Dr. Powles notes that to date, the only prospectively evaluated biomarker tested is the International Metastatic Renal Cell Carcinoma Database Consortium model as a prognostic tool. In a population-based study across 19 centers, Ko et al. assessed the primary endpoint of overall survival among 1,021 patients who received second-line targeted therapy for metastatic renal cell carcinoma RCC1. The median overall survival (OS) since the start of second-line targeted therapy was 12.5 months (95% CI 11.3-14.3). Five of six factors in the International Metastatic Database Consortium (IMDC) model (anemia, thrombocytosis, neutrophilia, Karnofsky performance status <80, and <1 year from diagnosis to first-line targeted therapy) were independent predictors of poor overall survival. The concordance index using all six prognostic factors in the IMDC model was 0.70 (95% CI 0.67-0.72) and when patients were divided into three risk categories using IMDC criteria, median overall survival was 35.3 months (95% CI 28.3-47.8) in the favorable risk group (n=76), 16.6 months (14.9-17.9) in the intermediate-risk group (n=529), and 5.4 months (4.7-6.8) in the poor-risk group (n=261).

Tumor mutational burden has been retrospectively correlated with response to immune checkpoint blockade. Among 10 tumor-type-specific cohorts from the phase 2 KEYNOTE-158 study (which assessed pembrolizumab in patients with selected, previously treated, advanced solid tumors), Marabelle et al. 2 showed that 102 (13%) of 790 patients had tissue tumor mutational burden-high status (≥10 mutations per megabase), and 688 (87%) patients had non- tissue tumor mutational burden-high status (<10 mutations per megabase). Objective responses were observed in 30 (29%; 95% CI 21–39) of 102 patients in the tumor mutational burden-high status group and 43 (6%; 5–8) of 688 in the non-tumor mutational burden-high status group. Dr. Powles notes that RCC was not included as a tumor subgroup in this study and highlights that we have a lot of work to do in the tumor mutational burden assessment of RCC.
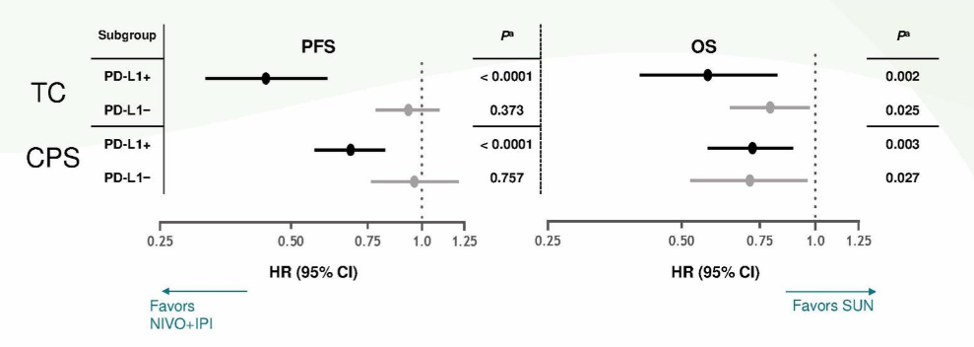
Previously presented at the ASCO 2020 annual meeting, Motzer and colleagues assess biomarker analyses from the phase 3 CheckMate 214 trial of nivolumab plus ipilimumab or sunitinib in advanced RCC. Forest plots based on PD-L1 positivity for progression-free survival (PFS) and OS are as follows:
Additionally, work lead by Dr. Brian Rini and first presented at ESMO 2018 suggested that angiogenesis biomarkers may be prognostic for RCC. Using patients from the IMmotion151 cohort testing atezolizumab plus bevacizumab versus atezolizumab versus sunitinib, patients treated with sunitinib that was deemed angiogenesisHigh compared to angiogenesisLow had improved progression-free survival (HR 0.59, 95% CI 0.47-0.75). Using the same trial data, they also found a progression-free survival benefit for atezolizumab plus bevacizumab versus sunitinib among patients deemed T-effect or high (HR 0.76, 95% CI 0.59-0.99), but no benefit among T-effect or low patients (HR 0.91, 95% CI 0.73-1.14).
Biomarker data from the JAVELIN Renal 101, which tested avelumab plus axitinib versus sunitinib in advanced RCC, was also previously presented at the ASCO 2019 annual meeting. This study consisted of four biomarker analyses: (i) PD-L1 expression (n=804), (ii) CD8 expression (n=795), (iii) a novel 26-gene JAVELIN gene signature (n=720), and (iv) mutations and polymorphisms (n=733). PFS according to PD-L1 immunohistochemistry showed no difference in the avelumab plus axitinib arm (HR 0.89, 95%CI 0.652-1.220), however in the sunitinib arm, patients that were PD-L1+ had worse PFS (HR 1.57, 95%CI 1.156-2.142). PFS according to CD8+ cells showed no difference for patients in the sunitinib arm (HR 1.42, 95%CI 0.955-2.115), however, patients greater than the median value had a PFS benefit in the avelumab plus axitinib arm (HR 0.59, 95%CI 0.361-0.967). PFS according to the 26-gene JAVELIN Renal 101 signature showed that high expression in the avelumab plus axitinib arm leads to a PFS benefit (HR 0.60, 95%CI 0.439-0.834), but no difference in the sunitinib arm (HR 0.89, 95%CI 0.670-1.172). Finally, PFS according to mutations and polymorphisms found that several genes were associated with PFS benefit in the avelumab plus axitinib arm: CD163L1 (HR 0.20, 95%CI 0.05-0.80), DNMT1 (HR 0.34, 95%CI 0.17-0.91), IL-16 (HR 0.54, 95%CI 0.35-0.85), and MC1R (HR 0.25, 95%CI 0.03-0.79).
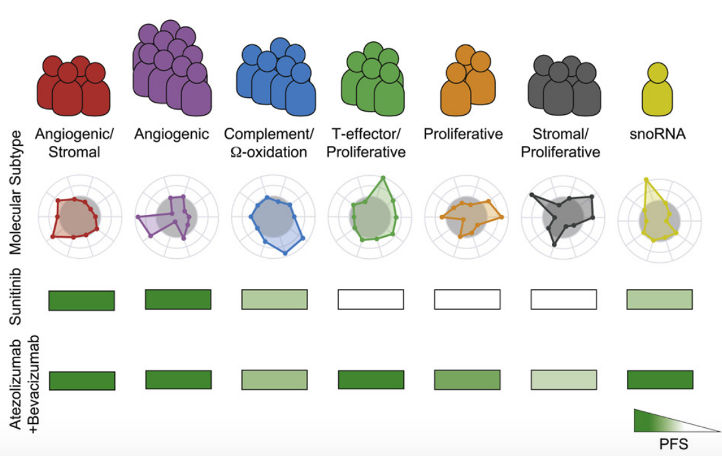
A recent publication from Motzer et al. published in Cancer Cell assessed multi-omic analyses leading to the identification of robust molecular subtypes in 823 tumors from patients with advanced RCC 3. This also included 134 tumors with sarcomatoid features, from the phase III IMmotion151 trial. This work found that these molecular subgroups (angiogenic/stromal, angiogenic, complement/Ω-oxidation, T-effector/proliferative, proliferative, stromal/proliferative, and snoRNA) associate with differential clinical outcomes to the combination of an anti-angiogenesis agent (bevacizumab, anti-VEGF) and a checkpoint inhibitor (atezolizumab or anti-PD-L1) versus a VEGF receptor tyrosine kinase inhibitor (sunitinib):

Finally, several other trials have incorporated biomarkers into their design/analysis plan, including BIONIKK (ccrcc1-4) and savolitinib versus sunitinib in patients with MET-driven papillary RCC (SAVOIR phase 3 randomized controlled trial).
Dr. Powles concluded his presentation with the following summary points:
• Renal cancer is immunologically distinct from other cancers and we will need to approach RCC differently
• There has been a focus more on drug development than patient selection, which has been important, but it will catch up to us at some point
• Biomarkers in renal cancer have been elusive, but perhaps we have not looked hard enough. For example, PD-L1 appears to have more prognostication potential in RCC than in bladder cancer
• 2nd generation biomarkers, especially active T-cell gene signatures and angiogenic signatures are partially validated, but there are no prospective studies to change practice
• The 7-cluster series recently published is being touted by some experts in the field as a breakthrough in the biomarker setting
Presented by: Thomas Powles, MBBS, MRCP, MD, Professor of Genitourinary Oncology, Lead for Solid Tumour Research at Barts Cancer Institute, Director of Barts Cancer Institute, London, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md during the 2021 European International Kidney Cancer Symposium (EIKCS), April 23-24, 2021
References:
1. Ko JJ, Xie W, Kroeger N, et al. The International Metastatic Renal Cell Carcinoma Database Consortium model as a prognostic tool in patients with metastatic renal cell carcinoma previously treated with first-line targeted therapy: A population-based study. Lancet Oncol. 2015 Mar;16(3):293-300.
2. Marabelle A, Fakih M, Lopez J, et al. Association of tumor mutational burden with outcomes in patients with advanced solid tumors treated with pembrolizumab: Prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol. 2020 Oct;21(10):1353-1365.3. Motzer RJ, Banchereau R, Hamidi H, et al. Molecular subsets in renal cancer determine the outcome to checkpoint and angiogenesis blockade. Cancer Cell. 2020 Dec 14;38(6):803-817.