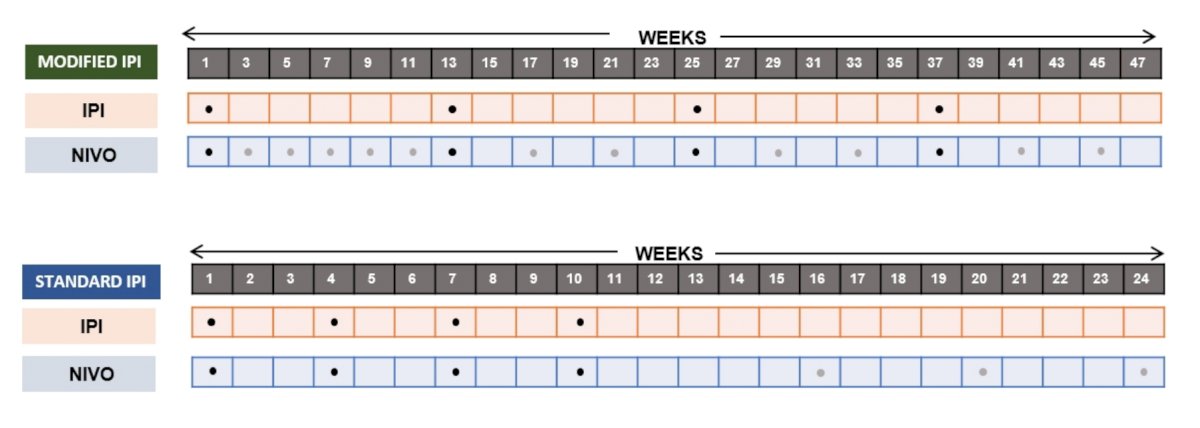
Patients with untreated clear cell advanced RCC were randomized 1:2 to receive 4 doses of ipilimumab 1mg/kg Q3W (conventional ipilimumab) or Q12W (modified ipilimumab), in combination with nivolumab (3mg/kg), until disease progression or unacceptable toxicity. The study design for PRISM is as follows:

As follows is a summary of the treatment schedule in PRISM:
The primary endpoint was the proportion of patients with a grade 3/4 treatment-related adverse events within 12 months of initiating treatment (from those who received at least one dose of therapy (modified intention-to-treat)). Secondary endpoints included progression-free survival (PFS) at 12 months tested against the historical PFS associated with sunitinib and objective response rate (ORR).
There were 192 patients (69.8% intermediate/poor-risk), including 128 patients in the modified ipilimumab arm and 64 patients in the standard ipilimumab arm, that received at least one dose of study drug. The median follow-up for the cohort was 19.7 months IQR: 15.9-23.6 months). Grade 3/4 treatment-related adverse events were significantly lower amongst patients receiving modified ipilimumab compared to conventional ipilimumab (32.8% versus 53.1%; OR 0.43, 90% CI 0.25, 0.72):

The most common grade 3/4 adverse events in the modified ipilimumab group was diarrhea (5.5%) and ALT increase (4.7%), whereas the most common grade 3/4 adverse events in the standard ipilimumab arm was arthralgia (7.8%), and diarrhea (4.7%). 12-month PFS rate was 46.1% (90% CI 38.6-53.2%) in the modified ipilimumab compared to the sunitinib historical rate of 39.7%; median PFS in the modified ipilimumab arm was 10.8 months (95% CI 8.2-14.2) compared to 9.8 months (95% CI 9.8-13.3) in the standard ipilimumab arm. Median PFS in the IMDC intermediate/poor risk group was 10.5 months for the modified ipilimumab arm (90% 7.0-14.2) compared to 8.6 months (90% 6.0-16.3) in the standard ipilimumab arm. In the intention-to-treat analysis, the ORR in for the modified ipilimumab arm was 45.3% (95% CI 36.7-53.9) compared to 35.9% (95% CI 24.2-47.7) in the standard ipilimumab. As follows is the summary of the treatment responses:

Although with limited follow-up, the median OS in either arm was not reached, however the 12-month landmark OS rate was 88.3% for the modified ipilimumab arm compared to 83.7% in the standard ipilimumab arm.
Dr. Vasudev concluded his presentation of the PRISM trial with the following take-home messages:
- Giving ipilimumab 12-weekly, instead of 3-weekly, in combination with nivolumab, was associated with a clinically significant reduction in rates of grade 3/4 treatment-related adverse events (33% versus 53%)
- The lower limit of the confidence interval for 12 month PFS observed with modified ipilimumab failed to exclude the rate associated with historical control data (sunitinib)
- However, median PFS, ORR, duration of response and 12-month landmark OS results were comparable between treatment arms
- This positive phase 2 trial supports further exploration of different nivolumab/ipilimumab regimes
Presented by: Naveen S. Vasudev, PhD, MRCP, MBChB, BMSc (Hons), Medical Oncology Department, St. James's University Hospital Leeds, Leeds, UK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 European Society for Medical Oncology (ESMO) Annual Congress 2021, Thursday, Sep 16, 2021 – Tuesday, Sep 21, 2021.
References: