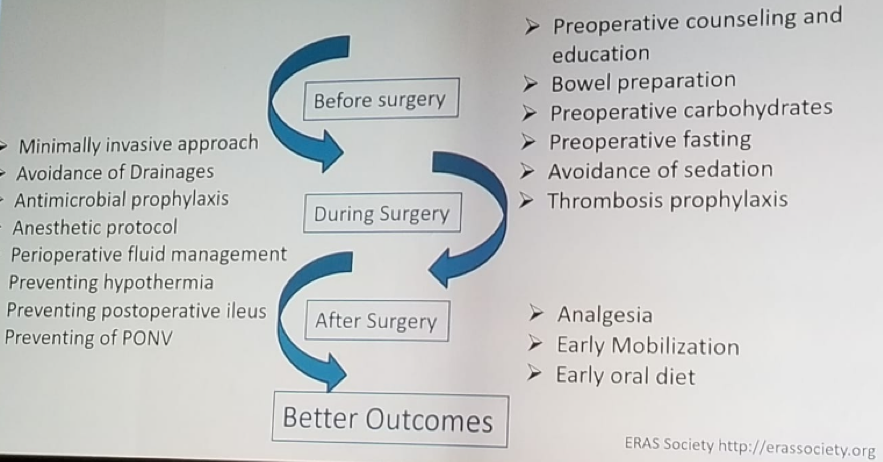
Dr. Graefen moved on to discuss the specifics of the ERAS protocol in this large volume center. Generally, ERAS has been shown to beneficial for patients, but it requires a team effort to work. The team consists of surgeons, anesthetists, fellows, residents, nurses, and others. The ERAS protocol entails many different factors preoperatively, intraoperative and postoperatively (Figure 1). All these factors put together in harmony will eventually result in better patient outcomes.
Figure 1 – ERAS protocol factors:
Dr. Graefen and Dr. Von Breunig then delved into the details of the ERAS protocol utilized in their center:
On a preoperative day:
The patient has a normal diet with 6 hours of preoperative fasting for solid food, and 2 hours fasting for clear fluids. The patient also receives laxative suppositories and is instructed to use the “Coach 2” spirometer to enhance pulmonary function. The patient is not given any sedation premedication.
On an operative day:
The patient is given dexamethasone as to prevent postoperative nausea and vomiting (PONV). Special attention is given to avoid hypothermia, critical hypovolemia and hypervolemia, and goal-directed fluid therapy (GDFT) is the key. GDFT has been shown to result in an earlier return to normal bowel function, lower the incidence of PONV, and decrease the length of hospital stay. A recently published meta-analysis on GDFT demonstrated that it reduces mortality, morbidity, and length of hospital stay1.
At the end of the surgery, surgeons attempt to avoid placing a drain. Several studies have shown that there is no risk in not placing a drain after radical prostatectomy2, 3.
Postoperatively:
In the recovery room, the patient receives sips of water, adequate analgesia, anti-emetics as necessary, and performs spirometer exercises every 15 min once the patient is awake. Once the patient is moved to the ward, food is reintroduced early (tea, water, juice and a light evening meal). The patient continues with chest physiotherapy (at least once an hour) and is mobilized as soon as possible. Adequate analgesia is continued with nonsteroidal medications being the first line, and anti-emetics are given as needed.
On a postoperative day one, patient resumes his normal diet and given chewing gum. Chest physiotherapy and analgesia are continued until the patient is completely mobile. In any case, he is mobilized at 3 times daily. Lastly, laxatives are given in the evening.
Dr. Graefen and Dr. Von Breunig concluded their informative talk by stating that it is the continuing goal of the staff at the Martini-Klinik to prevent the development of delirium through the ERAS protocol and to continue and improve the protocol.
Presented by: M. Graefen, Hamburg, Germany, F. Von Breunig, Martini-Klinik, Hamburg, Germany
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre, Twitter:@GoldbergHanan at the EAU Robotic Urology Section (ERUS) Meeting - September 5 - 7, 2018 - Marseille, France
References:
1. Chong MA, Wang Y, Berbenetz NM, et al. Does goal-directed hemodynamic and fluid therapy improve peri-operative outcomes?: A systematic review and meta-analysis. European journal of anaesthesiology 2018; 35(7): 469-83.
2. Chenam A, Yuh B, Zhumkhawala A, et al. Prospective randomized non-inferiority trial of pelvic drain placement vs no pelvic drain placement after robot-assisted radical prostatectomy. BJU international 2018; 121(3): 357-64.
3. Danuser H, Di Pierro GB, Stucki P, et al. Extended pelvic lymphadenectomy and various radical prostatectomy techniques: is pelvic drainage necessary? BJU international 2013; 111(6): 963-9.