(UroToday.com) The Realizing Potential Combination and Personalized Therapy educational session at the European Society for Medical Oncology (ESMO) 2021 congress included a presentation by Dr. Toni Choueiri discussing whether there is an optimal first-line combination approach for metastatic renal cell carcinoma (RCC). The current first-line combination therapies that are FDA approved are listed as follows:

Dr. Choueiri started his discussion by highlighting IO + IO combination therapy (PD-1 + CTLA4 inhibitors). The CheckMate 214 trial tested nivolumab + ipilimumab in newly diagnosed clear-cell RCC; the trial schema for CheckMate 214 is as follows:1
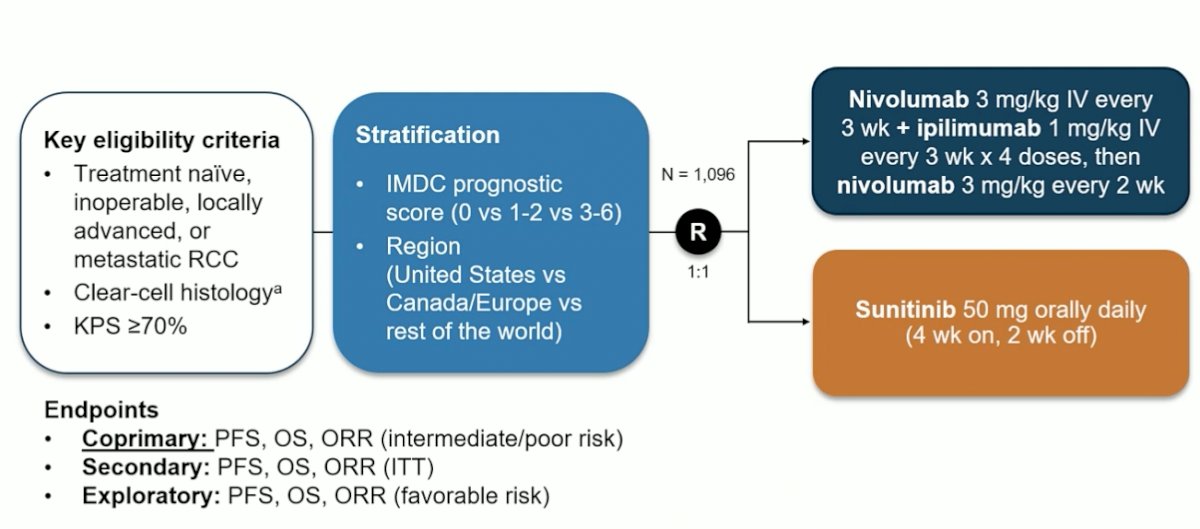
Now with a minimum of 60 months follow-up (presented at ESMO 2021), the combination of nivolumab + ipilimumab has shown a durable PFS and OS benefit (HR 0.68, 95% CI 0.58-0.81) among intermediate/poor-risk patients:

Dr. Choueiri then discussed the multitude of IO + VEGF combination therapies. There is a rationale for combining immunotherapy with VEGF-targeted therapy, including (i) normalization of the tumor vasculature for increased T-cell tumor infiltration, (ii) establishing an immune-permissive tumor microenvironment by decreasing MDSC and Treg populations, (iii) promotion of T-cell priming and activation via dendritic cell maturation. As follows are the four trials that have been approved in the first-line IO + VEGF combination therapy disease space:
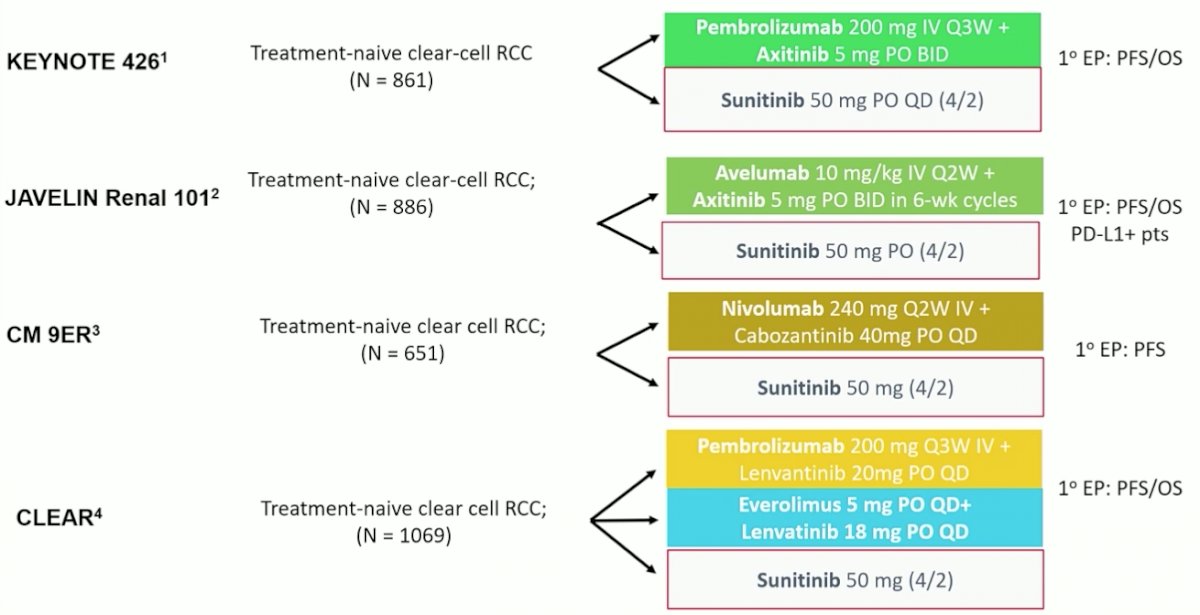
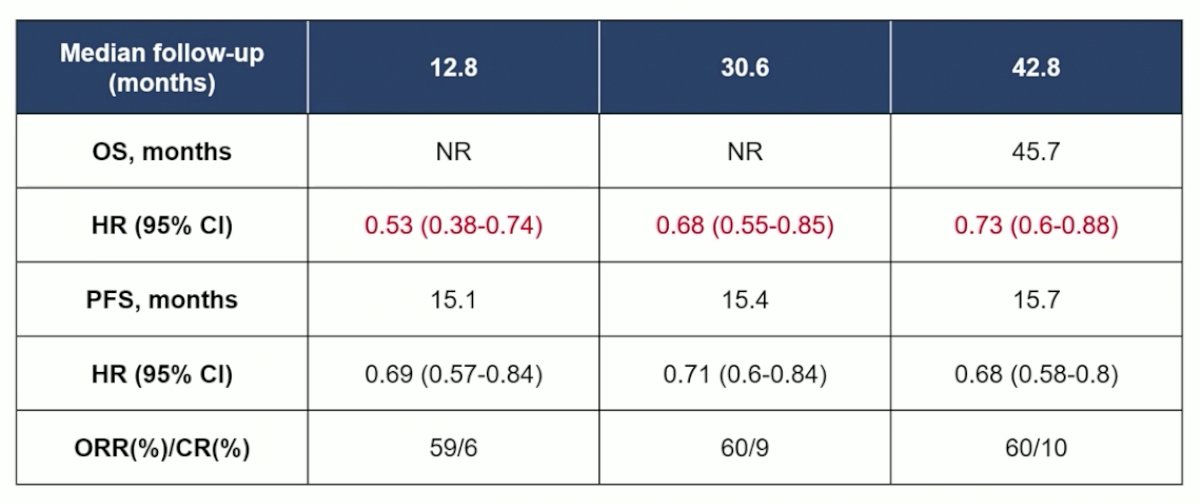
In KEYNOTE-426, 861 patients with metastatic clear cell RCC, predominately with intermediate or poor-risk disease, who had not previously received systemic therapy were randomized to pembrolizumab + axitinib or sunitinib and followed for the co-primary endpoints of overall survival and progression-free survival.2 While median OS was not reached, patients who received pembrolizumab + axitinib had improved OS (HR 0.53, 95% CI 0.38 to 0.74) and progression-free survival (HR 0.69, 95% CI 0.57 to 0.84), as well as overall response rate. These results were consistent across subgroups of demographic characteristics, IMDC risk categories, and PD-L1 expression level. Grade 3 to 5 adverse events were somewhat more common among patients getting pembrolizumab and axitinib, though rates of discontinuation were lower. The most recent updated follow-up of this trial was presented at ASCO 2021, showing a durable survival benefit for pembrolizumab + axitinib (HR 0.73, 95% CI 0.60-0.88):
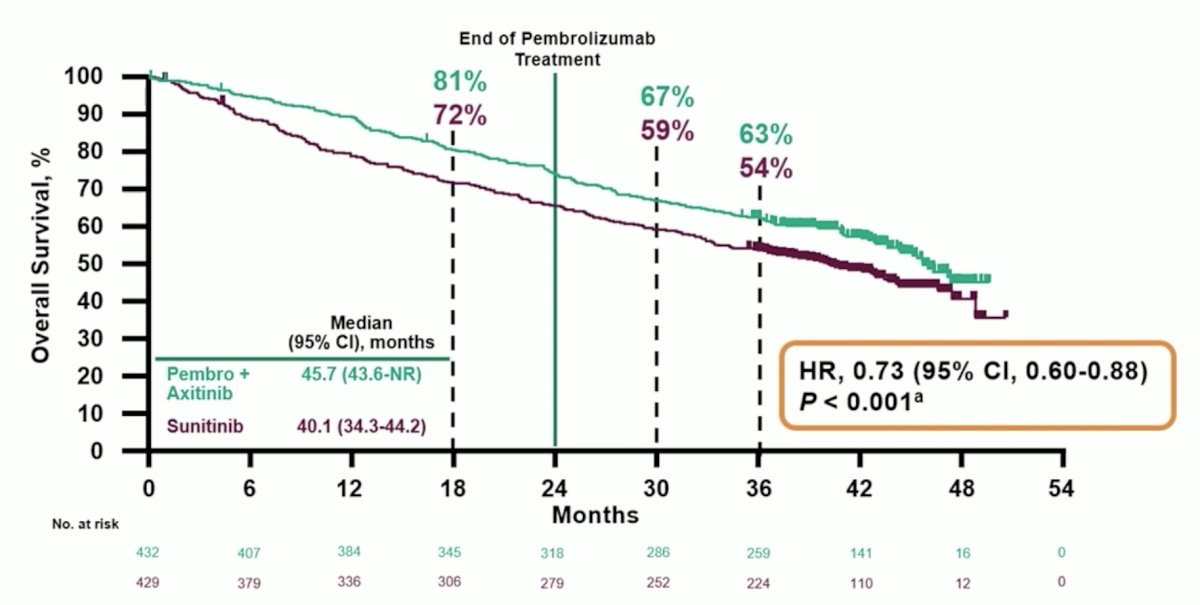
Although the PFS and ORR results have remained stable for pembrolizumab + axitinib with longer follow-up, the OS benefit has become less impressive (but still significant) likely secondary to secondary therapy following the trial period:
In JAVELIN Renal 101, 886 patients were randomized to avelumab + axitinib or sunitinib.3 In this trial, the primary endpoints were PFS and OS in patients with PD-L1 positive tumors. Notably, 560 of the 886 patients had PD-L1 positive tumors. Among the PD-L1 positive subgroup, progression-free survival (HR 0.61, 95% CI 0.47 to 0.79) was improved in patients receiving avelumab + axitinib compared to sunitinib while OS did not significantly differ (HR 0.82, 95% CI 0.53 to 1.28). In the overall study population, progression-free survival was similarly improved, as compared to the PD-L1 positive population (HR 0.69, 95% CI 0.56 to 0.84). Since this trial has not shown an OS benefit to date, utilization of avelumab + axitinib is less common than the other IO + VEGF combination therapies.
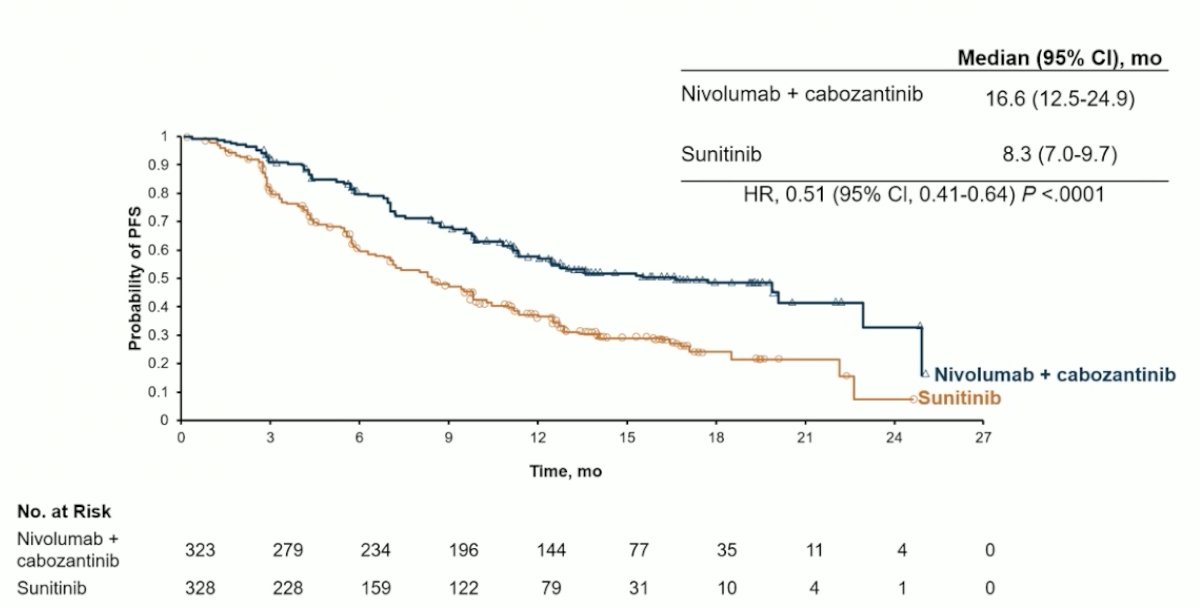
In the CheckMate 9ER trial, 651 patients were randomized in a 1:1 fashion to nivolumab + cabozantinib or sunitinib, in the first-line treatment of patients with advanced or metastatic renal cell carcinoma, with randomization was stratified by IMDC risk score, tumor PD-L1 expression, and region.4 The primary outcome was progression-free survival with overall survival, objective response rate, and toxicity comprising important secondary outcomes. Over a median follow-up of 18 months, median progression-free survival was significantly longer among those randomized to nivolumab + cabozantinib (16.6 months) than those randomized to sunitinib (8.3 months), with a relative difference of 49% (HR 0.51, 95% CI 0.41 to 0.64):
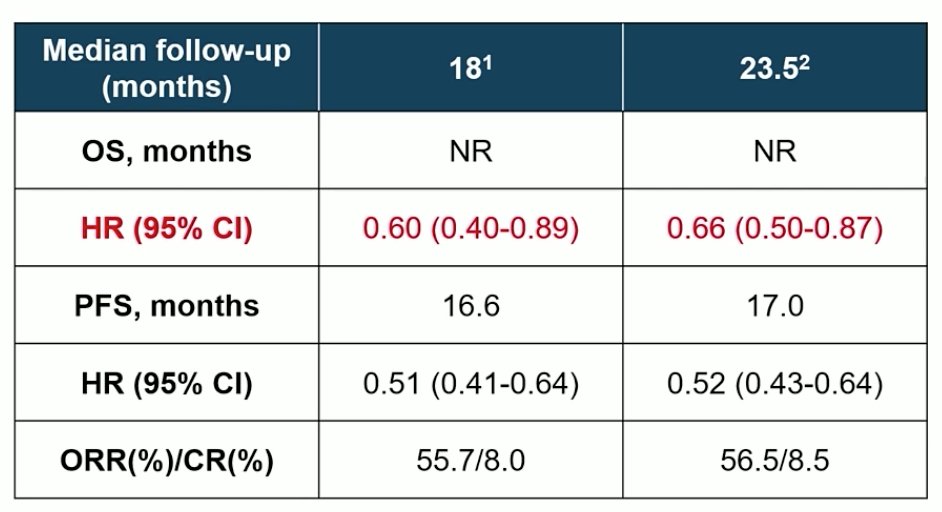
OS was not reached in either arm (HR 0.60, 98.89% CI 0.40 to 0.89). Notably, these benefits were seen consistently across pre-specified subgroups defined according to IMDC risk categories and PD-L1 expression. Any grade treatment related adverse events were common in both groups: 96.6% among those receiving nivolumab + cabozantinib and 93.1% among those receiving sunitinib. High-grade events (grade 3 or greater) were somewhat higher among those receiving nivolumab + cabozantinib (60.6% vs 50.9%). One grade 5 event occurred in the nivolumab + cabozantinib arm while 2 occurred in the sunitinib treated group. Notably, quality of life was maintained for those receiving nivolumab + cabozantinib while there was a decline in quality of life among those receiving sunitinib. In a subsequent update earlier this year, PFS continues to remain stable, with OS still not reached:
Finally, in the CLEAR trial, patients with previously untreated advanced RCC were randomization in a 1:1:1 fashion to lenvatinib 20 mg orally once daily + pembrolizumab 200 mg IV every 3 weeks; or lenvatinib 18 mg + everolimus 5 mg orally once daily; or sunitinib 50 mg orally once daily (4 weeks on/2 weeks off in 6-weekly cycles).5 The authors assessed the primary endpoint of progression-free survival by the Independent Review Committee per RECIST v1.1 with key secondary endpoints including OS, objective response rate (ORR), and safety. This trial randomized 1,069 patients, 355 who received lenvatinib and pembrolizumab, 357 who received lenvatinib and everolimus, and 357 who received sunitinib. Notably, intermediate and poor-risk disease comprised just over 70% of the cohort. Over a median follow-up of 27 months, PFS was significantly improved among patients receiving lenvatinib and pembrolizumab (median 24 months) vs sunitinib (median 9 months; HR 0.39, 95% CI 0.32–0.49) and among patients receiving lenvatinib and everolimus (median 15 months) vs sunitinib (HR 0.65, 95% CI 0.53–0.80). The benefit of lenvatinib and pembrolizumab versus sunitinib with respect to progression-free survival was consistent across many subgroups, comprising age, sex, geographic region, PD-L1 expression, IMDC risk group, prior nephrectomy, and sarcomatoid features. Further, OS was significantly longer among patients who received lenvatinib and pembrolizumab compared to sunitinib (HR 0.66, 95% CI 0.49–0.88), whereas there was no significant difference in OS for patients receiving lenvatinib and everolimus compared to sunitinib (HR 1.15, 95% CI 0.88–1.50). As with progression-free survival, these findings were consistent across all relevant tested subgroups for the comparison of lenvatinib and pembrolizumab, except patients with favorable-risk group. Grade ≥3 treatment-related adverse events occurred in 72% of patients in the lenvatinib and pembrolizumab arm and 73% of patients in the lenvatinib and everolimus arm compared with 59% of patients in the sunitinib arm.
There are several take-home messages from the IO/IO or IO/TKI combination trials, including pros and cons as listed:

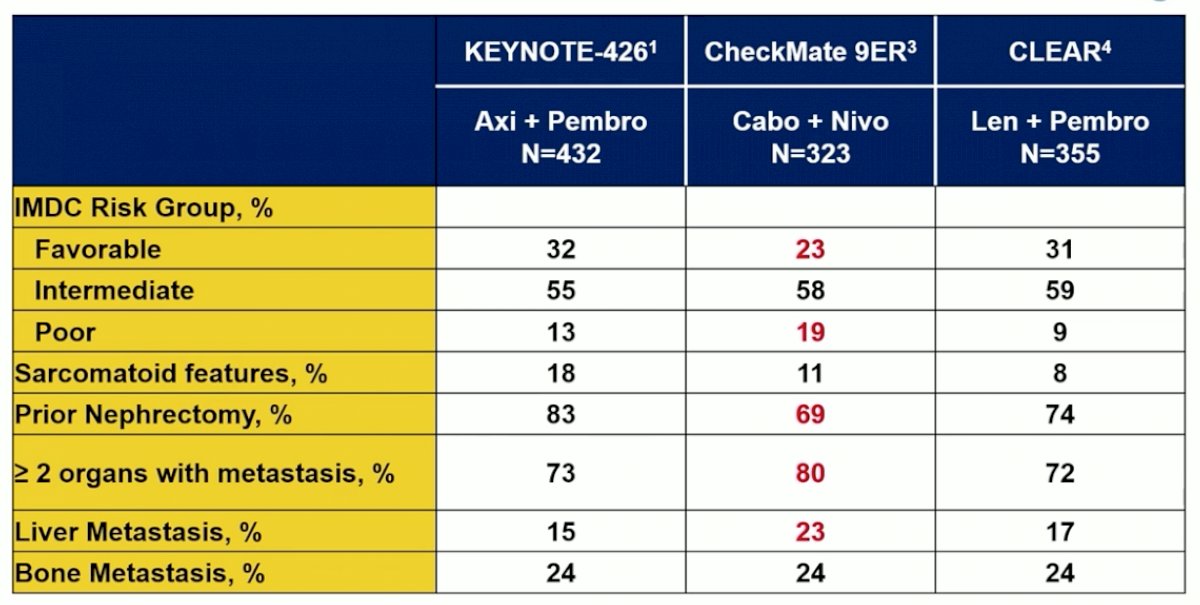
Dr. Choueiri notes that it is difficult to compare outcomes across these trials, given that even when assessing the IO/TKI trials that have a proven survival benefit (KEYNOTE-426, CheckMate 9ER, and CLEAR), they all have different baseline characteristics, specifically different proportions of IMDC risk groups:
Even comparing the quality of life data from the phase 3 studies (vs sunitinib) is difficult, since there are different instruments used across studies, assessed at different time points, variable compliance, thus making comparisons between studies challenging.
Dr. Choueiri then discussed several different populations of patients, starting with the IMDC favorable-risk patients. Highlighting the CheckMate 214 trial favorable-risk patients, the ORR was actually lower for nivolumab + ipilimumab (29.6%) compared to sunitinib (51.6%). Thus, there may be an argument for giving these patients sunitinib, however, the complete response rate of nivolumab + ipilimumab in this population is 12.0% compared to 6.5% for sunitinib. Furthermore, with extended follow-up for PFS and OS, the sunitinib benefit versus nivolumab + ipilimumab continues to shrink:

Among the IO + TKI trials that have an overall survival benefit in the ITT population, in the favorable risk groups, all of these trials have a PFS benefit, but no trial has an OS benefit:

Dr. Choueiri notes that in his opinion an OS benefit in favorable-risk patients for IO + TKI treatment may be elusive, given the limited number of patients, a limited number of events, and indolent disease with available second-line options.
The other population Dr. Choueiri highlighted was patients with metastatic RCC with sarcomatoid features. In CheckMate 214, the combination of nivolumab + ipilimumab demonstrated an OS benefit with a HR of 0.45 (95% CI 0.30-0.70) compared to sunitinib in this challenging subgroup:
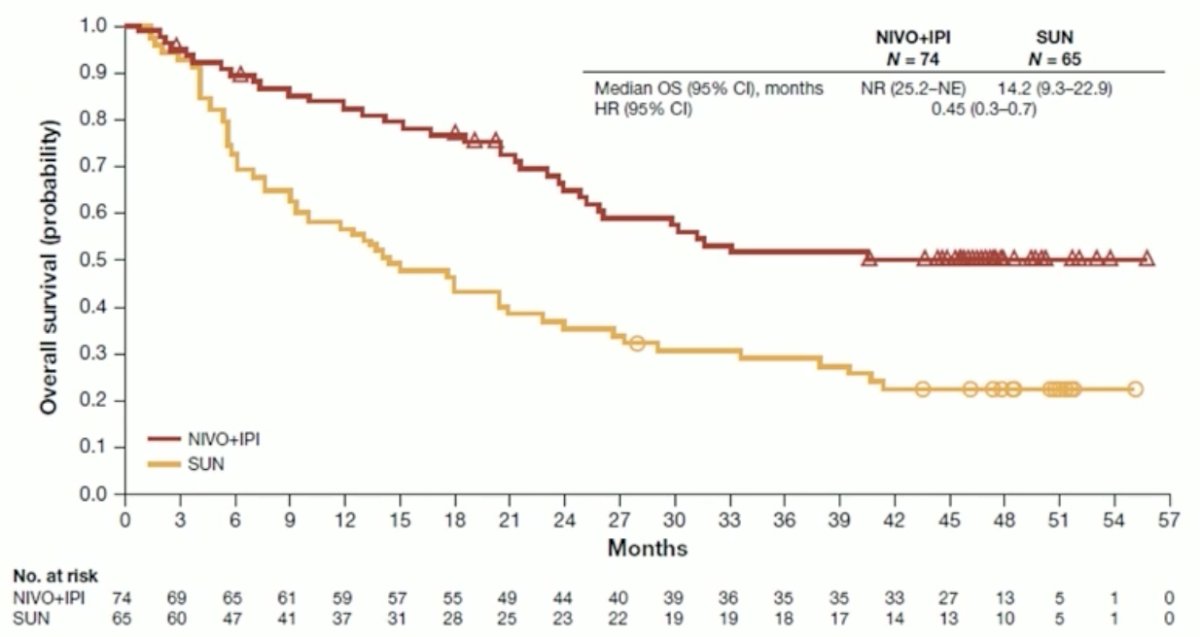
Sarcomatoid RCC tumors are characterized by an immune-inflamed phenotype, leading to activation of immune pathways, increased expression of antigen-presenting machinery genes, increased cytotoxic immune infiltration, and high PD-L1 on tumor cells. Standard of care for these patients according to Dr. Choueiri should be nivolumab + ipilimumab.
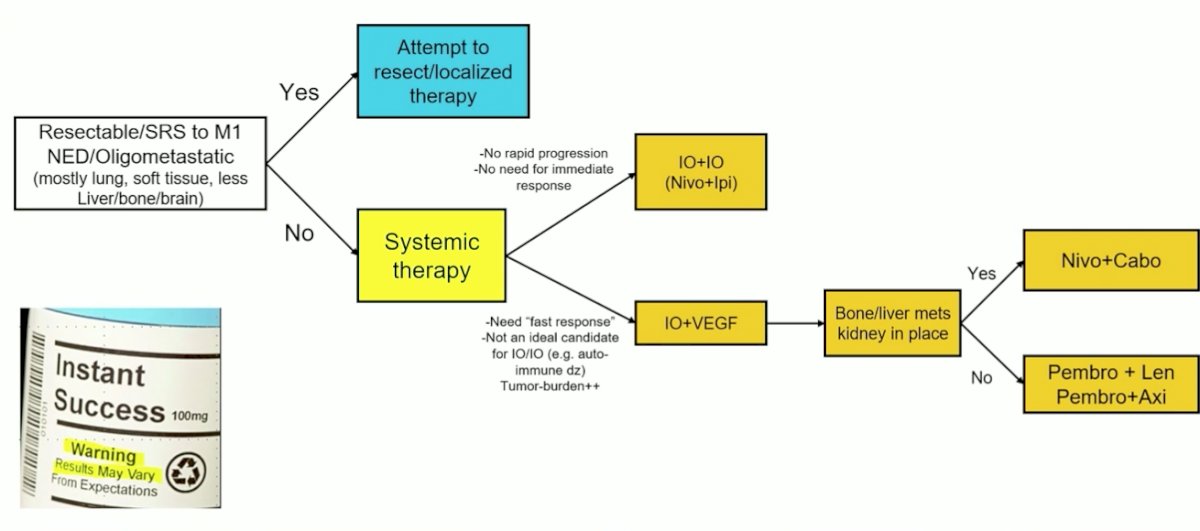
As of 2021, Dr. Choueiri’s own, evolving approach to the first-line treatment of metastatic RCC is as follows:
Dr. Choueiri concluded this presentation of the first-line treatment options for metastatic RCC with the following take-home points:
- There is a wealth of evidence of different combinations for the first-line treatment of metastatic RCC, including CheckMate 214, KEYNOTE-426, JAVELIN Renal 101, CheckMate 9ER, and CLEAR studies, with all trials showing improvement in the combination therapy compared to sunitinib
- Patients in the clinic do not always reflect the trial population and real-world evidence collection is important
- Many factors may influence a physician’s choice of sequential treatment and personalization of care, including availability, efficacy, safety, QoL, prior treatment, comorbidities, and cost
- The favorable-risk population best therapy remains undefined, however, a case can be made for IO + IO, IO + VEGF, or even VEGF monotherapy
- For patients with sarcomatoid features, nivolumab + ipilimumab should be the standard of care
- Biomarkers today all remain experimental in metastatic RCC
- If adjuvant IO becomes a reality, the first-line choice in metastatic RCC will become more complicated
Presented by: Toni K. Choueiri, MD, Dana-Farber Cancer Institute, Harvard Medical School, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 European Society for Medical Oncology (ESMO) Annual Congress 2021, Thursday, Sep 16, 2021 – Tuesday, Sep 21, 2021.
References:
- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carinoma. N Engl J Med 2018;378(14):1277-1290.
- Rini BI, Plimack ER, Stus V, et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med 2019;380(12):1116-1127.
- Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med 2019;380(12):1103-1115.
- Choueiri TK, Powles T, Burotto M, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021 Mar 4;384(9):829-841.
- Motzer R, Alekseev B, Rha SY, et al. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N Engl J Med. 2021 Apr 8;384(14):1289-1300.