In a mini-oral presentation at this year’s European Society of Medical Oncology (ESMO) 2020 Virtual Annual Meeting, Dr. Bo Dai presented the results of a phase II randomized trial assessing the role of local therapy to the prostate for men with newly diagnosed oligo-metastatic prostate cancer.
The authors included patients with newly diagnosed oligometastatic prostate cancer (defined as no more than 5 bone metastases or extra-pelvic lymph node metastases and the absence of visceral metastases), aged 18 to 80 years, with ECOG performance status 0 or 1, without histologic evidence of neuroendocrine differentiation, any prior primary tumor-directed treatment, and without prior systemic chemotherapy, or use of novel oral anti-androgen therapy (abiraterone, enzalutamide, apalutamide).
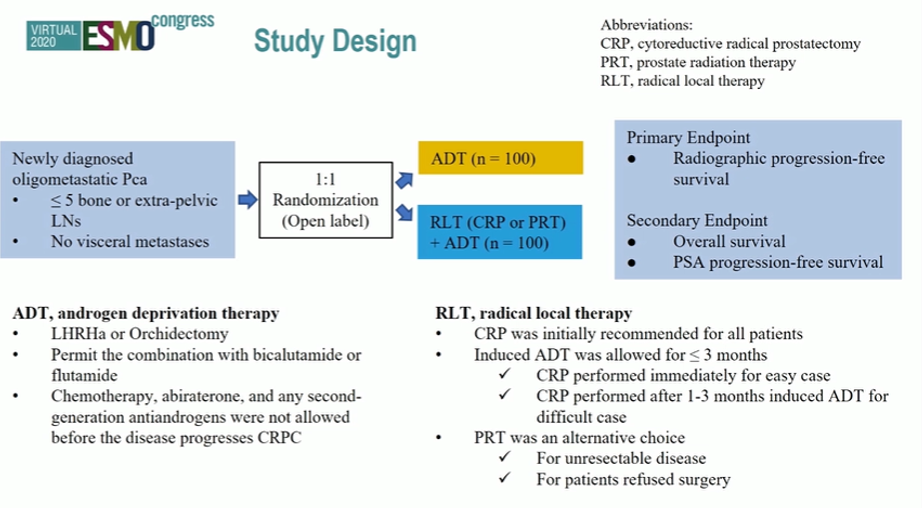
Patients were randomized in 1:1 open-label fashion to receive standard ADT with or without complete androgen blockade but without chemotherapy, abiraterone, enzalutamide, or apalutamide prior to CRPC or ADT plus radical local therapy defined as cytoreductive radical prostatectomy or prostate radiotherapy, with a preference for surgical extirpation.
Among those randomized to the radical local therapy arm, 85 underwent cytoreductive radical prostatectomy, 11 underwent prostate radiotherapy, 2 refused local therapy and 2 abandoned this approach following randomization due to disease progression. Among those undergoing surgery, Clavien 3b or greater complications were noted in 3 patients (3.5%).
With a median follow-up of 28 months, there was improved radiographic progression-free survival for those randomized to radical local therapy (median NR vs 50 months) (hazard ratio 0.50, 95% confidence interval 0.28 to 0.87, p=0.015).
The authors conclude that local therapy to the primary tumor improves radiographic progression-free survival in this patient population.
Presented by: Bo Dai, MD, Ph.D., Chief Physician, and Director of the Department of Urology, Fudan University Shanghai Cancer Center.
Written by: Christopher J.D. Wallis, MD, Ph.D., Urologic Oncology Fellow, Vanderbilt University Medical Center, @WallisCJD at the 2020 European Society for Medical Oncology Virtual Congress (#ESMO20), September 19th-September 21st, 2020.