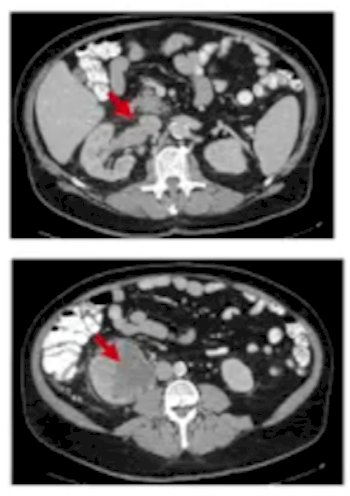
(UroToday.com) The 2022 International Kidney Cancer Symposium (IKCS) European Annual meeting included a session on surgical approaches to kidney cancer and a presentation by Dr. Tian Zhang discussing perioperative indications for systemic therapy. Dr. Zhang started by highlighting two clinical cases in her practice, both of which were referred to here for systemic therapy. The first patient is a 68-year-old woman that presented with severe left flank pain and subsequent abdominal/pelvic CT scan showed an 8-cm left renal mass invading posteriorly into the chest wall/rib. All lab values were normal and as follows are images from the CT scan:

The second patient is a 65-year-old man that presented with hematuria and subsequent CT scan showed a 9 cm right renal mass with renal vein thrombus, a hemoglobin of 8, platelets of 546, and calcium of 13. A biopsy of this mass showed clear cell with sarcomatoid differentiation and the CT scan for this patient is as follows:
Dr. Zhang notes that there are several potential benefits of pre-operative systemic therapy, including:
- Downsizing of the primary tumor, as well as potentially decreasing any renal vein thrombus or IVC thrombus
- Improving the challenges of a radical nephrectomy
- Changing the surgical approach, perhaps from radical nephrectomy to partial nephrectomy
- Improving systemic symptoms or clinical instability prior to surgery
- Treating micrometastatic disease that may develop into true metastatic disease and limit disease free survival/overall survival after surgery
As follows is a timeline of US FDA approved therapies in advanced kidney cancer:
Dr. Zhang notes that the neoadjuvant VEGF inhibitor trials have been small (sample size 18-25), with objective response rates ranging from 5%-46%. Thus, there is a paucity of evidence, at best. Advantages of neoadjuvant VEGF inhibition include this therapy being oral pills, thus allowing ease of administration and the ability to stop quickly. Disadvantages of neoadjuvant VEGF inhibition include timing of surgery depending on half-life of treatment, and would healing delays secondary to VEGF inhibition. Neoadjuvant immune checkpoint inhibitor trials have also been small trials with no objective responses and 1-2 year RFS rates of 82%-85%:

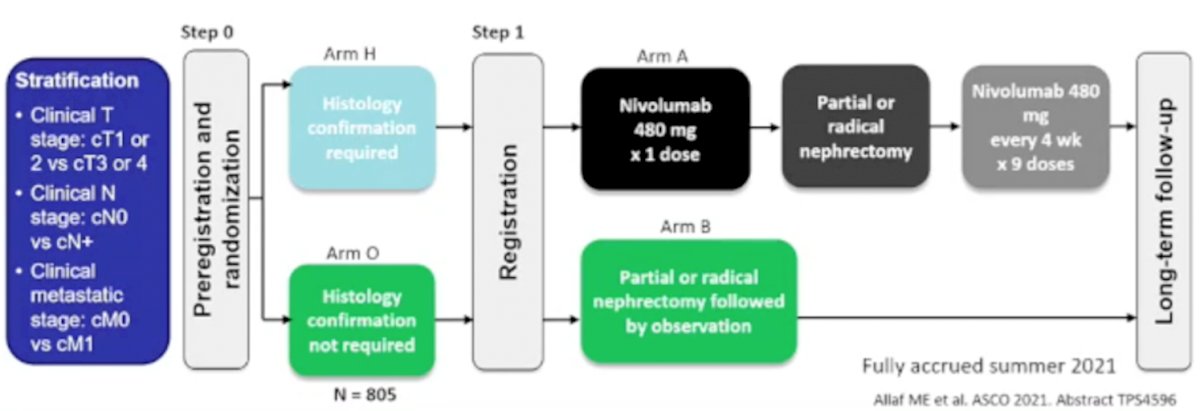
The main advantage of neoadjuvant immune checkpoint inhibitors is that there is less wound healing from treatment, however several disadvantages include: (i) immune mediated adverse events and short-term toxicities, (ii) IV treatments, (iii) inflammatory changes and fibrosis complicating surgery, and (iv) use of steroids or other immune suppressive medications delaying surgery. Dr. Zhang notes that the PROSPER clinical trial finished accrual in summer 2021, which is testing nivolumab followed by partial/radical nephrectomy followed by nivolumab versus partial/radical nephrectomy. The trial design of PROSPER is as follows:
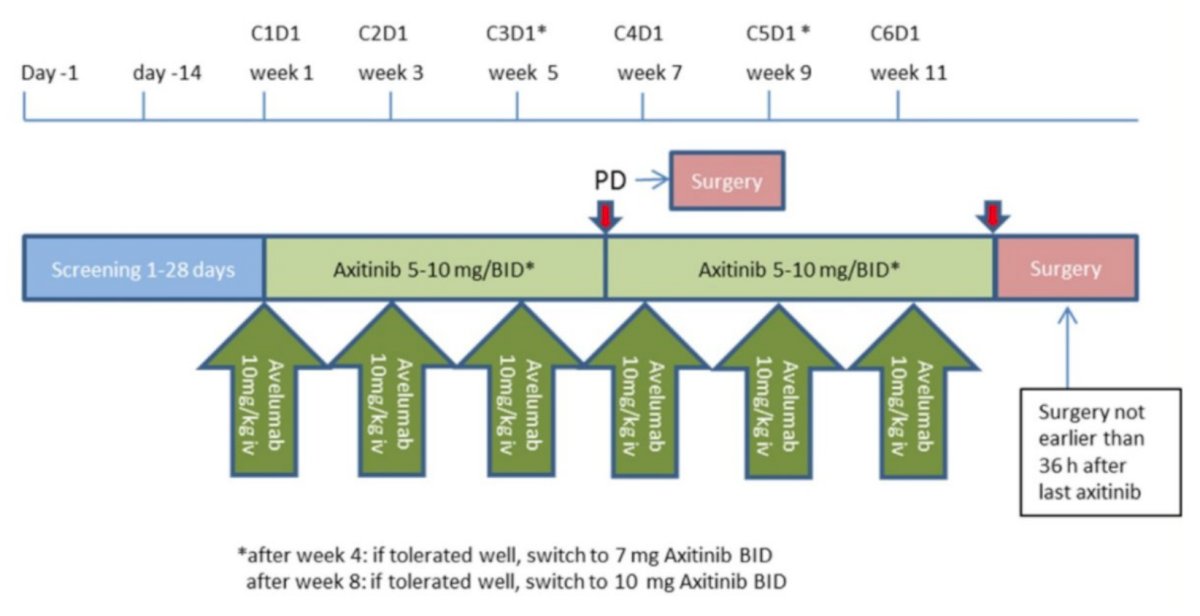
At GU ASCO 2022, Dr. Axel Bex presented results of the NeoAvAx study examining neoadjuvant avelumab and axitinib following nephrectomy for patients who are at high risk for recurrence. This single arm phase II trial enrolled adult patients (age 18 years and older) with clinically high-risk clear cell RCC, WHO performance status 0-1, and no comorbidities that preclude surgery or systemic therapy. Patients were defined as having high-risk clear cell RCC if they had cT1b-T2a grade 4 disease, cT2b-3a grade 3-4 disease, cT3-4 disease of any grade, or resectable node-positive disease regardless of primary tumor stage or grade. The trial schema for NeoAvAx is as follows:
The primary endpoint was RECIST 1.1 partial response in the primary tumor in ≥25%. Between May 2018 and October 2021, 40 patients were enrolled. The median age was 63 years (range 47-74). Eight patients (20%) had T4 disease and 17 (42.5%) had node positive disease. Baseline tumor diameter was 10.3 cm (range 5.6 to 18.8 cm) and baseline lymph node diameter (in 17 patients with nodal disease) was 2.6 cm (range 1.1 to 7.1 cm). Twelve patients (30%) had a partial response of the primary tumor. The median primary tumor downsizing was 20% (+3.8 to -43.5%). No patient had a primary tumor progression, per RECIST v1.1:

Among the 12 patients with a partial response of the primary tumor, 10 (83%) were disease-free. At a median follow-up of 23.5 months, recurrence occurred in 13 (32%) patients at a median of 8 (2-23) months and 3 died of disease. Neither median DFS nor OS were reached to date.

Intraoperative adverse events occurred in two patients with bowel damage and splenectomy each in one patient. Postoperative adverse events occurred in 13 patients, 4 of which were Clavien Dindo grade 3a (10%) and one of which was grade 4a (2.5%). All serious adverse events were attributable to either prolonged hospitalization or readmission.
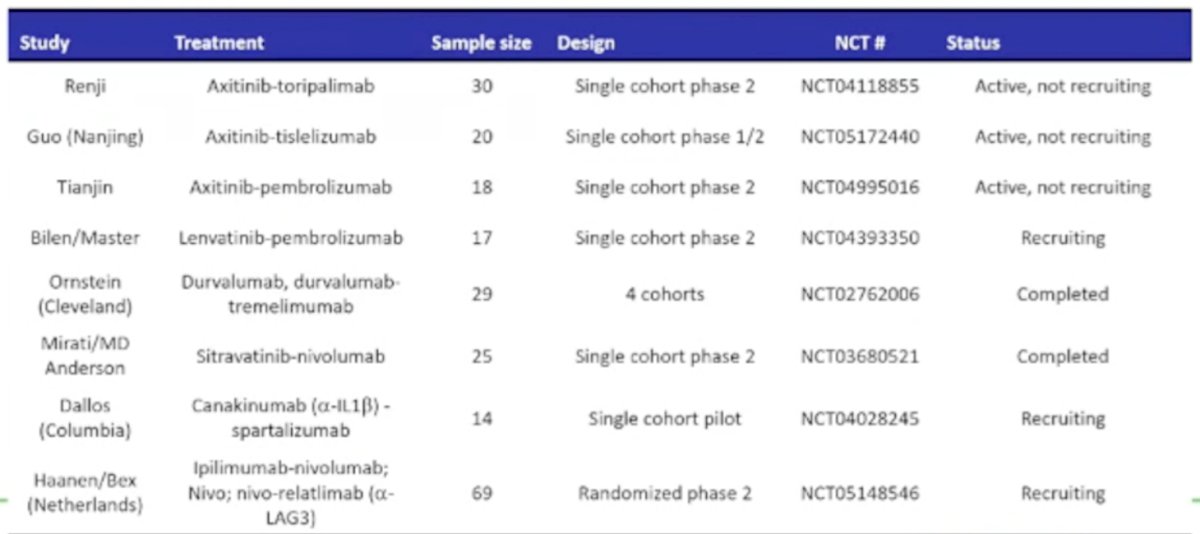
As follows is a table highlighting the ongoing neoadjuvant clinical trials:
Going back to the aforementioned two patient cases, Dr. Zhang notes that both of these patients received perioperative treatment. When assessing which treatment to choose, Dr. Zhang lists the following points to keep in mind:
- Timing of surgery
- Comorbidities
- Tolerance of toxicity
- Are there trials available?
- Further prospective trials are necessary with oncologic endpoints
- VEGF inhibitor alone (based on data for nivolumab alone, there is no objective responses)
- VEGF-IO combination (based on data for NeoAvAx avelumab + axitinib)
Dr. Zhang concluded her presentation of perioperative indications for systemic therapy with the following provoking perioperative trial questions:
- Overcoming past stigma of neoadjuvant therapy with active treatments?
- How long can/should we give perioperative therapy before nephrectomy? Is there hesitancy about “delaying surgery”?
- Which drugs are best to give? Highest rate of response? Shortest half-life?
- What are the right outcomes? Is earlier better than later? From tumor shrinkage to disease free survival to overall survival
We need good answers to these questions to design the next neoadjuvant trial to improve RCC outcomes.
Presented by: Tian Zhang, MD, MHS, Medical Oncologist, UT Southwestern Medical Center, Dallas, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2022 International Kidney Cancer Symposium (IKCS) Europe Annual Hybrid Meeting, Antwerp, Belgium, Fri, Apr 22 – Sun, Apr 24, 2022.