(UroToday.com) The European International Kidney Cancer Symposium 2021 virtual meeting’s keynote lecture was provided by Dr. David McDermott discussing kidney cancer as a model for a curable neoplasm.
Dr. McDermott notes that the proof of principle for kidney cancer being a curable neoplasm dates back to the late 1990’s with the treatment of metastatic renal cell carcinoma (RCC) with high dose IL-2 therapy. Since then, there has been much interest in enhancing the anti-kidney cancer immune response, with VEGF blockade, PD-L1/PD-1 inhibitors, and CTLA-4 blockade:
The fusion of first and second line therapy has resulted in several PD-1 plus VEGF blockade options in the first-line setting. This now includes (but which regimen should be favored?):
- Axitinib plus avelumab versus sunitinib
- Bevacizumab plus atezolizumab versus sunitinib
- Nivolumab plus cabozantinib versus sunitinib
- Lenvatinib plus everolimus or lenvatinib plus pembrolizumab versus sunitinib
- Axitinib plus pembrolizumab versus sunitinib
- Nivolumab plus ipilimumab versus sunitinib
Dr. McDermott then provided the following pros/cons for both PD-1 plus VEGF and PD-1/CTLA-1 therapy:
- PD-1 plus VEGF
- Pros: improved overall survival, high ORR/low progressive disease rate, longer PFS, and lower immune related-adverse event rate
- Cons: unclear adverse event attribution profile, less mature follow-up, and chronic TKI toxicity
- PD-1/CTLA-1
- Pros: improved overall survival, mature follow-up data available, durable responses, potential to stop therapy, and quality of life during maintenance
- Cons: higher immune related-adverse event rate and lower PFS/response rate
There is still considerable debate regarding which clinical endpoints we should use when assessing these trials. Early endpoints are defined as within the first two years after treatment initiation (ie. ORR and metastatic PFS), and are favored by industry and important for symptomatic patients. Late endpoints are defined as developing after two years (ie. duration of response, landmark PFS, and long-term overall survival), and are favored by surgeons and medical oncologists. Durable endpoints are defined as developing after treatment stops (ie. treatment-free survival) and are favored by patients. According to Dr. McDermott, for intermediate and poor risk patients, a PD-1/VEGF combination therapy is favorable for early endpoints, whereas a PD-1/CTLA-4 combination is preferable for late and durable endpoints:
To date, the adjuvant setting for high risk localized RCC has unfortunately had several negative trials for non-IO therapies. However, a news release on April 8th, 2021 stated that the Keynote 564 phase III trial of adjuvant pembrolizumab versus placebo for high risk localized RCC had superior disease-free survival favoring the pembrolizumab arm. We will eagerly await the presentation of this data at an upcoming meeting.
To make cures more common in kidney cancer we need to have better predictors of response, for example, biomarkers, in actionable disease states such as the adjuvant setting for high-risk disease. Work led by Dr. McDermott among patients in the IMotion150 trial (atezolizumab alone or combined with bevacizumab versus sunitinib) found that angiogenesis, T-effector/IFN-γ response, and myeloid inflammatory gene expression signatures were strongly and differentially associated with PFS within and across the treatments.1 A recent publication from Motzer et al. published in Cancer Cell assessed multi-omic analyses leading to identification of robust molecular subtypes in 823 tumors from patients with advanced RCC.2 This also included 134 tumors with sarcomatoid features, from the phase III IMmotion151 trial. This work found that these molecular subgroups (angiogenic/stromal, angiogenic, complement/Ω-oxidation, T-effector/proliferative, proliferative, stromal/proliferative, and snoRNA) associate with differential clinical outcomes to the combination of an anti-angiogenesis agent (bevacizumab) and a checkpoint inhibitor (atezolizumab) versus a VEGF receptor tyrosine kinase inhibitor (sunitinib):
In order to continue to push potentially curative therapy further forward in the disease space, the PROSPER RCC phase III trial is assessing preoperative PD-1 blockade as follows:
Novel targets for developing new therapeutics potentially include HIF2alpha. Nobel prize-winning work from the Kaelin lab at Dana Farber Cancer Institute is working towards targeting the HIF transcription factor to increase cures, including affecting glucose uptake (ie. GLUT1), anaerobic glycolysis (ie. PFK, LDH), angiogenesis (ie. VEGF, PDGF, IL-8, TGFbeta), erythropoiesis (ie. EPO), invasion/homing (ie. MMP2, MMP9, c-MET, CXCR4), and mitogenesis (ie. TGFalpha, cyclin D1). HIF2alpha combination blockade is delineated in the following figure:
Additionally, novel targets may be available to enhance immune response through interrogation of the tumor microenvironment, including therapies such as vaccines, novel ICs, CAR-T therapy, and TILs. Patient-specific cancer vaccines based on neo-antigens are feasible: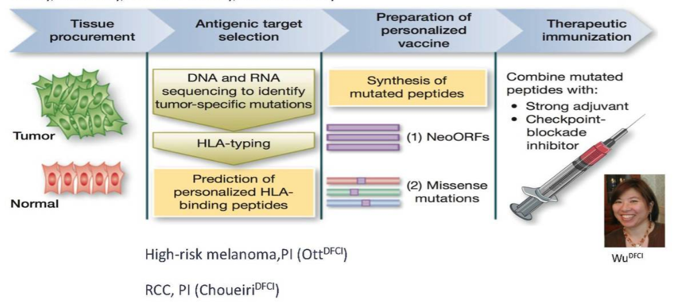
Novel endpoints are also important for making kidney cancer a model for a curable neoplasm, for example, depth of response (deep response = long term overall survival). For example, depth of response was associated with improved overall survival in the CheckMate 214 trial.
Treatment-free survival may also be another novel endpoint based on data from the melanoma literature. Among 1,077 patients who initiated immune checkpoint inhibitor therapy, 47% of patients receiving nivolumab plus ipilimumab, 37% receiving nivolumab, and 15% receiving ipilimumab were surviving free of subsequent therapy initiation. Treatment-free survival has the opportunity to add quality of life and decrease cost in care. Additionally, it may allow IMDC good risk patients a period of observations by stopping treatment early. However, it will be important to test this prospectively and compared PD-1/VEGF to PD-1/CTLA-4 combinations. One trial assessing this hypothesis is the A031704 PDIGREE study, with the following trial design: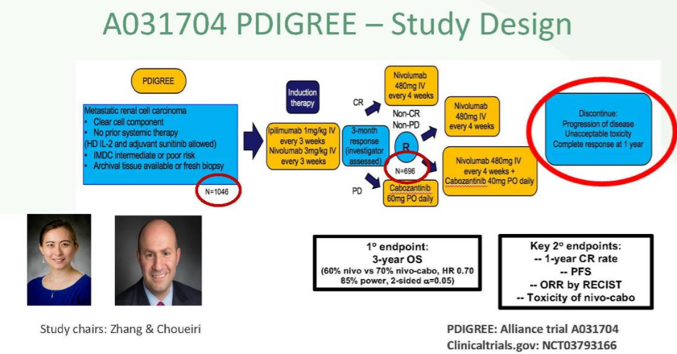
Dr. McDermott notes that we also may be moving toward triplet therapy in the first-line metastatic RCC setting. The COSMIC phase 3 trial (aiming to accrue 676 patients) is randomizing patients to nivolumab plus ipilimumab plus cabozantinib versus nivolumab plus ipilimumab plus placebo. The primary endpoint for this study is progression-free survival based on the blinded imaging review committee. Additional therapies/prognostications that potentially hold promise include TIL therapy and the detection of RCC using plasma and urine cell free DNA methylomes.
Dr. McDermott concluded by highlighting that making cures more common in kidney cancer will require adequate trial design, identification of novel targets, classifying novel endpoints, and using novel algorithms for treatment.
Presented by: David F. McDermott, MD, Professor of Medicine at Harvard Medical School, is Director of the Cutaneous and Immuno-Oncology Programs at Beth Israel Deaconess Medical Center, Leader of the Dana-Farber/Harvard Cancer Center Kidney Cancer Program and Principal Investigator of the National Cancer Institute Kidney Cancer SPORE grant
Written By: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md during the 2021 European International Kidney Cancer Symposium (EIKCS), April 23-24, 2021
References:
- McDermott DF, Huseni MA, Atkins MB, et al. Clinical activity and molecular correlates of response to atezolizumab alone or in combination with bevacizumab alone or in combination with bevacizumab versus sunitinib in renal cell carcinoma. Nat Med. 2018 Jun;24(6):749-757.
- Motzer RJ, Banchereau R, Hamidi H, et al. Molecular subsets in renal cancer determine outcome to checkpoint and angiogenesis blockade. Cancer Cell. 2020 Dec 14;38(6):803-817.