint inhibitors are effective in advanced RCC. In the first-line setting, immune checkpoint inhibitor combination therapy has become standard of care. Bempegaldesleukin is a pegylated IL-2 prodrug, designed with the intent to preferentially bind to IL-2Rβγ. In the PIVOT-09 trial, the investigators assessed the efficacy of bempegaldesleukin plus nivolumab compared to an investigators choice of sunitinib or cabozantanib (NCT03729245).

The authors enrolled adults with measurable and untreated advanced/metastatic clear-cell RCC. Once enrolled, patients were randomized 1:1 (stratified by IMDC risk score and TKI choice) to receive bempegaldesleukin IV 0.006 mg/kg plus nivolumab 360 mg q3w OR either sunitinib 50 mg PO daily for 4 weeks followed by 2 weeks off, or cabozantinib 60 mg PO daily. The primary study endpoints were objective response rate (ORR) by blinded independent central review (BICR) and overall survival (OS) in patients with IMDC intermediate (I) or poor (P) risk, and in IMDC all-risk disease. With an overall study α of 0.05 (2-sided), the authors allocated 0.001 for ORR and 0.049 for OS.
The authors enrolled a total of 623 patients of whom 514 had IMDC intermediate or poor risk disease and 109 had IMDC favorable-risk disease. Among 623 randomized patients, 616 patients (IMDC intermediate/poor n=509; IMDC favorable n=107) received at least one dose of their allocated treatment (sunitinib n=221; cabozantinib n=85).
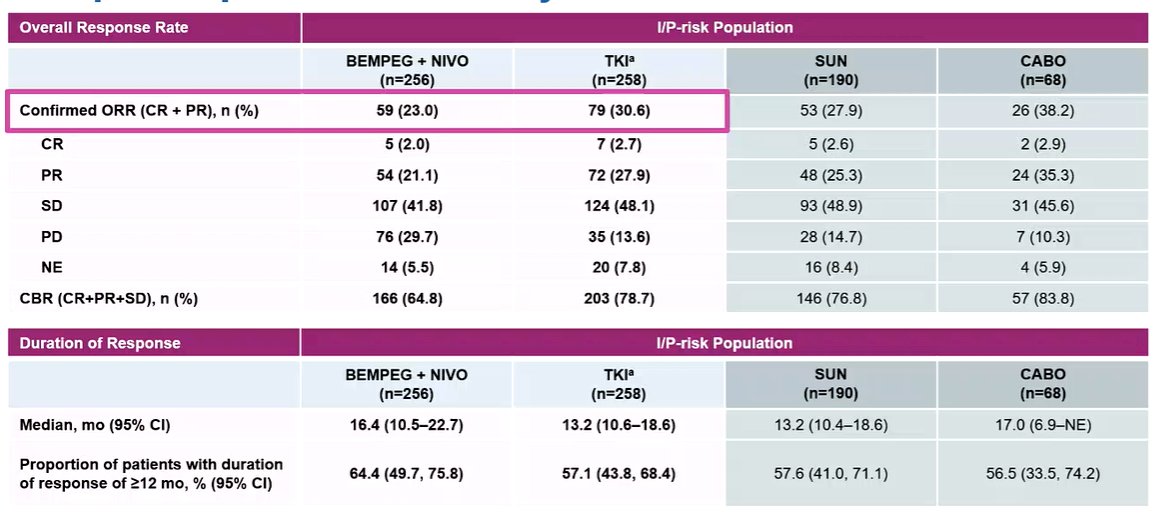
Among patients with intermediate or poor risk disease, after a median duration of follow-up of 15.5 months, the ORR was 23.0% for bempegaldesleukin plus nivolumab vs 30.6% for the TKI arm. As highlighted in the table below, complete response rates and clinical benefit rates were higher in the TKI arm. However, among responders, the duration appeared somewhat longer in the bempegaldesleukin plus nivolumab arm.
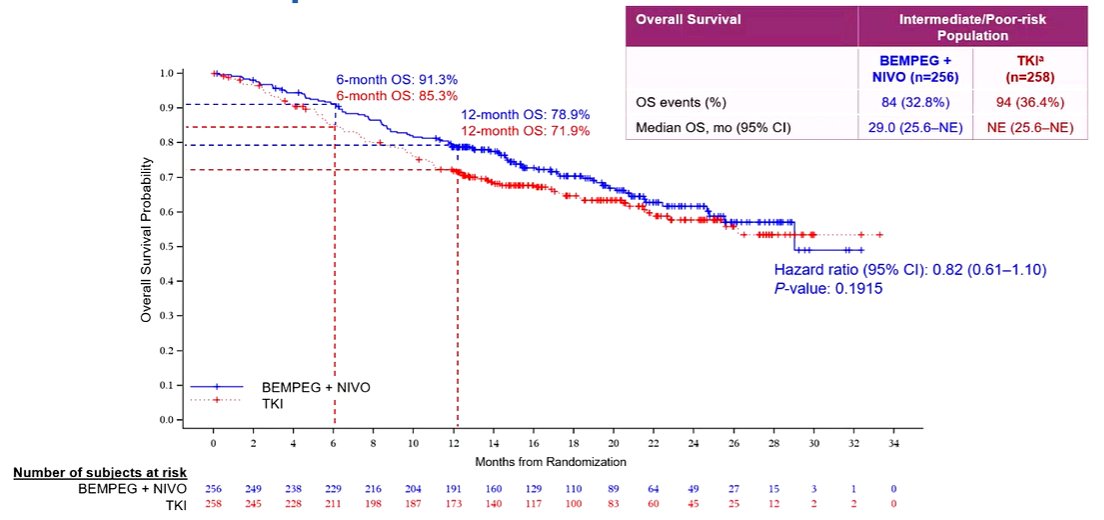
In addition to lower observed response rates, median OS in subset of patients with IMDC intermediate/poor risk disease was 29.0 months for bempegaldesleukin plus nivolumab and not reached for the TKI arm (HR=0.82, 99% CI: 0.56-1.21). OS was not significantly different, with p-value of 0.19 did not pass the pre-specified alpha of 0.01 at the interim analysis.
Subgroup analyses demonstrated relatively homogenous effect. However, there was evidence of a greater benefit of the combined treatment approach among patients with baseline PD-L1 of 1% or greater.

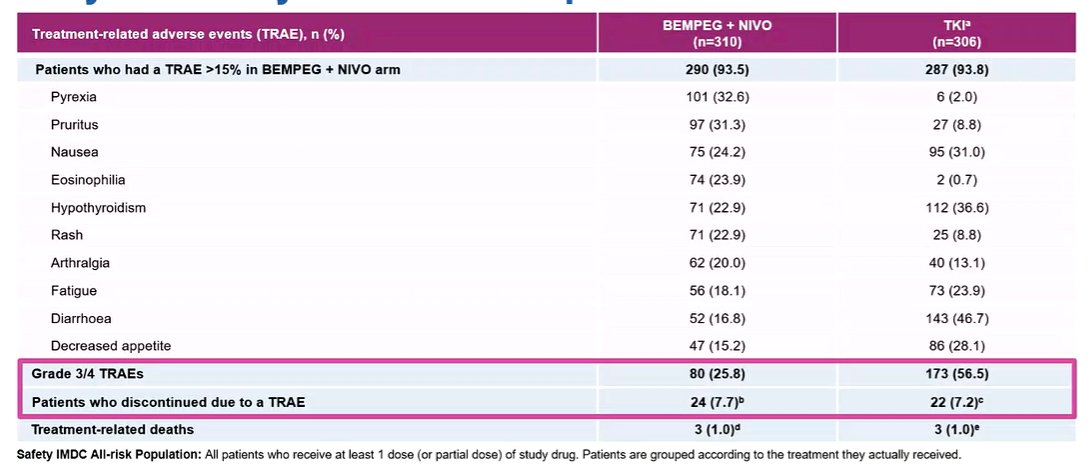
Among all comers, regardless of IMDC risk group, the most common treatment-related adverse events (TRAEs, >20%) of any grade in bempegaldesleukin plus nivolumab arm were pyrexia (32.6%), pruritus (31.3%), nausea (24.2%), eosinophilia (23.9%), hypothyroidism (22.9%), rash (22.9%), and arthralgia (20.0%). Grade ≥3 TRAEs occurred in 83 pts (26.8%) and 24 pts (7.7%) discontinued due to TRAEs for bempegaldesleukin or nivolumab. Grade 5 TRAEs occurred in 3/310 pts (1.0%).
Thus, the authors conclude that, in first line treatment of advanced/metastatic clear-cell RCC, bempegaldesleukin plus nivolumab did not improve outcomes vs investigator’s choice of TKI.
Presented by: Nizar Tannir, MD, Department of Genitourinary Medical Oncology, Division of Cancer Medicine, MD Anderson Cancer Center, Houston, TXWritten by: Christopher J.D. Wallis, University of Toronto Twitter: @WallisCJD during the 2022 European Society for Medical Oncology (ESMO) Annual Congress, 9-13 September 2022.