He first emphasized the question of why we may care about biomarkers. In particular, he emphasized that the distinction between prognostic and predictive biomarkers may be fluid, as the development of novel treatment approaches (or simply more data) may transform a currently prognostic biomarker into one that is predictive. Instead, he highlighted that biomarkers may help us answer a number of clinically relevant questions including:
- Who needs treatment?
- Who benefits from treatment?
- Do features associated with resistance help identify new treatment targets?
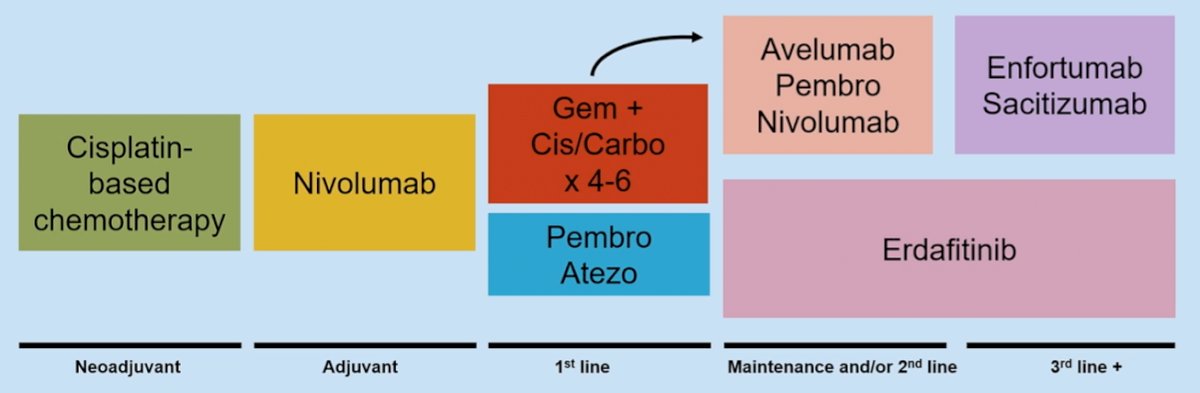
To set the stage for the role of biomarkers in advanced urothelial cancer, he highlighted the current treatment landscape across the spectrum of diseases ranging from neoadjuvant chemotherapy to third-line systemic therapy for metastatic disease and beyond.
In this context, there are two biomarkers that have already impacted clinical care and decision making, PD-L1, and FGFR3. He emphasized that these are limited given the gap between biomarker discovery and proof of clinical utility, based on a number of practical or technical reasons. In particular, he emphasized that features associated with adaptive immune resistance have been correlated with sensitivity to immune checkpoint blockade. PD-L1 expression is one such example. While these biomarkers have helped guide our understanding of the underlying disease biology, there are a number of practice considerations that have limited their clinical utility. In particular, he highlighted that each immune checkpoint inhibitor has a different associated biomarker which may be stored in a somewhat different fashion, utilizes a different assay, and maybe operationalized with different thresholds.

This makes generalized clinical applicability difficult. Instead, he suggested that combining biomarkers or clinical features may allow for better prediction of clinical outcomes. For example, he cited data supporting the combinations of three major groups of biomarkers including measures of adaptive immune resistance (associated with response to immune checkpoint blockade), measures of neoantigen burden (similarly associated with response to treatment), and measures of an activated stroma (which are associated with resistance). Combinations of these biomarkers may outperform each individually as they each confer independent prognostic information. However conceptually appealing, this approach does, however, introduce technical barriers given the multiple assays required.
Dr. Galsky emphasized that as our ability to characterize urothelial carcinoma with increasing resolution evolves, this should help us better develop useful biomarkers. Recent work from his own group has shown that three gene signatures may allow for the identification of either response or resistance to current therapies. One of these, a signature associated with tumor-promoting inflammation is relatively novel and appears to override the prognostic value of the stromal signature. Thus, the balance of the pro-tumorigenic inflammation signature and the adaptive immune responsive signature was best associated with response or survival among patients receiving anti-PD-L1 therapy. The group then identified that a subset of myeloid cells may account for this signature.
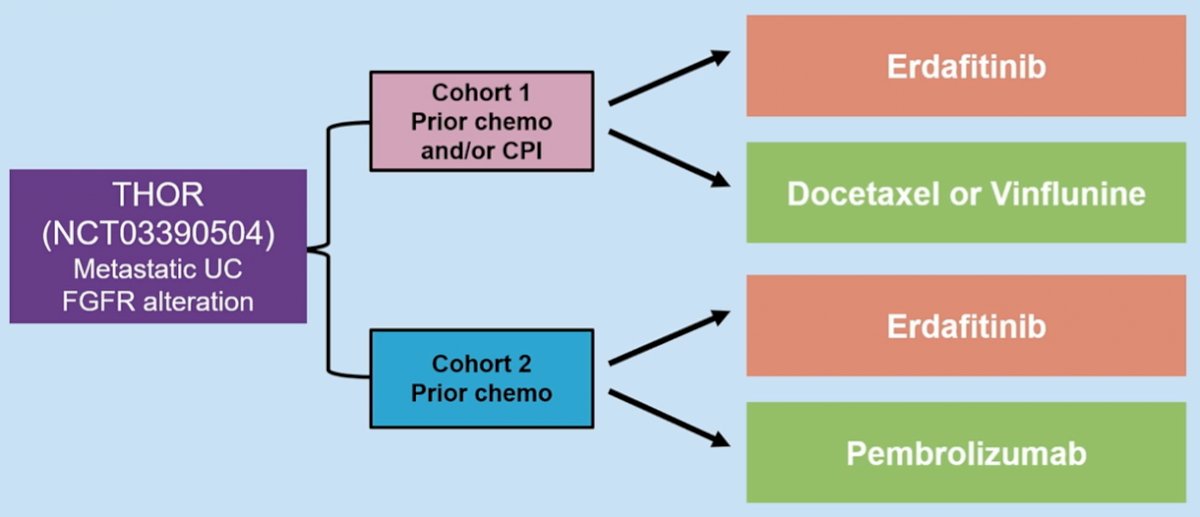
Dr. Galsky then transitioned to a discussion of cancer intrinsic biomarkers that may be operationalized dichotomously may be more straightforward, based on examples from other tumor types. In advanced urothelial carcinoma, FGFR3 mutations are seen in approximately 15-20% of patients and are associated with response to treatment to targeted therapy. As is currently being tested in the THOR trial, the question is whether FGFR3 status can guide the optimal sequencing of systemic therapy in this disease space.
While biomarkers may help define subsets of patients who benefit from treatment, he further emphasized the role of biomarkers in determining who needs treatment. The recently presented and published data from CheckMate-274 demonstrated the role for adjuvant nivolumab in patients following radical cystectomy among those with ≥pT3/pN+ disease (or ≥pT2 disease for those who received neoadjuvant chemotherapy). However, it is likely that not all patients will need adjuvant therapy as a large proportion of patients may not harbor micrometastatic disease and can be cured with surgery. Thus, defining the subset who will benefit from adjuvant therapy is important to personalize care. Based on analyses of the IMVigor010 cohort, the use of circulating tumor DNA as a minimal residual disease assay may allow for enrichment of patients who will benefit from adjuvant therapy.
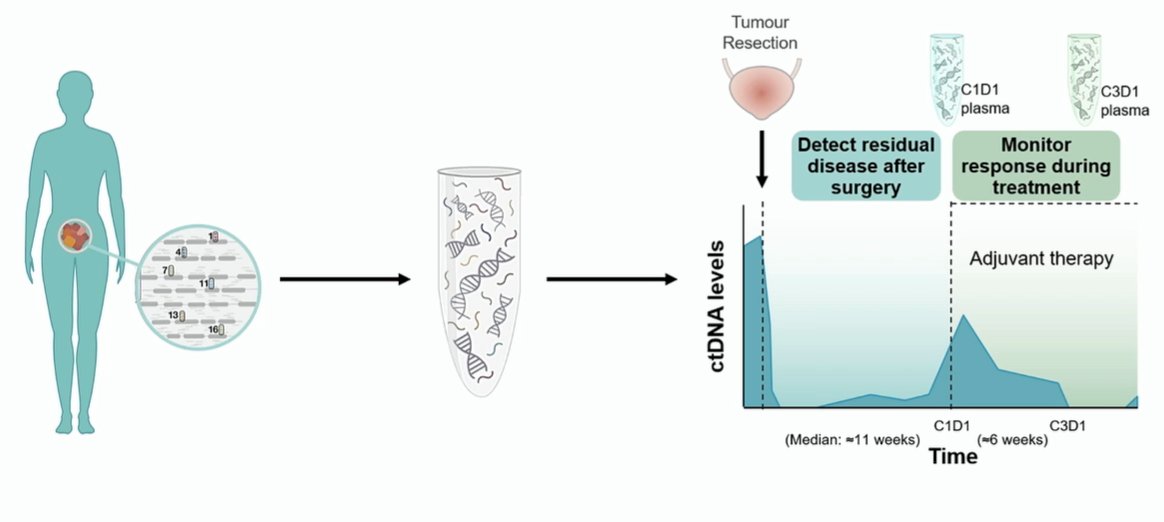
In the observation arm of the IMVigor010 trial, ctDNA detectable at day 1, cycle 1 had an important prognostic value in both disease-free survival and overall survival. Further, these data provided information that adjuvant therapy may improve outcomes while no benefit to adjuvant therapy was seen among patients without detectable ctDNA.
Dr. Galsky, therefore, concluded that the role of biomarkers to inform current treatment in advanced urothelial carcinoma is somewhat muddy. While PD-L1 and TMB (and ctDNA as a minimal residual disease assay) may possibly be informative and nectin-4 is not informative based on its ubiquity, only mFGFR3 is clearly useful today. The role of Trop-2 remains to be assessed.

Presented by: Matthew D. Galsky, MD, Professor of Medicine (Hematology and Medical Oncology), Director of Genitourinary Medical Oncology, Co-Director of the Center of Excellence for Bladder Cancer at The Tisch Cancer Institute, and Associate Director for Translational Research at The Tisch Cancer Institute at The Mount Sinai Hospital, New York, United States of America