(UroToday.com) The 2022 International Kidney Cancer Symposium (IKCS) European Annual meeting featured a Keynote Lecture from Dr. Tim O’Brien discussing challenges in the surgical management of advanced and recurrent kidney cancer. Dr. O’Brien started by clarifying that this lecture is not about relatively straightforward renal masses that need a partial nephrectomy or a laparoscopic nephrectomy, but rather about T3/T4 renal masses that are challenging and often require a multidisciplinary approach:

Dr. O’Brien emphasized that it is crucial to operative with timely and recent imaging. When dealing with locally advanced RCC, a 3 month scan should be considered out of date; he prefers scans that are within one month of surgery and ideally less than 2 weeks prior to surgery. Furthermore, he cautions that patients presenting with pulmonary emboli are at risk of sudden death, and that these patients should be operated on as soon as possible (within days rather than weeks).
Next, Dr. O’Brien postulated that if a renal mass biopsy is necessary in ‘extreme cases’? To illustrate, Dr. O’Brien presented the following six complex locally advanced RCC cases:
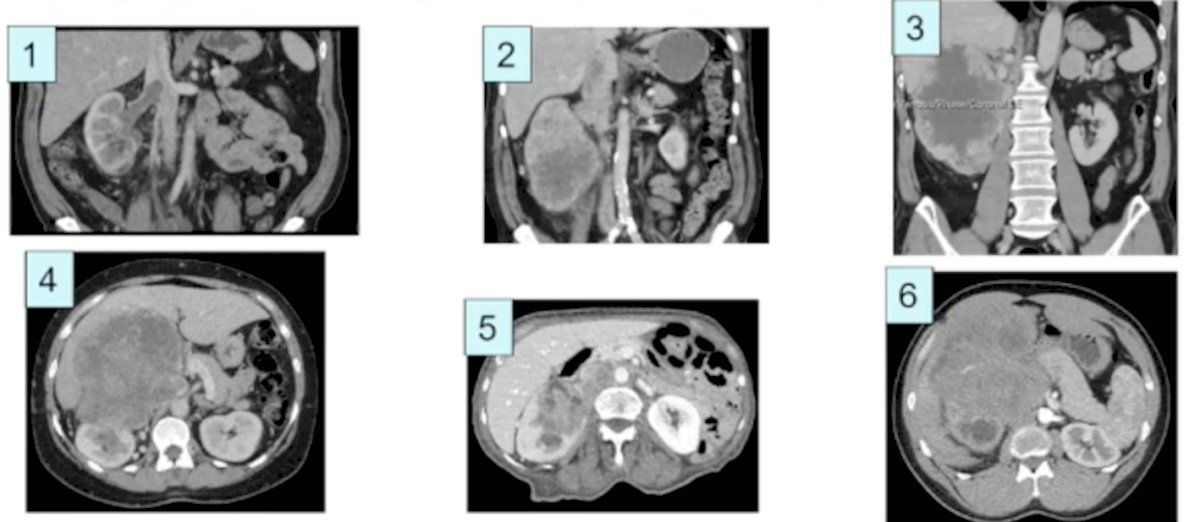
For cases 1 through 4, Dr. O’Brien did not obtain a biopsy, however for cases 5 and 6 a biopsy was obtained, which showed upper tract urothelial carcinoma (case 5) and Wilms tumor (case 6). Following radical nephrectomy, case 1 was a Wilms tumor, case 2 was clear cell RCC, case 3 was clear cell RCC with sarcoma, and case 4 was a leiomyosarcoma. Dr. O’Brien emphasized that when patients have concomitant bilateral renal masses, he always obtains a biopsy in order to rule out oncocytoma, given that bilateral oncocytoma is not that uncommon.
When assessing whether there is invasion into surrounding structures, Dr. O’Brien takes a stoplight metaphorical approach:
- Green light (operate): invasion into the IVC, colon, tail of the pancreas, spleen, psoas muscle, or diaphragm
- Amber light (operate with caution): invasion into the liver, lymph nodes, or head of the pancreas
- Red light (do not operate): invasion into the superior mesenteric artery, celiac trunk, duodenum, or bones
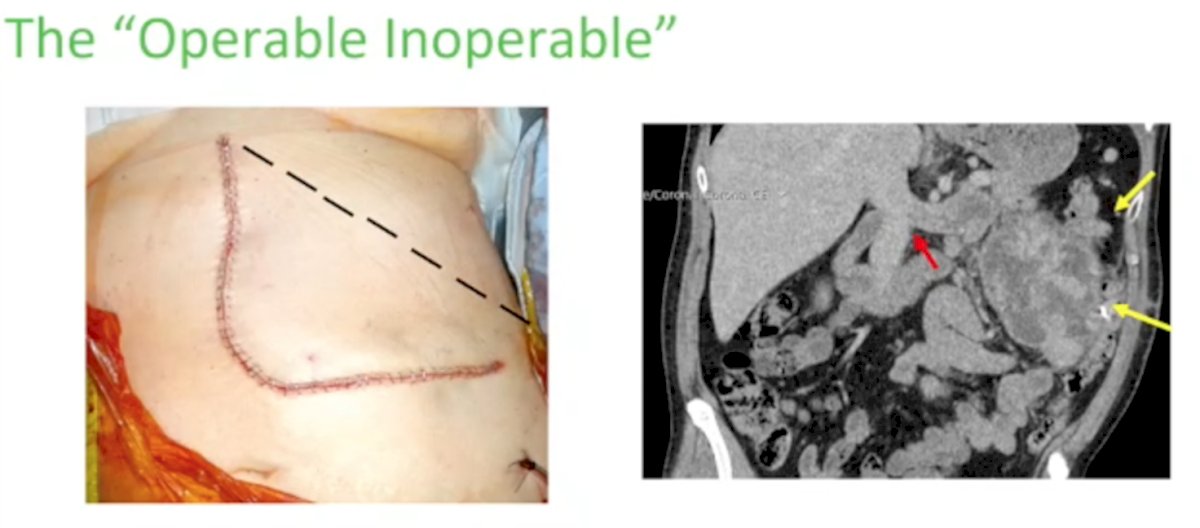
One of the hardest decisions to make when treating patients with locally advanced RCC is deciding if a tumor is operable or inoperable. Dr. O’Brien provided the following challenging cases for discussion regarding tumor operability:

At the time of referral to Dr. O’Brien, cases 1, 3, and 5 were deemed “inoperable”. Ultimately, all 6 patients underwent an operation, with a degree of difficulty of 8/10 for cases 1 and 5, 9/10 for cases 3 and 6, and 10/10 for cases 2 and 4 (case 2 – tumor thrombus ascending the IVC and bland thrombus in the lower IVC/common iliac veins; case 4 – colon/side wall invasion laterally, and abutment of the majority of the aorta medially). According to Dr. O’Brien, one of the keys to making an “inoperable” tumor operable is making the correct incision. For example, a large, locally advanced renal mass is difficult to remove safely through a subcostal incision given that once inside the abdomen with a subcostal approach, the surgeon comes right down onto the colon, with very little access to the renal vasculature. When using an ‘L’ or hockey stick incision, exposure to the renal hilum early is much easier and safer:
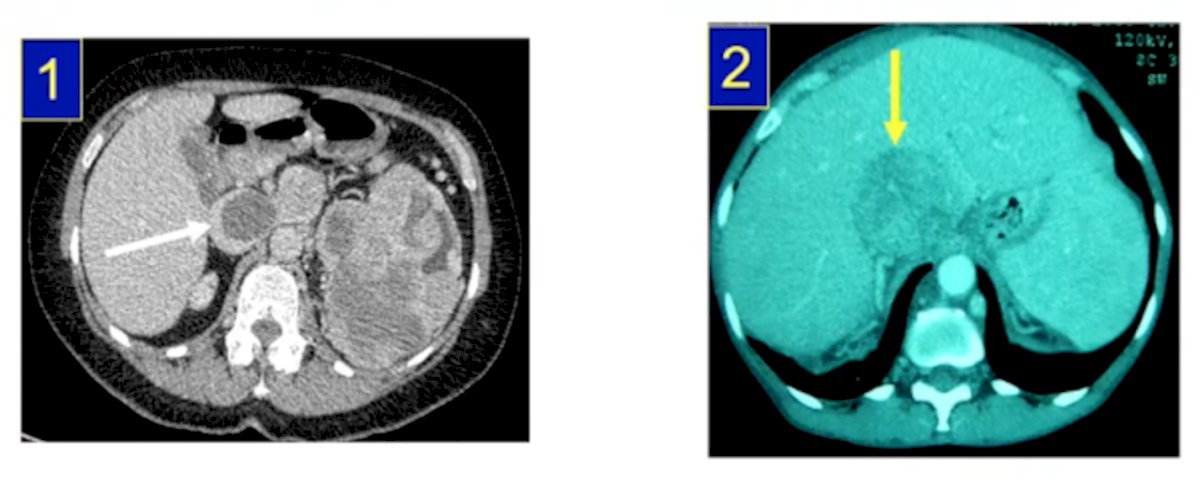
When ‘Learning from the Extreme’ Dr. O’Brien emphasizes several important points. First, the importance of ligating the renal artery early. To do this, one must (i) dissect the 4th part of the duodenum off of the aorta, (ii) ‘hug’ the front of the aorta, and (iii) slide under the left renal vein. In Dr. O’Brien’s practice, if there is a venous thrombus and the renal artery is able to be ligated early, this saves approximately one liter of blood loss. Dr. O’Brien is also a big advocate of utilizing RPLND techniques used for testicular cancer surgery, namely bowel mobilization allowing complete exposure of the entire retroperitoneum, and complete access to the great vessels and the renal hilar vessels. Second, assessing venous invasion, given that not all IVC thrombi are created equally. In the first example, venous blood is still able to traverse the IVC, whereas in the second example there is complete occlusion of the IVC with IVC expansion and compression against the surrounding liver:
According to Dr. O’Brien, the worst combination of IVC occlusion is cephalad venous thrombus and vascular thrombus secondary to venous stasis behind the IVC tumor thrombus. Third, is being aware of cardiac invasion. For these patients, it is crucial to place patients on cardiac bypass, often with the use of hypothermia (28 degrees C) in order to operate for ~30 minutes in a bloodless field. Furthermore, it is important to note that if the IVC tumor extension is intra-cardiac, Dr. O’Brien cautions operating on patients if the INR is > 2. In his practice, in patients with an INR < 2 the mortality rate is 2.5% (2/86), compared to 60% (3/5) if the INR is >2. Fourth, is being aware of high output cardiac failure. Certain large volume tumors can be so vascular, that the cardiac output these tumors require leads to high output cardiac failure. A radical nephrectomy for these patients essentially corrects this cardiac derangement. Fifth is deciding if preoperative renal artery embolization is necessary. Dr. O’Brien notes that he only embolizes the kidney if he is concerned that he will not be able to get early access to the renal artery. Given the inflammatory response that may occur with preoperative embolization, he opts for embolizing the renal artery less than 2 hours prior to surgery, essentially having the patient moved from interventional radiology suite directly to the operating room.
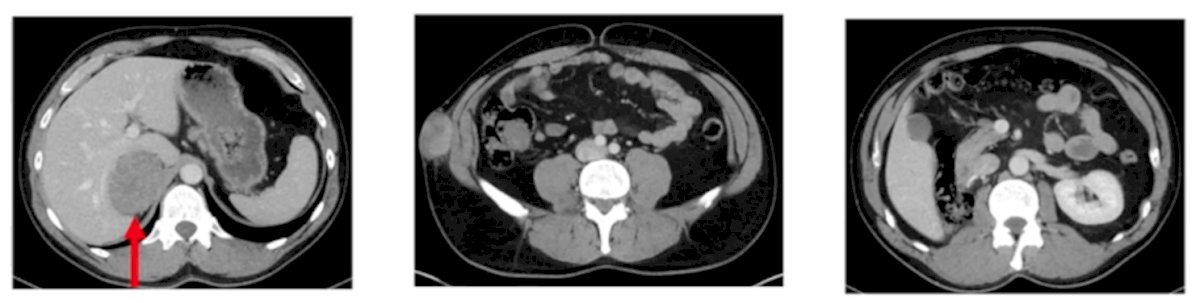
In the setting of recurrent disease, an important question to ask is whether these patients need a biopsy to confirm disease recurrence. For lymph node recurrence, if lymphadenopathy is present in a “reasonable template” for recurrent kidney cancer, a biopsy may not be necessary. For chromophobe RCC, Dr. O’Brien notes that N+ M0 disease does occur, and in these patients he has changed his practice to being very aggressive surgically in these scenarios, doing a complete retroperitoneal lymph node dissection:

In the recurrent disease setting, if the disease is resectable, Dr. O’Brien’s moto is to go for it operatively. In these situations, particularly in the setting of IVC recurrence, it is important to be aware of the possibility of vascular replacement. Unfortunately, Dr. O’Brien notes that tumor seeding (usually during extraction of the tumor during a minimally invasive procedure) is more prevalent than likely reported. When the disease recurrence pattern after a nephrectomy is abnormal, the potential for a seeding event has to be high on the differential diagnosis:
To summarize the principles of recurrent disease, Dr. O’Brien provided the following questions one should ask:
- Is it localized or metastatic?
- Is the patient symptomatic?
- What is the patient’s physiological reserve?
- Can you do it safely?
Importantly, the dissection is always harder than it looks and we are in need of an evidence base in this disease space.
As a final extreme case presentation, Dr. O’Brien showed a CT image of a level 3 IVC thrombus, however in a patient who was a Jehovah’s witness (no receipt of blood transfusion) and a hemoglobin of 78 g/L.
The multidisciplinary approach to this patient was to treat the patient with 4x 1g IV iron, as well as very high doses of erythropoietin. After this treatment regimen, 7 weeks later, the patient’s hemoglobin was 110 g/L, and he underwent a successful (and safe) radical nephrectomy with IVC thrombectomy. While most patient’s post-operatively after a complex radical nephrectomy + venous invasion will often have their hemoglobin level slowly drift down, Dr. O’Brien notes that this patient’s hemoglobin improved quickly post-operatively, perhaps secondary to the ‘priming’ of the bone marrow after preoperative treatment with iron and erythropoietin. Based on this case, Dr. O’Brien postulates whether our current approach to pre-operative anemia may be outdated.
Dr. O’Brien concluded his Keynote Lecture discussing challenges in the surgical management of advanced and recurrent kidney cancer stating that “there is no place in surgery for occasional extremists.” Thus, volume matters, and these procedures are best served in high volume centers.
Presented by: Tim O’Brien, MA, DM, FRCS (Urol), Guy’s and St. Thomas’ Hospital, NHS Foundation Trust, London, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 International Kidney Cancer Symposium (IKCS) Europe Annual Hybrid Meeting, Antwerp, Belgium, Fri, Apr 22 – Sun, Apr 24, 2022.