(UroToday.com) The 2023 European Association of Urology (EAU) annual congress held in Milan, Italy between March 10th and 13th, 2023 was host to a session addressing precision medicine in patients with metastatic castrate-resistant prostate cancer (mCRPC). Professor Thomas Steuber delivered a state-of-the-art lecture addressing optimal treatment sequencing in the area of triplet therapies for hormone-sensitive prostate cancer.
The mHSPC treatment landscape has seen a significant evolution since the publication of the CHAARTED docetaxel + ADT trial in 2014:
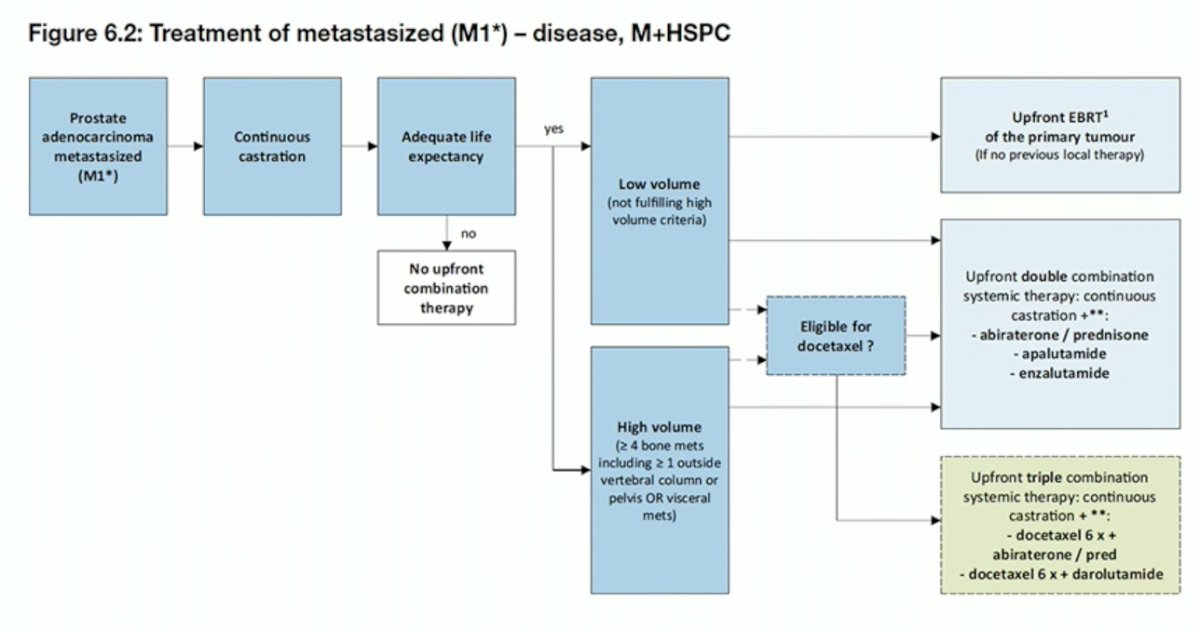
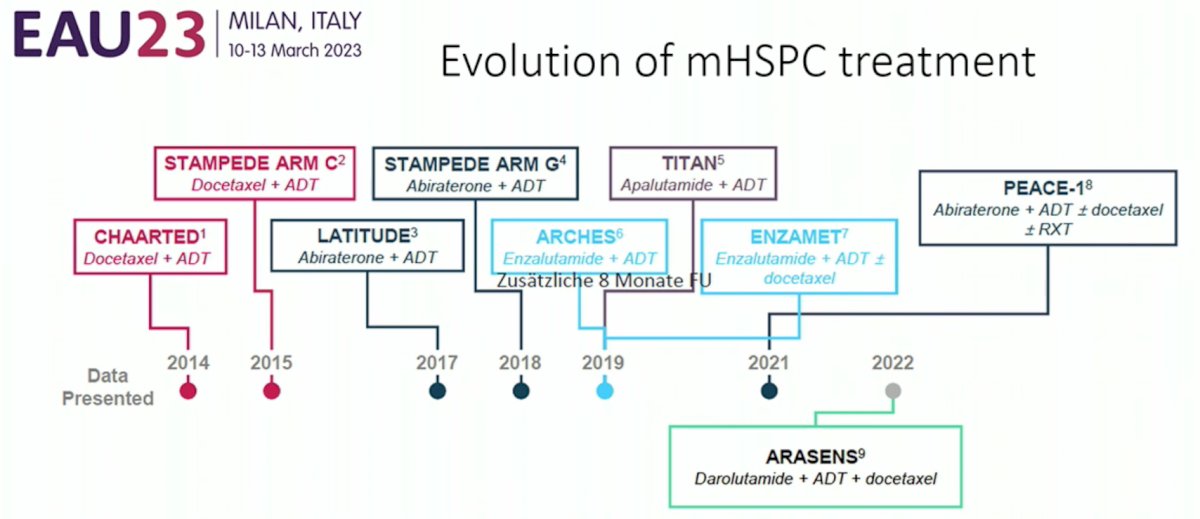 Despite the combination of ADT + docetaxel being the first combination regimen to demonstrate an OS benefit in the mHSPC disease state, this doublet regimen has fallen out of favor with the lower side effect profile of novel hormonal agents (NHAs) and the emergence of triplet therapies. As such, the new EAU 2023 guidelines currently recommend the following in the first-line treatment setting hormone-sensitive setting:
Despite the combination of ADT + docetaxel being the first combination regimen to demonstrate an OS benefit in the mHSPC disease state, this doublet regimen has fallen out of favor with the lower side effect profile of novel hormonal agents (NHAs) and the emergence of triplet therapies. As such, the new EAU 2023 guidelines currently recommend the following in the first-line treatment setting hormone-sensitive setting:
- Offer ADT combined with abiraterone acetate plus prednisone or apalutamide or enzalutamide to patients with M1 disease and who are fit for the regimen (strong recommendation)
- Offer docetaxel only in combination with ADT plus abiraterone or darolutamide to patients with M1 disease and who are fit for docetaxel (strong recommendation)
Of note, there are currently no clear recommendations by the EAU guidelines as to when to use docetaxel in the mHSPC disease space.
What about triplet therapy? The question of what is the added value of adding docetaxel to ADT plus an NHA has not been directly evaluated within the context of a clinical trial. The data from ARASENS and PEACE-1 should be discussed with patients who are fit/young for chemotherapy and an NHA. There appears to be more evidence for using triplet therapy in synchronous, high-volume disease. The choice will most likely be driven by:
- Patient performance status/fitness for docetaxel
- Disease volume (CHAARTED high/low) and timing (synchronous/metachronous)
- Patient preference
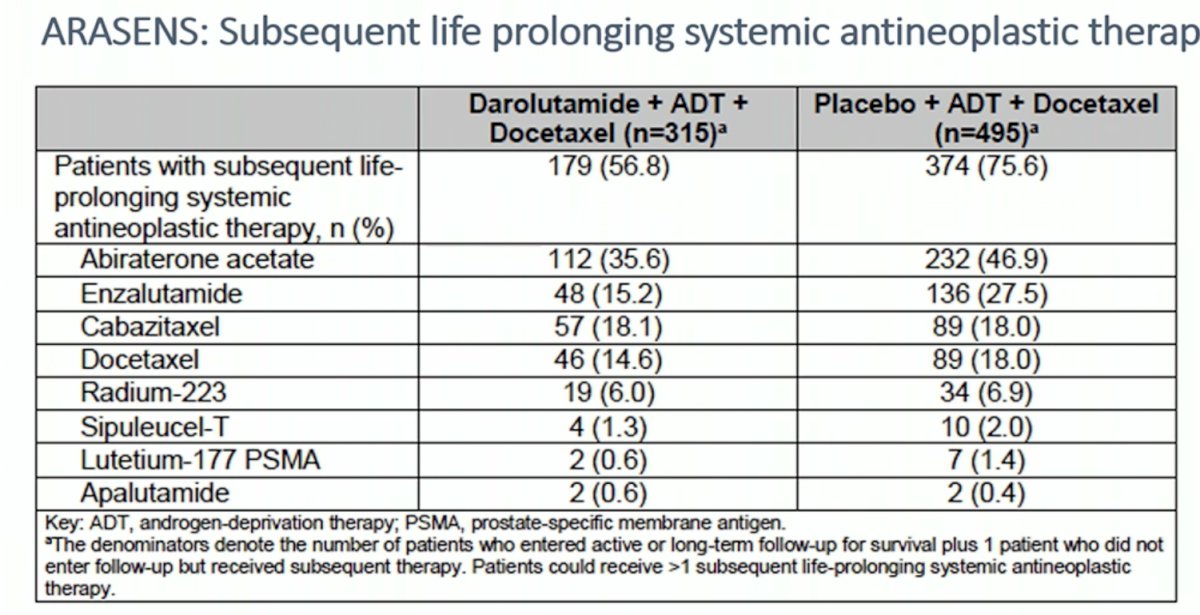
With the recent emergence of triplet therapies utilizing docetaxel, an NHA (abiraterone acetate or darolutamide) and ADT, what is the current optimal treatment sequencing in the area of triplet therapies for hormone-sensitive disease? Looking at data from ARASENS (docetaxel/darolutamide/ADT), it appears that almost 50% received an alternate NHA (abiraterone or enzalutamide), almost 20% received cabazitaxel, and 15% docetaxel. Agent such as PARP inhibitors and Lu-PSMA were sparingly used as expected secondary to their recent approval in this setting.1
Data regarding subsequent mCRPC therapy (i.e., PFS2) are not yet available and will be important to assess for the optimal sequencing of post-triple therapies. As such, the question remains: what is the ideal post-triplet therapy agent(s)?
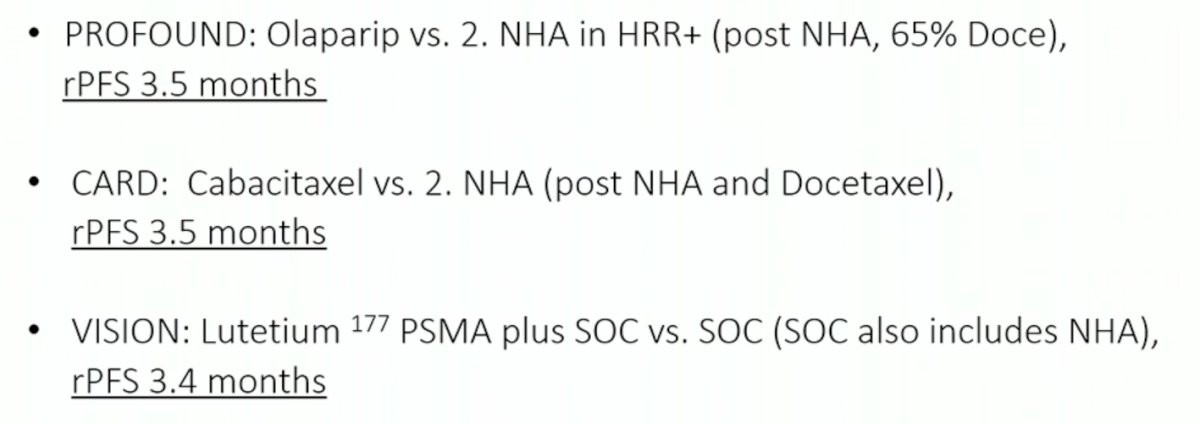
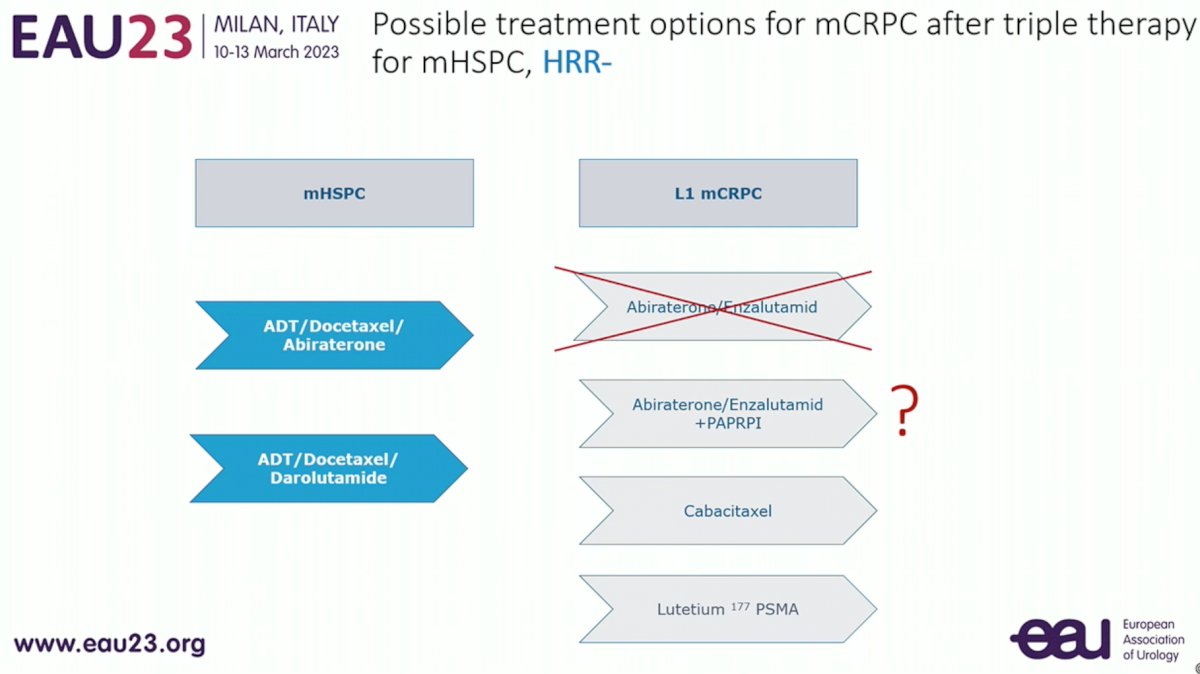
Starting with possible treatment options for non-HRR mutated mCRPC patients progressing following triplet therapy, it is clear that use of an alternate, single agent NHA (e.g. apalutamide or enzalutamide) is not ideal in this setting. As seen in the control arms of PROFOUND, CARD, and VISION, which all utilized an alternate NHA as the comparator, outcomes were consistently poor in such control arms.
What about combination PARP inhibitor + NHA (e.g. olaparib + abiraterone)? As seen in the biomarker-unselected cohort of patients in the PROpel trial, rRPFS outcomes are more “convincing” for patients with HRR mutations, particularly the BRCA1/2 mutated cohort, yet still observed more modestly in the non-HRR mutated cohort.

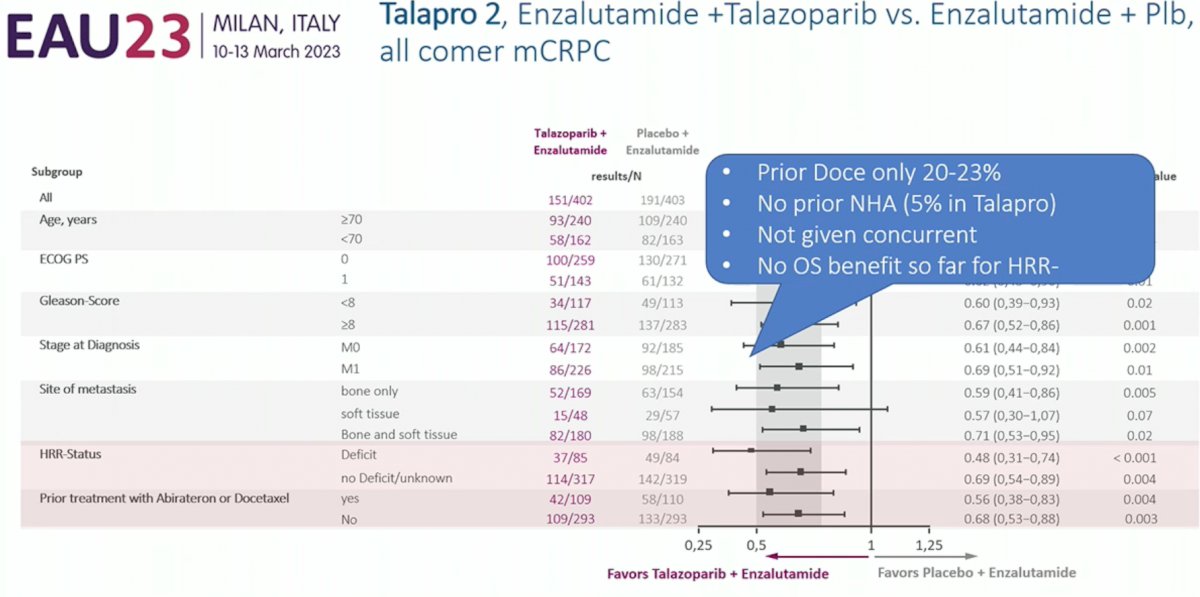
Similarly, rPFS benefits were significantly more pronounced in the HRRm patients in the TALAPRO-2 trial of talazoparib + enzalutamide, yet still present in the non-HRR mutated cohort of patients. Furthermore, an rPFS benefit was seen in the cohort of patients who had previously received docetaxel (HR: 0.56, p=0.004). However, prior docetaxel exposure was present in only 20-23% of patients. Only 5% of patients had received a prior NHA in TALAPRO-2. Furthermore, these benefits are restricted to rPFS with OS benefits not yet observed for non-HRR mutated patients.
As such, the verdict is “possibly” for combination PARPi/NHA in the post-triplet setting for non-HRR mutated patients. Other potential agents include the current “third line” treatment options of cabazitaxel and Lu-PSMA, although Professor Steuber argued that he would favor LuPSMA over cabazitaxel in this setting given the superior PSA50 response rates (no OS differences) and the better quality of life experienced with LuPSMa compared to cabazitaxel.

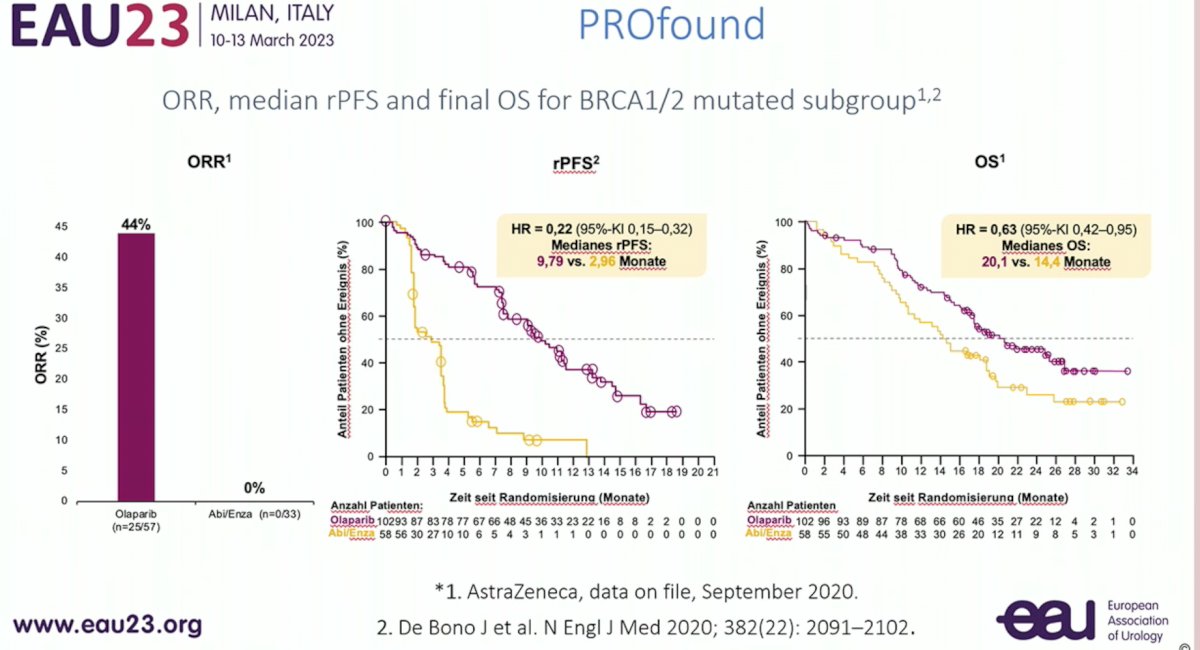
What about the HRR mutated cohort post-triplet therapy? Results from PROfound suggest that olaparib may be a reasonable option in these patients. PROfound was a randomized, open-label, phase III trial that evaluated the efficacy and safety of olaparib versus enzalutamide or abiraterone in patients with mCRPC with alterations in any of 15 predefined genes with a direct or indirect role in homologous recombination repair whose disease had progressed on prior NHA therapy. rPFS and OS benefits were observed in Cohort A of patients with BRCA1/2 or ATM mutations as demonstrated below. 100% of patients had received a prior NHA (abi or enza), 65% ahd received a prior taxane, and no concurrent NHA/Docetaxel in the mHSPC disease state.
Similar results were observed in the recently published TRITON-3 trial of rucaparib in a similar treatment setting.3

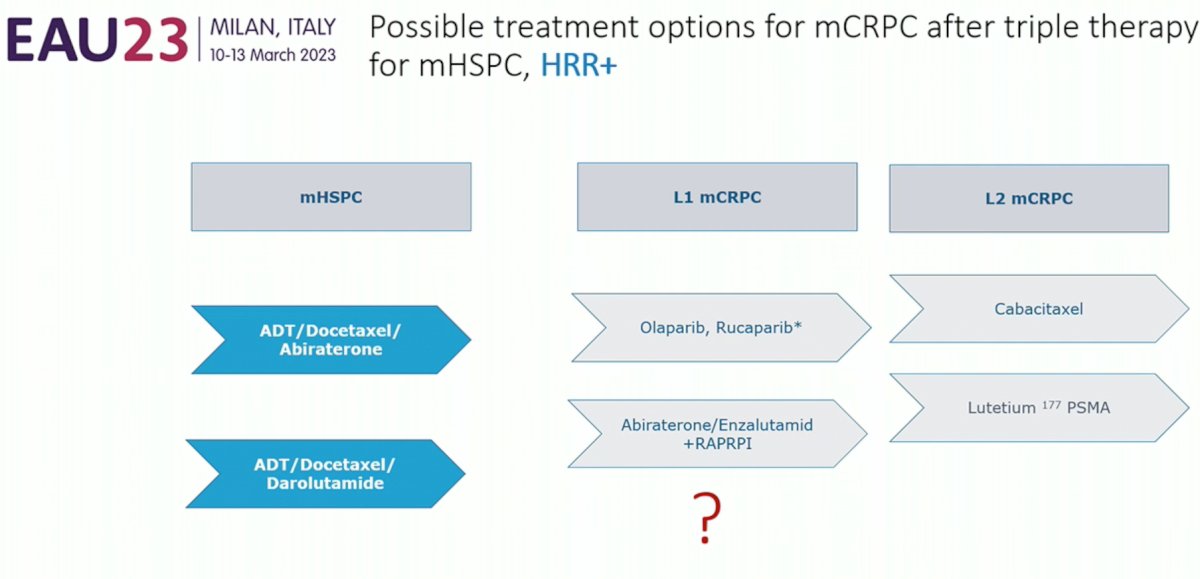
As such, single agent PARPi (olaparib, rucaparib) appear to be possible treatment options for HRR mutated mCRPC patients after triplet therapy. What about combination PARPi and NHA (i.e., PROpel, TALAPRO-2). This combination remains questionable given that OS only 20-23% of patients were pre-treated with docetaxel and only 5% received prior NHA. As with the non-HRRm cohort, cabazitaxel and Lu-PSMA remain viable 2nd line mCRPC treatment options in this setting.
Professor Steuber concluded with the following take home messages:
- No prospective or retrospective data are available to guide sequential treatment decisions in triplet therapy pre-treated mCRPC patients
- 1st line mCRPC treatment options following triplet therapy in non-HRR mutated patients include Lu-PSMA and cabazitaxel, with the possibility for PARPi/NHA use
- 1st line mCRPC treatment options following triplet therapy in HRR mutated patients include: PARPi followed by LuPSMA or cabazitaxel, with the possibility for PARPi/NHA use
Presented by: Professor Thomas Steuber, Department of Urology, University Hospital Hamburg, Germany
Written by: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 European Association of Urology (EAU) 38th annual congress held in Milan, Italy between March 10th and 13th, 2023
References- Smith MR, et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med 2022. 386:1132-1142.
- De Bono, et al. Survival with Olaparib in Metastatic Castration-Resistant Prostate Cancer. N Engl J Med 2020. 383:2345-2357.
- Fizazi K, et al. Nonmetastatic, Castration-Resistant Prostate Cancer and Survival with Darolutamide. N Engl J Med 2023. 383:1040-1049.