(UroToday.com) The 2023 European Association of Urology (EAU) annual congress held in Milan, Italy between March 10th and 13th, 2023 was host to a session addressing precision medicine in patients with metastatic castrate-resistant prostate cancer (mCRPC). Dr. Christopher Evans delivered a state-of-the-art lecture discussing how and when to sequence with molecular testing in patients with mCRPC.
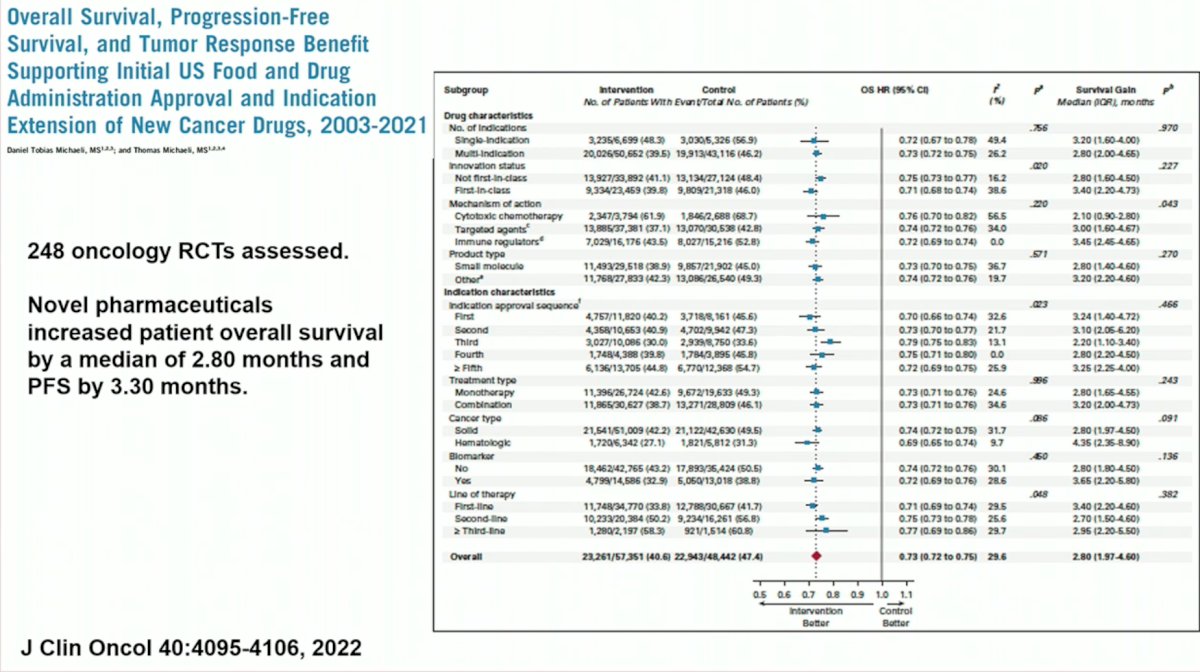
Dr. Evans began his presentation on a sobering note. Quite clearly, we have not made as much progress in the field of oncology as we had previously thought. In a systematic review published in The Journal of Clinical Oncology in 2022, 248 oncology randomized controlled trials of novel pharmaceuticals between 2003 and 2021 were assessed. In the meta-analysis, it was estimated that novel pharmaceuticals over the past two decades have only improved patient overall survival by a median of 2.8 months and progression-free survival by 3.3 months.
MOSCATO 01 was a prospective clinical trial evaluating the clinical benefit of high-throughput genomic analyses to improve outcomes in patients with advanced cancers. Nucleic acids were extracted from fresh-frozen tumor biopsies and analyzed by array comparative genomic hybridization, next-generation sequencing, and RNA sequencing. The primary objective was to evaluate clinical benefit as measured by the percentage of patients presenting progression-free survival (PFS) on matched therapy (PFS2) 1.3-fold longer than the PFS on prior therapy (PFS1).
Of 1,110 included patients, an actionable target was identified in only 411 patients, of which 193 were evaluable for PFS2/PFS1.
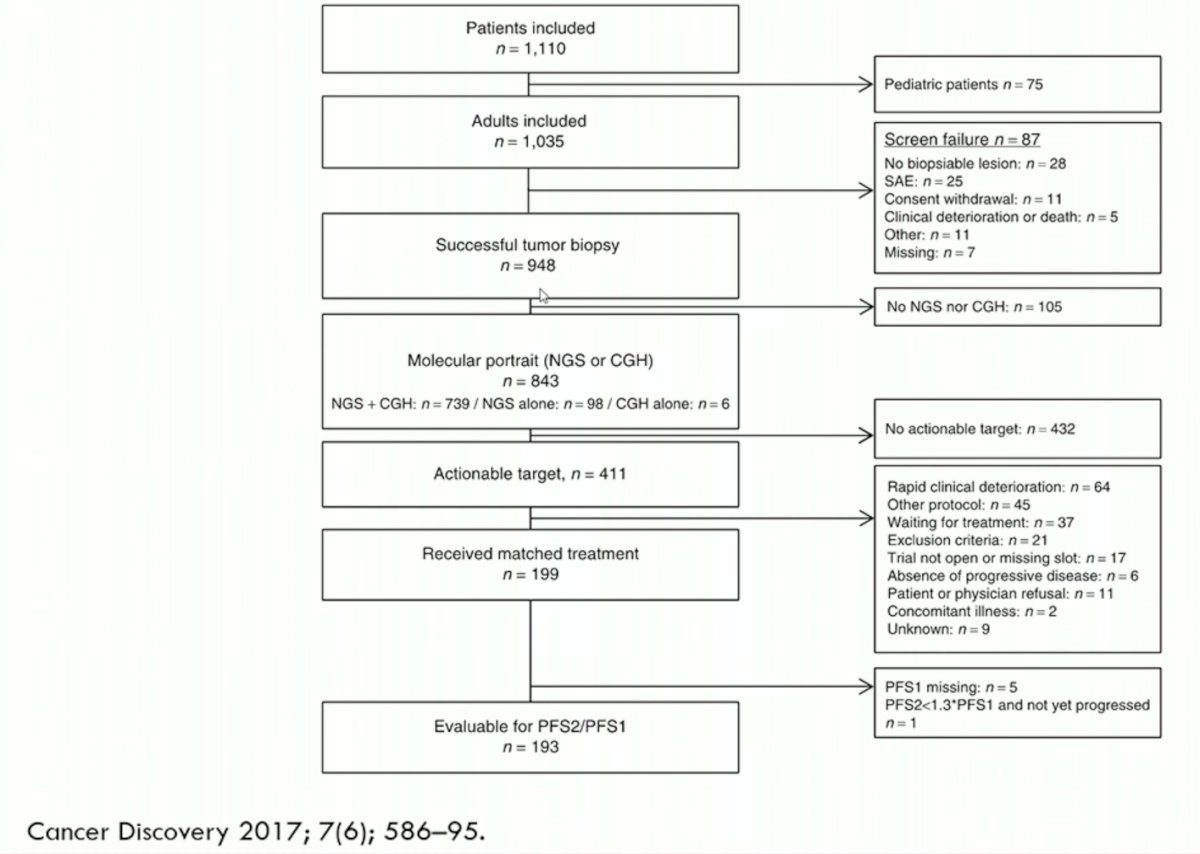
These results were even more disappointing among urologic cancer patients, with 158 such patients biopsied, 15% having matched treatment, and eventually, only 10 (of the total 158: 6.3%) meeting the criteria of PFS success.
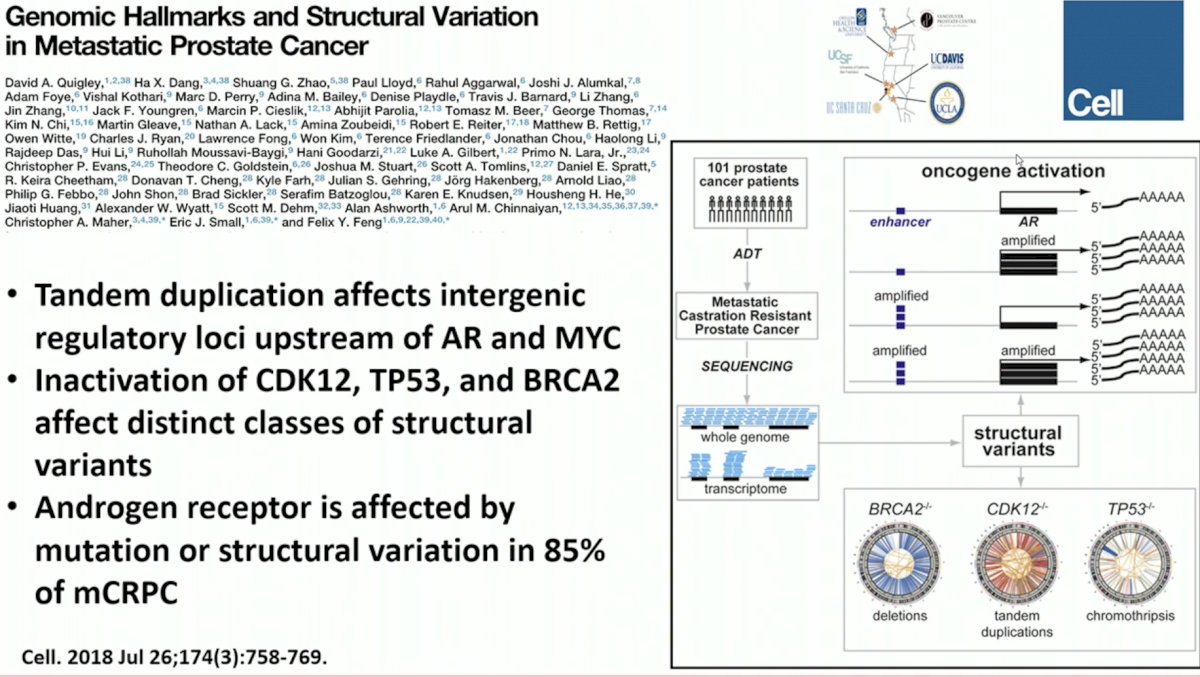
In 2018, Dr. Felix Feng’s group described the genomic hallmarks and structural variation in metastatic prostate cancer. While this work was undoubtedly pivotal in furthering our understanding of the underlying disease biology, the reality is that the majority of the identified mutations remain clinically non-applicable with no relevant drug targets.
In addition to considering the genomic profile of these tumors for adopting a personalized approach, we cannot underestimate the importance of DNA methylation/epigenetic expression in explaining the underlying disease pathogenesis.

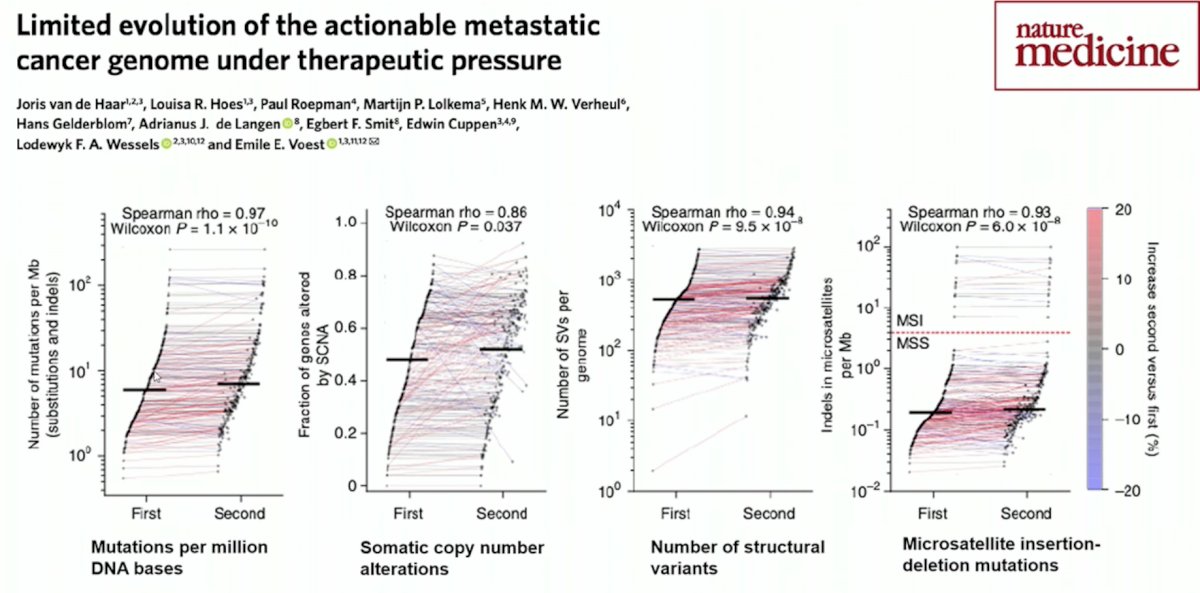
A common clinical principle is sequentially using agents with different mechanisms of action, as it is presumed that disease progression is related to underlying treatment-resistant clones that have adapted/mutated to the “therapeutic pressure”. In fact, this may not be accurate in the metastatic prostate cancer setting. Van de Haar et al. performed whole genome sequencing of 250 paired biopsies from mostly metastatic to metastatic lesions. The median time interval between biopsies was 6.4 months, which admittedly is a relatively short period when evaluating for mutational changes secondary to external factors. One or more standard of care treatment were given between biopsies. As demonstrated in the figure below, the number of mutations varied minimally between the first and second biopsy specimens and there were infrequently any new actionable targets (~10%).1

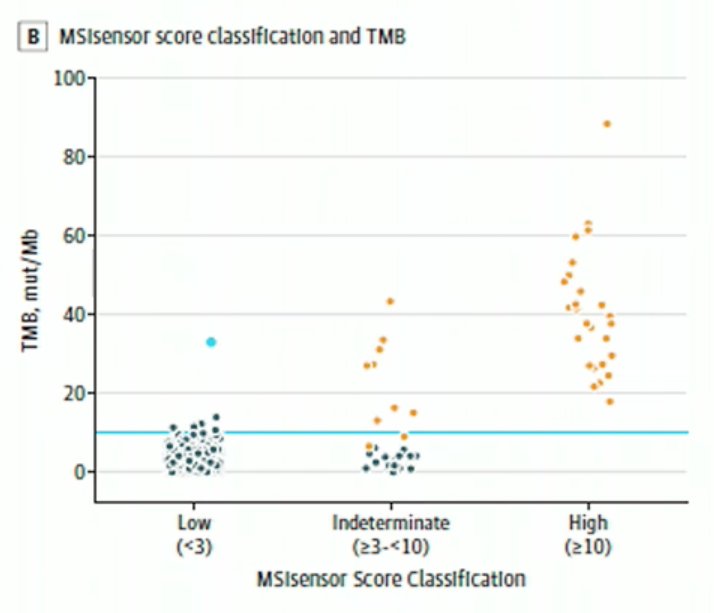
Dr. Evans acknowledged the “pan-cancer” approval of pembrolizumab for all cancer patients with microsatellite instability. How does this apply to prostate cancer patients? Only 2-3% of mCRPC patients are MSI-H. However, as demonstrated by Abida et al in 2019, patients with a higher MSIsensor score and tumor mutational burden (TMB) experienced significant improvements with anti-PD-1/PD-L1 therapy, as demonstrated below:
Approximately 12% of patients with metastatic prostate cancer have germline DNA repair gene mutations, with BRCA1/2 accounting for approximately half of such mutations. With the emergence of PARP inhibitors, both as single acting or in combination, such mutations have increasingly important treatment implications.

Published in 2020, PROfound was a randomized, open-label, phase III trial evaluating efficacy and safety of olaparib (PARPi) versus enzalutamide or abiraterone in patients with mCRPC with alterations in any of 15 predefined genes with a direct or indirect role in homologous recombination repair whose disease had progressed on prior new hormonal agent therapy. In patients with BRCA1/2 or ATM mutations (cohort A), rPFS was significantly longer in the olaparib group than in the control group (median, 7.4 months vs. 3.6 months; hazard ratio for progression or death, 0.34; 95% confidence interval, 0.25 to 0.47; P<0.001). The median overall survival in cohort A was 18.5 months in the olaparib group and 15.1 months in the control group.3

When attempting to identify actionable genomic targets to guide a personalized treatment approach, is tumor tissue sequencing sufficient? It appears that the answer is no. Dr. Taplin and colleagues analyzed results of independent germline testing and tumor-only sequencing from 100 men with advanced PCa from a prospective clinical trial. Tumor-only sequencing failed to report approximately 20% of the pathologic germline variants. As such, it appears that combining tumor and germline sequencing is essential to maximizing the detection of clinically actionable alterations.4

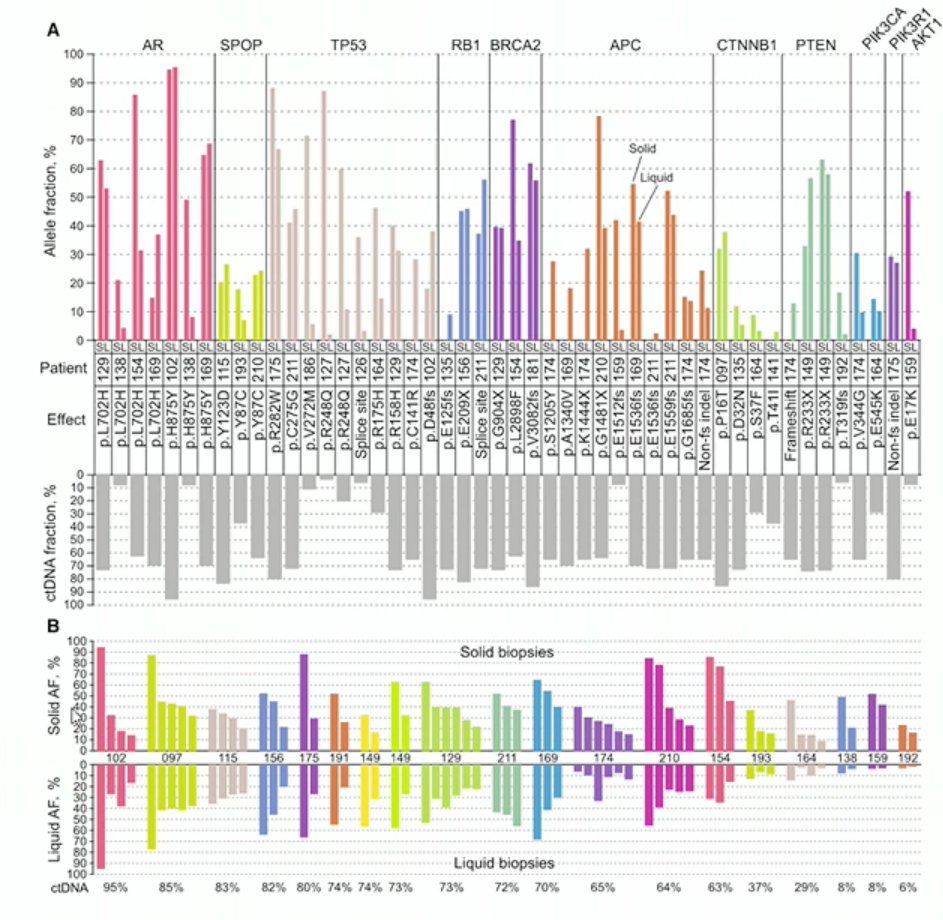
What about circulating tumor DNA (ctDNA) in lieu of metastatic tissue biopsy in prostate cancer? In 2017, Wyatt et al. evaluated the concordance of these two modalities for variant allele frequencies. They performed whole exome sequencing of solid metastatic biopsy tissue and then performed targeted sequencing for 72 relevant genes from plasma cfDNA assessing ctDNA. Somatic mutations were subsequently compared. As seen in the figure below, variant allele frequencies for somatic mutations were essentially shared between matched liquid and solid biopsies.
Furthermore, it appears that high levels of ctDNA correlates with worse outcomes on AR inhibitors as demonstrated below:

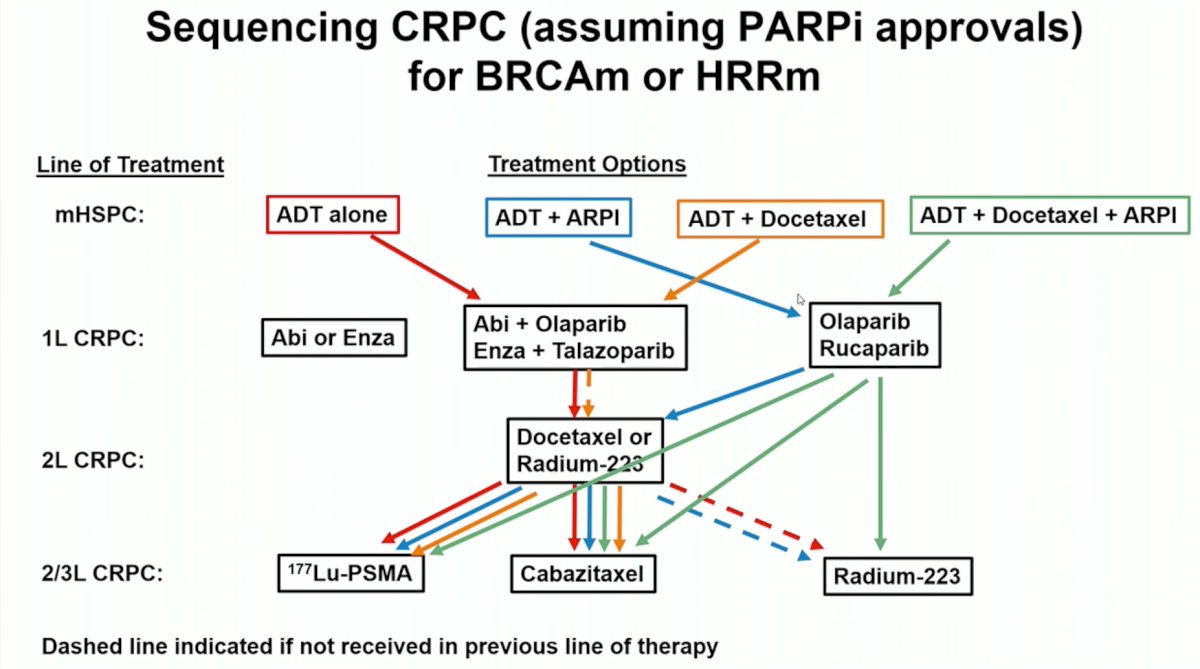
Based on the currently available evidence, Dr. Evans concluded his presentation with the following treatment sequencing frameworks for mCPRC patients by BRCAm/HRRm status:

Presented by: Christopher P. Evans, MD, Chair, Department of Urologic Surgery, University of California, Davis, Sacramento, CA, USA
Written by: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 European Association of Urology (EAU) 38th annual congress held in Milan, Italy between March 10th and 13th, 2023
References:
- Van de Haar, et al. Limited evolution of the actionable metastatic cancer genome under therapeutic pressure. Nat Med. 2021. 27, pages1553–1563.
- Abida, et al. Analysis of the Prevalence of Microsatellite Instability in Prostate Cancer and Response to Immune Checkpoint Blockade> JAMA Oncol. 2019. 5(4):471-478.
- de Bono et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. NEJM. 2020. 382:2091-2102.
- Berchuck et al. Addition of Germline Testing to Tumor-Only Sequencing Improves Detection of Pathogenic Germline Variants in Men With Advanced Prostate Cancer. JCO Precis Oncol. 2022. DOI: 10.1200/PO.22.00329.
- Wyatt et al. Concordance of Circulating Tumor DNA and Matched Metastatic Tissue Biopsy in Prostate Cancer. JNCI. 2017. https://doi.org/10.1093/jnci/djx118