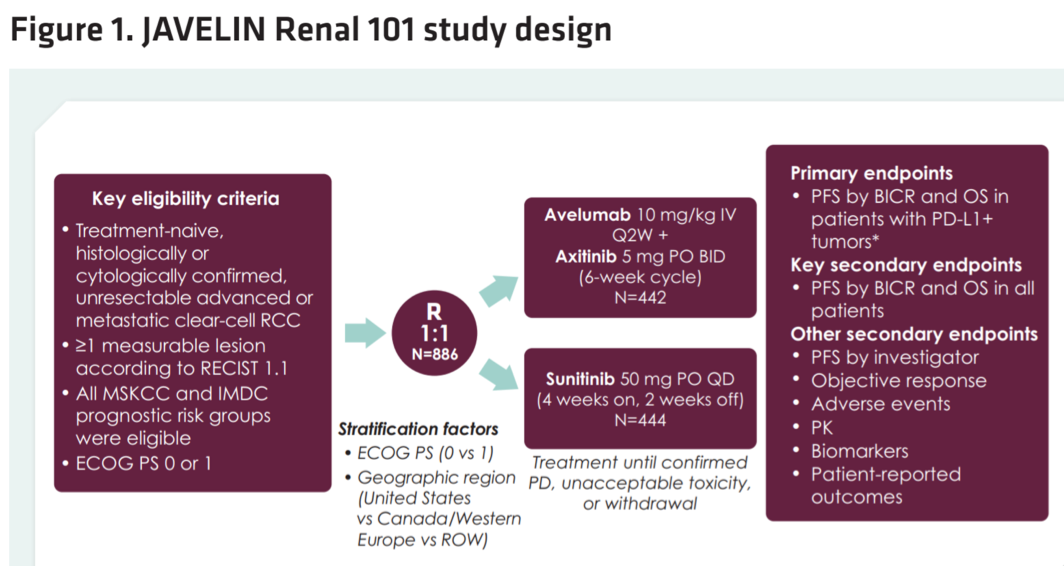
As has been previously reported, Javelin Renal 101 was a randomized phase III trial of 886 patients with a primary endpoint of progression-free survival. In the present analysis, investigators report the clinical outcome data at the time of the first Javelin Renal 101 data cutoff for patients with sarcomatoid histology. With respect to biomarker analysis, CD8 and PD-L1 expression were assessed by immunohistochemistry.
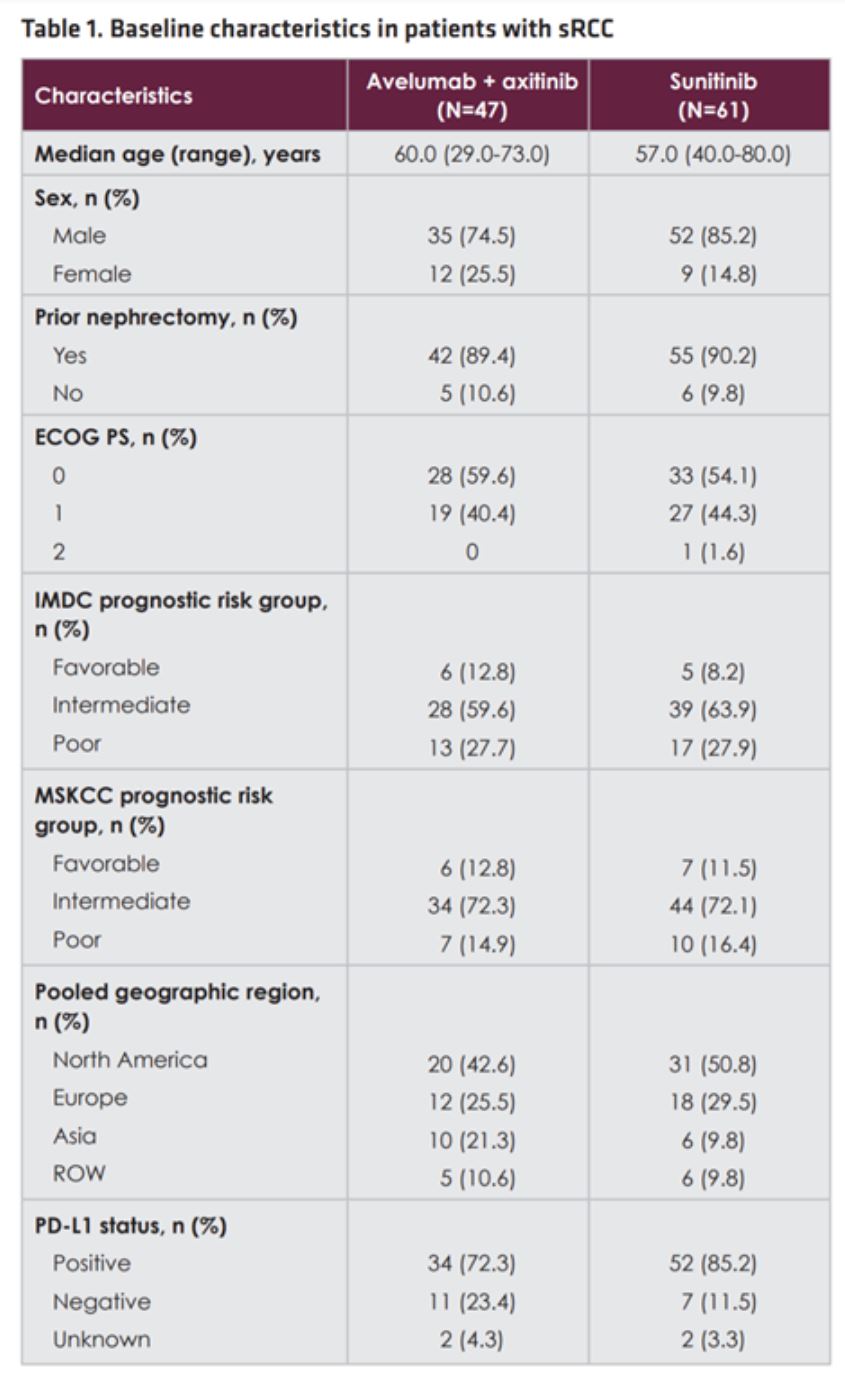
A total of 108 patients with sarcomatoid RCC were identified – 47 patients received avelumab plus axitinib, and 61 patients received sunitinib. The two arms were moderately well-balanced with respect to the sarcomatoid RCC patients with median ages of approximately 60 and male predominance of approximately 80%. Risk groups were also evenly distributed between the arms, including both the IMDC and MSKCC risk groups, as was ECOG performance status. Interestingly, the sunitinib arm exhibited a slightly higher rate of PD-L1 positivity at 85.2% compared to 72.3% in the avelumab plus axitinib arm.
Despite lower prevalence of PD-L1 positivity, the avelumab plus axitinib arm achieved a statistically significant improvement in objective response rate relative to sunitinib – 46.8% relative to 21.3%, and 2 sarcomatoid RCC patients had a complete response to the combination.

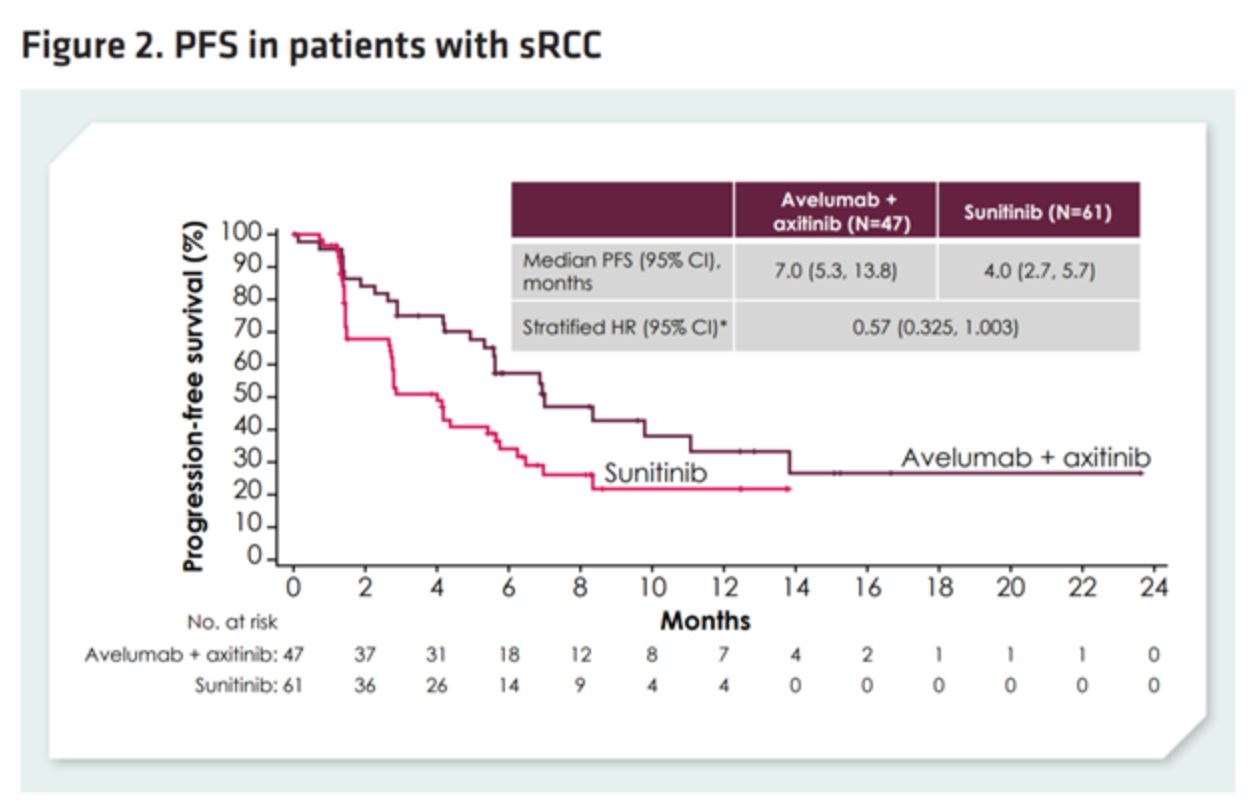
Furthermore, among sarcomatoid RCC patients, avelumab plus axitinib achieved a clinically significant 3.0-month improvement in progression-free survival (HR 0.57, 95 CI 0.325 – 1.003), though this study was not powered to detect survival differences specifically among sarcomatoid patients.
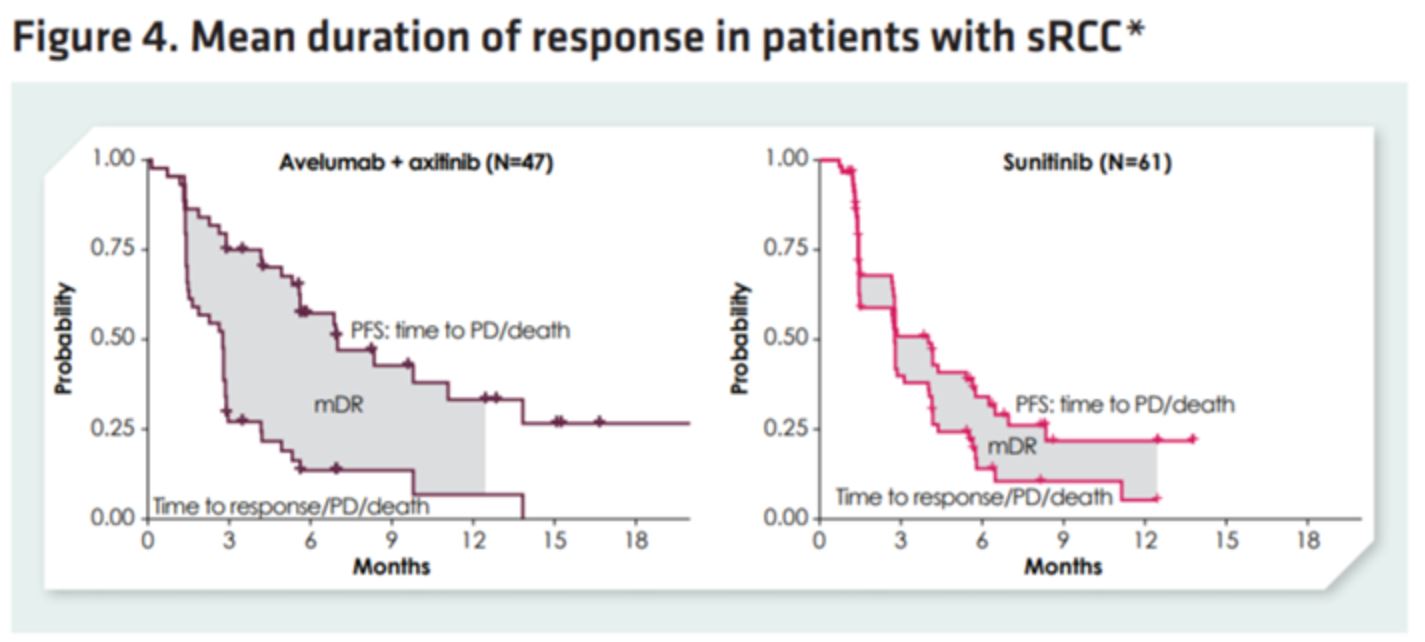
Among objective responders, aveluab plus axitinib patients generally exhibited a shorter time to first response at 1.6 months relative to 3.1 months with sunitinib.

Furthermore, patients treated with avelumab plus axitinib had a statistically significant 2.4-month improvement in duration of response.
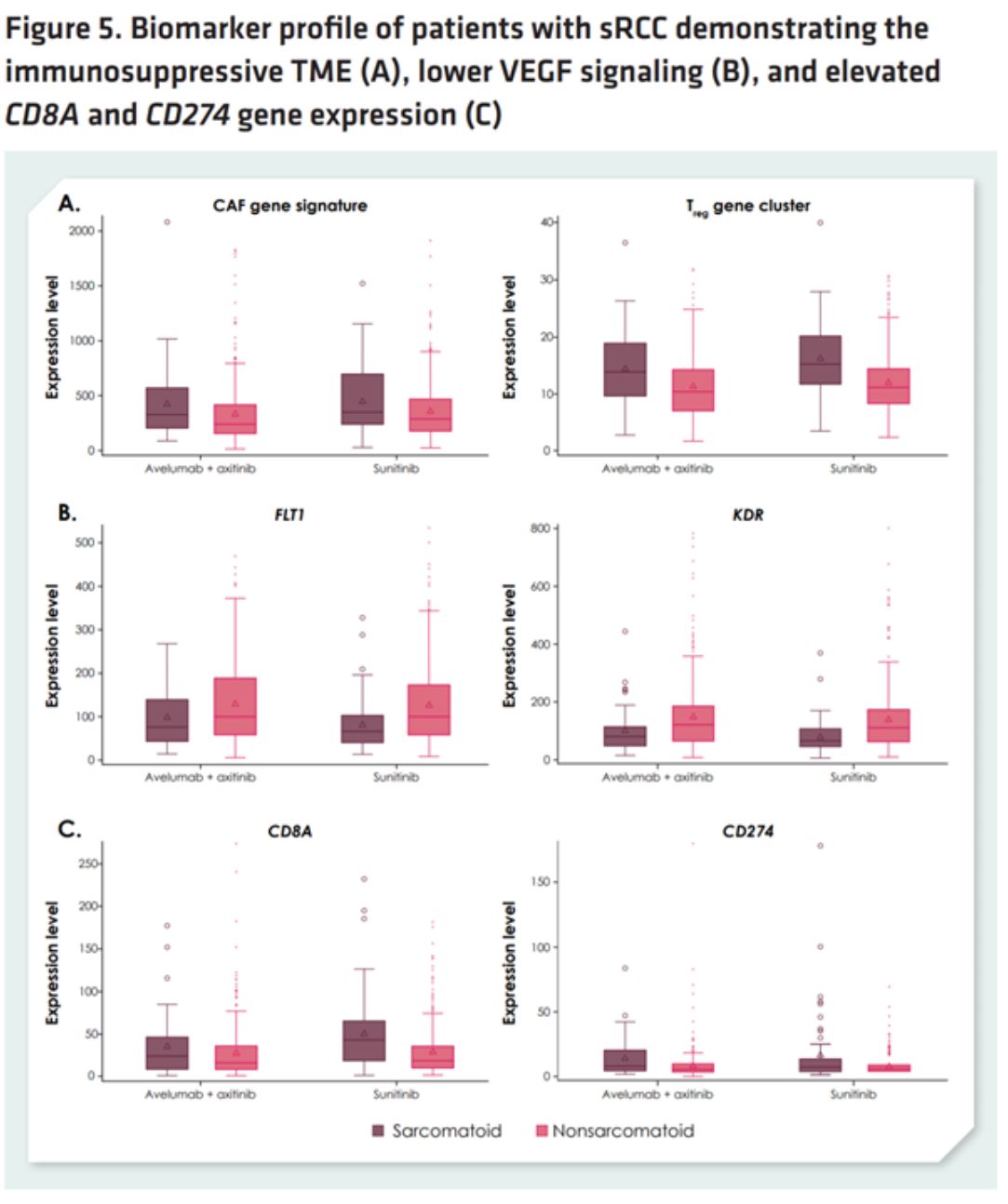
Gene expression analysis revealed sarcomatoid tumors to harbor an immunosuppressive tumor microenvironment enriched for cancer-associated fibroblast and regulatory T cell gene signatures. However, sarcomatoid RCC also exhibited higher CD8A and CD274 gene expression, suggesting an exhausted immune infiltrate. Investigators hypothesized that these features may explain both why sarcomatoid tumors are refractory to traditional VEGF directed therapy and why they respond preferentially to the anti-PD-L1 combination.
In summary, the Javelin Renal 101 data, taken in conjunction with the CheckMate214 data clearly suggest a benefit to immunotherapy and immune-oncology combinations in sarcomatoid RCC.
Presented by: Toni K. Choueiri, MD, Dana-Farber Cancer Institute, Boston, MassachusettsWritten by: Michael Lattanzi, MD, Medical Oncology Fellow, Memorial Sloan Kettering Cancer Center, Twitter: @MikeLattanzi at the 2019 European Society for Medical Oncology annual meeting, ESMO 2019 #ESMO19, 27 Sept - 1 Oct 2019 in Barcelona, Spain
References:
1. Kawakami F, Sircar K, Rodriguez‐Canales J, Fellman BM, Urbauer DL, Tamboli P, Tannir NM, Jonasch E, Wistuba II, Wood CG, Karam JA. Programmed cell death ligand 1 and tumor‐infiltrating lymphocyte status in patients with renal cell carcinoma and sarcomatoid dedifferentiation. Cancer. 2017 Dec 15;123(24):4823-31.Rini BI, Motzer RJ, Powles T,
2. McDermott DF, Escudier B, Donskov F, Hawkins RE, Bracarda S, Bedke J, De Giorgi U, Porta C. Atezolizumab (atezo)+ bevacizumab (bev) versus sunitinib (sun) in pts with untreated metastatic renal cell carcinoma (mRCC) and sarcomatoid (sarc) histology: IMmotion151 subgroup analysis.