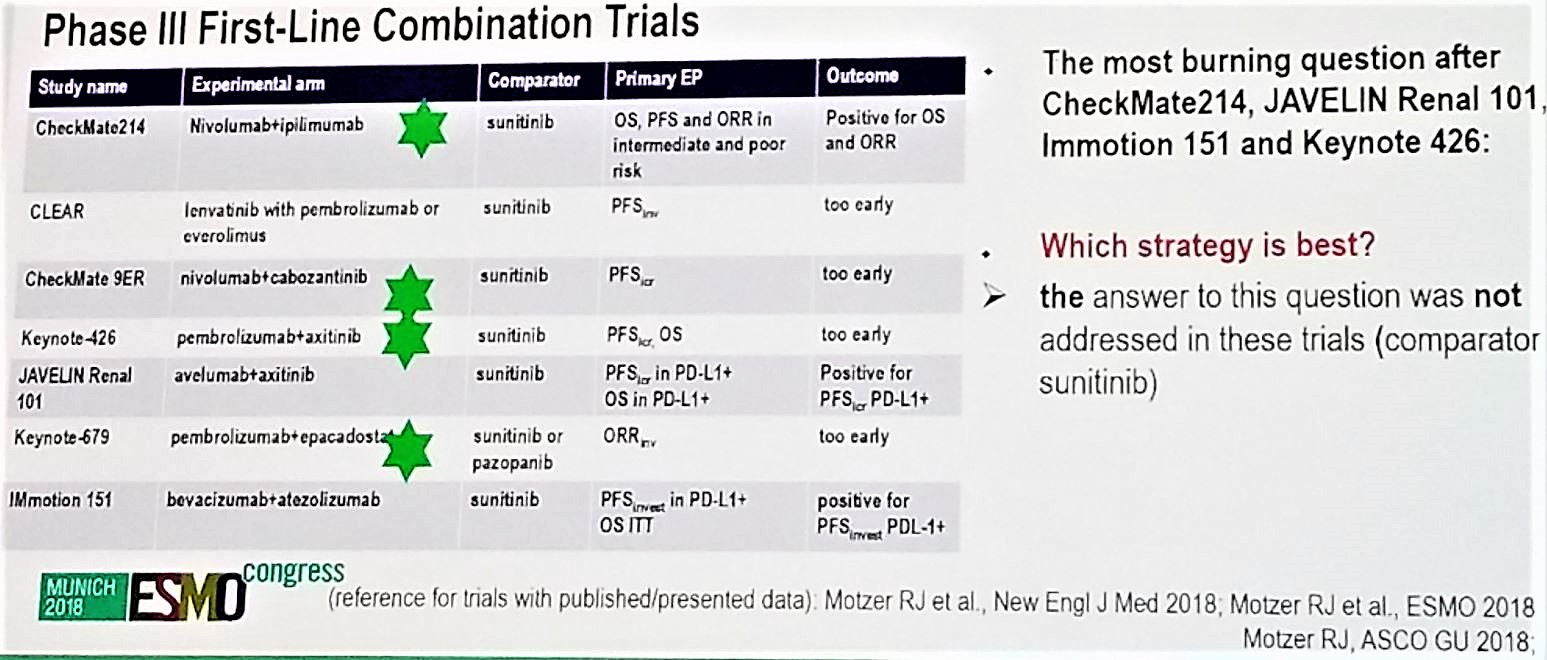
Figure 1- Phase 3 first-line combination trial in metastatic renal cell carcinoma patients:
As new strategies get approved, the cross-trial comparison will be the basis for treatment decisions. Several factors will need to be considered: Survival improvement, the degree of overall survival (OS) benefit, complete response (CR) rate, benefit in specific populations, and drug toxicity. The available information we have to date on tumor and disease biology does not answer the question of which treatment for which patient at what sequence. Our treatment decisions are currently based on histology and the various risk categories for mRCC (Figure 2).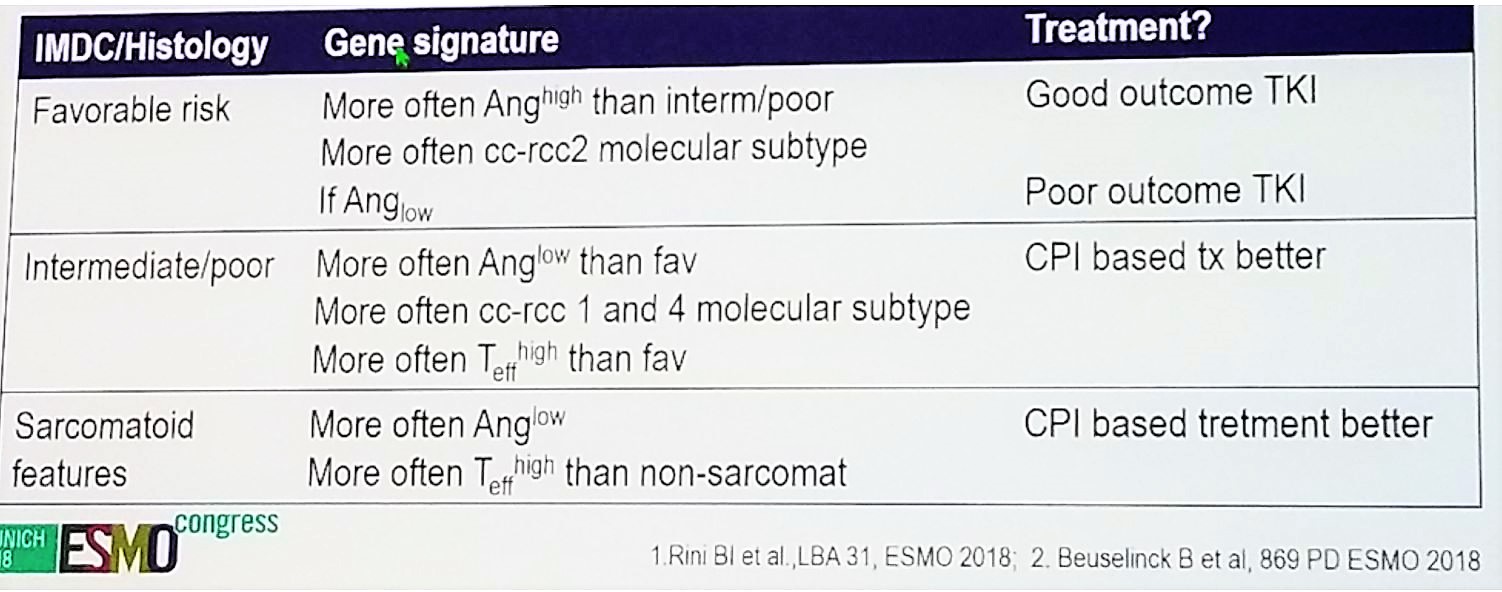
Figure 2- Treatment decision based on histology and IMDC/MSKCC risk scores:
Impressive results can be obtained when the biology and treatment match. A good example is the Checkmate 214 trial comparing nivolumab alone to nivolumab +Ipilimumab in different dosages. An excellent response was seen when the combination was given to PD-L1 positive patients1. For the non-responders, we need more data on individual biology. Part of the problem is that despite the staging attempting to stratify patients into smaller groups, the population is still highly heterogeneous. A good example is the intermediate risk group patients, who are highly heterogeneous2. It has been shown that within risk groups, gene signatures may vary tremendously, with high and low angiogenesis, high and low T Effector cells, and PD-L1 positive and negative3. All these have substantial effects on the treatments that these patients will respond to.
There are two different clinical scenarios that deserve a closer look:
- Patient belongs to a specific and well-described risk group, receives what is supposed to be the most appropriate treatment, but still does not perform well.
- The patient does not fit any of the guidelines, because his profile is quite rare.
When a tumor continues to progress despite treatment with immunotherapy, it is important to raise the question of whether the tumor is escaping cancer immunity despite the treatment being received. There are various escape mechanisms, including myeloid-derived suppressor cells, impaired T cell metabolism, impaired T cell tracking, and impaired infiltration, T cell dysregulation, induction of T cell apoptosis, lack of antigens, or microbiome dysbiosis. Therefore, it would tremendously help to get as much information as possible on the tumor escape mechanisms from the pathologist. This might help us to find a druggable target, but this is not always enough.
When the patient expresses high levels of CRP while being treated with ICI, and there are no signs of tumor regression, this might reflect high IL-6 secretion, which mediates myeloid-derived suppressor cells activation, a known escape mechanism, due to their ability to hinder ICI activity. VEGF inhibitors can be added to this patient, due to their ability to activate CD8+ T-Cells, and more importantly due to their capacity to deplete myeloid-derived suppressor cells. But aside from increased CRP, there are other signs of systemic inflammation that could represent an immunotherapy escape mechanism. These include thrombocytosis, neutrophilia, and an increase in CRP. These objective signs could all be a reliable surrogate for myeloid-derived suppressor cells or other immune escape mechanisms.
In summary, biology can help guide treatment decisions, with biomarkers showing differential effects across treatment groups. However, we are still not at a stage where we can get an exact fingerprint of the individual tumor along with a recipe for the best-detailed treatment. Biology cannot answer questions that should have been addressed in clinical trials. It is imperative that we understand that the individual biology can help to modify a treatment that was less effective than expected. This will be extremely useful in cases where the patient profile does not fit into any guideline. Understanding the biology will potentially make a therapeutic difference and improve outcomes of these patients.
Presented by: Manuela Schmidinger, MD, Clinical Division of Oncology, Department of Medicine, Medical University of Vienna, Vienna, Austria
Written By: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, Twitter @GoldbergHanan at the 2018 European Society for Medical Oncology Congress (#ESMO18), October 19-23, 2018, Munich Germany
References:
1. Motzer RJ et al. NEJM 2018
2. Sella A et al. Clin Genito Cancer 2017
3. Guida A et al. ESMO 2018