(UroToday.com) The European Society of Medical Oncology (ESMO) 2021 annual meeting’s non-prostate cancer session included a presentation by Dr. Marc-Oliver Grimm discussing the role of prior nephrectomy on outcomes of avelumab + axitinib versus sunitinib in the JAVELIN Renal 101 trial for metastatic renal cell carcinoma (RCC). Cytoreductive nephrectomy has been a standard of care in metastatic RCC for 20 years, although its role in patients receiving currently available therapies remains controversial. In the randomized phase 3 CARMENA trial, OS results showed that treatment with sunitinib alone was not inferior to cytoreductive nephrectomy followed by sunitinib.1 In the randomized phase 3 SURTIME trial, there was no significant difference in PFS observed with sunitinib before deferred nephrectomy compared with cytoreductive nephrectomy followed by sunitinib.2 However, the role of prior nephrectomy in patients treated with immune checkpoint inhibitor remains unknown. In this extended follow-up analysis of the phase III JAVELIN Renal 101 trial (NCT02684006),3 Dr. Grimm and colleagues assessed the role of prior nephrectomy in patients with metastatic RCC presenting with synchronous metastases at the time of diagnosis and treated with avelumab + axitinib or sunitinib.
JAVELIN Renal 101 was a multicenter, open-label, randomized phase 3 trial comparing avelumab + axitinib with sunitinib in patients with advanced RCC. Efficacy outcomes were assessed from the third interim analysis in patients with metastatic RCC who presented with M1 disease at the time of diagnosis and had undergone prior nephrectomy or no nephrectomy in the avelumab + axitinib and sunitinib arms. Multivariate Cox regression analyses were used to assess hazard ratios for overall survival (OS) and progression-free survival (PFS; investigator assessment per RECIST 1.1). Logistic regression method was used to obtain the odds ratio for objective response (investigator assessment per RECIST 1.1).
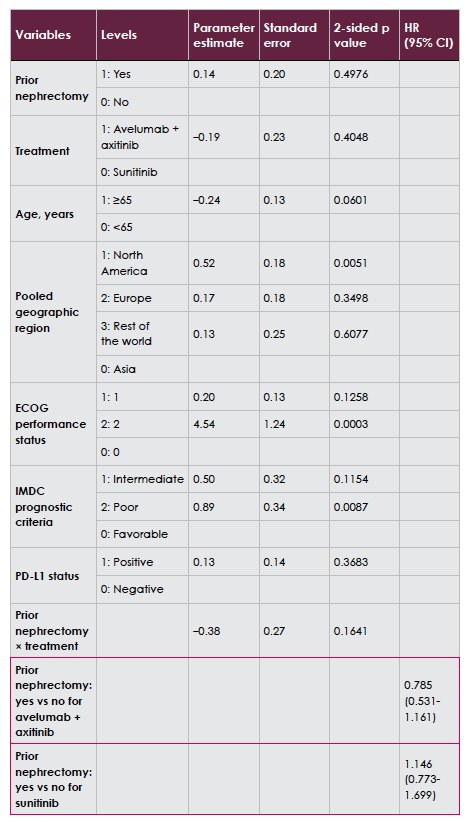
There were 412 of 886 patients in JAVELIN Renal 101 that presented with M1 disease at diagnosis. Of these patients, 126 (avelumab + axitinib) and 147 (sunitinib) had undergone prior nephrectomy and 72 (avelumab + axitinib) and 67 (sunitinib) had no nephrectomy. Compared with the nephrectomy group, a higher proportion of patients in the no-nephrectomy group were older (42% vs 32% were ≥65 years), had impaired performance status (ECOG PS 1, 54% vs 40%), and had poor prognosis (40% vs 16% by IMDC criteria). Additionally, fewer patients had PD-L1+ tumors (40% vs 77%). To assess the impact of nephrectomy, these parameters were adjusted in the multivariate model. Post hoc analyses showed that in the avelumab + axitinib arm, OS and confirmed objective response were significantly improved in patients with nephrectomy versus no nephrectomy (ORR: HR 2.669, 95% CI 1.315-5.414), however no differences were observed in the sunitinib arm (ORR: HR 2.018, 95% CI 0.824-4.941). As follows is the multivariable Cox regression analysis for OS:

PFS was numerically longer in patients with nephrectomy vs no nephrectomy in the avelumab + axitinib arm but not in the sunitinib arm.
Dr. Grimm concluded this subgroup analysis assessing the impact of prior nephrectomy on outcomes in the JAVELIN Renal 101 trial with the following take-home messages:
- Patients who presented with M1 disease at the time of diagnosis and had undergone prior nephrectomy had superior efficacy outcomes versus no nephrectomy with avelumab + axitinib but not with sunitinib
- In the avelumab + axitinib arm, PFS and OS were numerically longer in patients with a prior nephrectomy versus those without a prior nephrectomy, however there were no differences observed between groups in the sunitinib arm
- The confirmed ORR was numerically higher in patients with a prior nephrectomy versus those without a prior nephrectomy in the avelumab + axitinib arm, but not in the sunitinib arm
Presented by: Marc-Oliver Grimm, MD, Department of Urology, University Hospital of Jena, Jena, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 European Society for Medical Oncology (ESMO) Annual Congress 2021, Thursday, Sep 16, 2021 – Tuesday, Sep 21, 2021.
References:
- Mejean A, Ravaud A, Thezenas S, et al. Sunitinib alone or after nephrectomy in metastatic renal cell carcinoma. N Engl J Med 2018 Aug 2;379(5):417-427.
- Bex A, Mulders P, Jewett M, et al. Comparison of immediate vs deferred cytoreductive nephrectomy in patients with synchronous metastatic renal cell carcinoma receiving sunitinib: The SURTIME Randomized Clinical Trial. JAMA Oncol 2019 Feb 1;5(2):164-170.
- Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med 2019;380(12):1103-1115.