Second, with regards to the study design, Dr. Efstathiou notes that the control arm of abiraterone or enzalutamide was essentially a placebo arm, considering that sequential treatment with androgen signaling inhibitors is common practice even though there is typically little benefit. However, she notes that the investigators should not be criticized for this as they made sure to allow crossover to the olaparib arm upon progression.
Third, the PROfound trial had positive outcomes that were clinically meaningful. These patients were all heavily pretreated, as all had prior novel androgen signaling inhibitors, 2/3 had prior taxanes, and 30-40% had extensive visceral disease. Thus, there are not many options left for these patients. It is clinically meaningful that among the BRCA1/2 and ATM cohort that olaparib doubled radiographic progression-free survival (rPFS) from 3.55 months in the abiraterone/enzalutamide arm to 7.39 months for olaparib (hazard ration (HR) 0.35, 95% confidence interval (CI) 0.25-0.47). However, she notes that the overall efficacy was largely driven by Cohort A (BRCA1/2 and ATM) given that there was no difference in rPFS for Cohort B (HR 0.88, 95% CI 0.88-1.36). Furthermore, looking even deeper into the details, the outcomes are really being driven by the 125 BRCA2 mutation patients: HR 10.84, 95% CI 9.17-13.08. Another clinically meaningful outcome, especially in this heavily pretreated cohort, is improved time to pain progression: 9.92 months in the abiraterone/enzalutamide arm and not reached in the olaparib arm (HR 0.44, 95% CI 0.22-0.91). Although overall survival (OS) data is immature, there is a signal for olaparib benefit, even with ~80% of patients crossing over to receive olaparib.
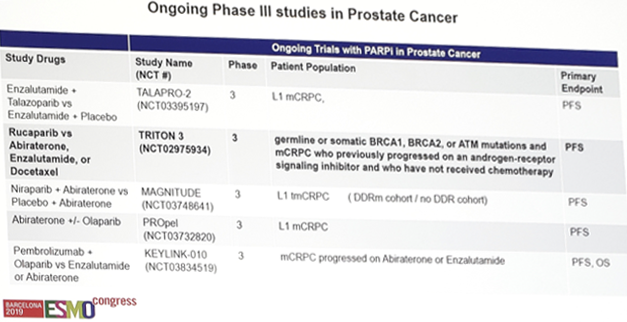
Fourth, are these reproducible results? As mentioned, this is the first prostate cancer Phase III trial to report, however poly ADP-ribose polymerase (PARP) inhibitor approval in other solid organs is largely driven by progression-free survival (PFS): olaparib in ovarian and breast cancer, rucaparib in ovarian cancer, niraparib in ovarian cancer, and talazoparib in breast cancer. And, looking at other Phase II studies in prostate cancer (TOPARP-A, TRITON2, and GALAHAD), there is BRCA2 concordance (the best responders) across these trials. Excitingly, there are ongoing Phase III studies in prostate cancer (TALAPRO-2, TRITON3, MAGNITUDE, PROpel, KEYLINK-010):
Fifth, Dr. Efstathiou wonders if there is community practice accessibility? There are certain barriers in this regard, as there is still heterogeneity in the community as to how these patients are worked up. Furthermore, there is still a lack of understanding regarding the importance of DNA damage repair alterations, of which 20% of metastatic castration-resistant prostate cancer (mCRPC) patients harbor. Importantly, there is also limited access to validated genomic assays, related to the high cost of certified assays, unavailability internationally, concerns with the validity of in-house assays, and limited understanding of reporting.
To summarize, Dr. Efstathiou notes that this is truly a practice-changing study. This is the first assay-specific study in advanced prostate cancer where a validated genomic tissue-based test successfully identified candidates for olaparib treatment. In patients with pretreated mCRPC and DNA damage repair alterations (mainly BRCA2), olaparib provided a statistically significant, clinically meaningful improvement with an acceptable safety profile. This signifies the initiation of the targeted therapy era and we should abandon sequential use of novel androgen signaling inhibitors.
Clinical Trial Information:
NCT02987543
Presented by: Eleni Efstathiou, MD, PhD, Associate Professor, Department of Genitourinary Medical Oncology, Division of Cancer Medicine, The University of Texas MD Anderson Cancer Center, Houston, Texas
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md at the 2019 European Society for Medical Oncology annual meeting, ESMO 2019 #ESMO19, 27 Sept - 1 Oct, 2019 in Barcelona, Spain