(UroToday.com) In the on-demand poster session of the European Society for Medical Oncology (ESMO) Annual Congress, Dr. Christopher Darr presented results of the phase II NIVOSWITCH trial assessing whether a 1st line switch-maintenance approach (CPI after TKI) improved outcome in metastatic clear cell renal cell carcinoma (mRCC). Each of these treatment approaches (CP and TKI) are accepted standards of care.
The authors enrolled 49 patients with mRCC who had partial remission (PR) or stable disease (SD) after 12 weeks of tyrosine kinase inhibitors (TKI) induction therapy. They were then randomized in a 1:1 fashion to receive either TKI continuation (24 patients) or nivolumab (NIVO; 25 patients.; 240 or 480 mg IV q2-4wk). The authors assessed objective response rate (ORR) (according to RECIST 1.1), progression-free survival (PFS), and adverse events (AE, according to CTCAE v4.03) from the time of randomization. The authors used the Kaplan-Meier technique and log-Rank analyses for time to event analyses. Further, patient-reported outcomes were assessed by the FACT Kidney Symptom Index (FKSI-15). Time to deterioration (TTD) was defined as the time between randomization to PRO decrease ≥3 points.
Among the 49 enrolled patients, the median age was 65 years, 82% were male and 4% had ECOG 2. The predominant metastatic sites were lung (47%), lymph nodes (27%), and liver (24%). MSKCC risk classification was favorable in 31%, intermediate in 65%, and poor in 4%. Prior to randomization, the response to TKI induction therapy was PR in 59% and SD in 41% of pts.
As of the database closure on December 2020, the ORR from randomization favored TKI continuation (16 vs. 48%; P=0.03). Additionally, after a median follow-up of 26.3 months (1.3-45.6), 40 PFS events and 17 deaths occurred. PFS was 3.0 vs. 11.9 months (HR = 2.57 [95% CI: 1.36 – 4.89]) in favor for TKI continuation. The median OS was not reached.

The 2-year OS was 64% for patients switched to nivolumab and 66% for TKI treatment (HR = 1.12 [95% CI: 0.43 – 2.89]; P=0.82).
In terms of toxicity, any AEs occurred in 96% of patients receiving nivolumab and 100% of those receiving ongoing TKI while the rates were 56% vs. 71% for grade 3-5 events and 48% and 50% for serious AE (SAE), respectively.
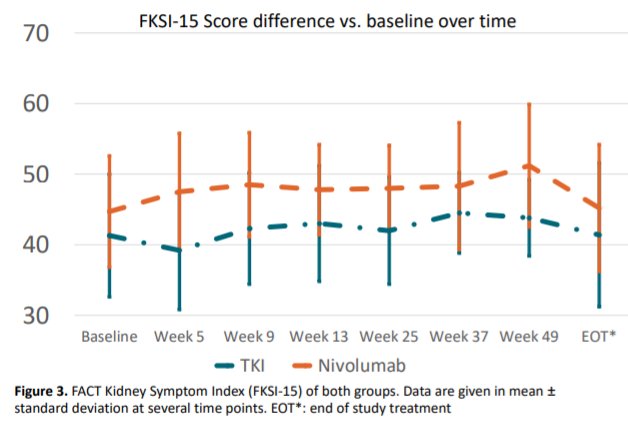
In terms of patients' reported outcomes, the median FKSI15 score at therapy initiation to end of therapy showed no significant difference between the two groups, though the median TTD favored nivolumab (NR) vs. TKI (6.9 months), the difference remained insignificant (P=0.16).
The authors, therefore, concluded that a switch-maintenance approach in mRCC is not recommended.