(UroToday.com) The 2023 EAU annual meeting included a session discussing clinically meaningful questions in the management of advanced, hormone-sensitive prostate cancer, featuring a debate of treatment for low-volume disease at conventional imaging, with 5 bone metastases at PSMA PET/CT.
Case Presentation
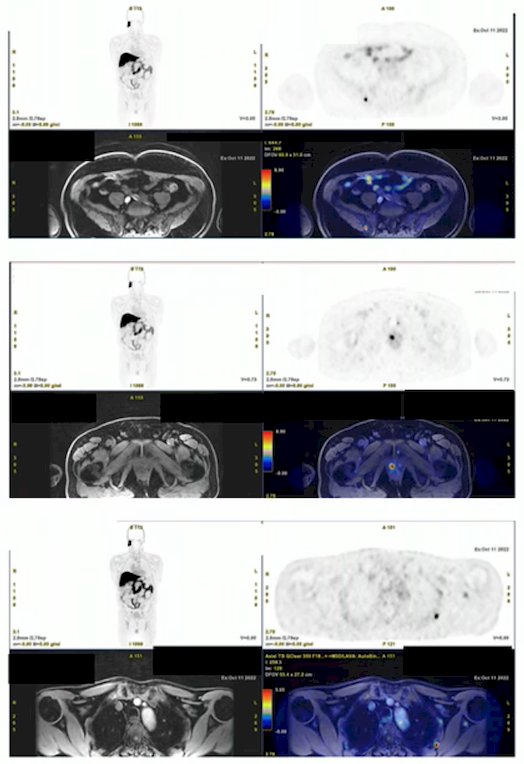
Dr. Giorgio Gandaglia started with a case presentation of a 68 year old man with no family history of prostate cancer, BMI 24 kg/m2, a prior left laparoscopic hemicolectomy, PSA 17.2 ng/mL, and digital rectal examination demonstrating cT2c disease. A multiparametric MRI showed an 8mm PI-RADS 4 lesion at the left base, and + MRI-targeted biopsy (4 cores) + concomitant systematic biopsy (12 cores) showed Grade Group 3 adenocarcinoma of the prostate in all cores. Staging with a bone scan showed pathological uptake in two right ribs and CT scan showed no enlarged lymph nodes. Subsequently, he underwent an 18F-PSMA PET/CT and PET/MRI that showed PSMA-avid lesions in bilateral prostate lobes, posterior portion of the second left rib, left scapula, sternum, right iliac wing, and left pubic bone:
Radiotherapy to the Primary + ADT Alone
The position of radiotherapy to the primary + ADT alone was taken by Dr. Nicolas Mottet who emphasized that this patient has no lesions outside the axial skeleton and no visceral metastases. Furthermore, quite simply he only has two bone metastases on conventional imaging, which is low volume per Dr. Sweeney’s criteria.
Dr. Mottet then discussed STAMPEDE Arm H,1 an open label, randomized controlled phase III trial of 2,061 men (819 low volume) that randomized patients with de novo mHSPC in a 1:1 fashion to standard of care + radiotherapy or standard of care alone. Standard of care was defined as lifelong ADT with upfront docetaxel permitted from December 2015 onwards. Men allocated to radiotherapy received either a daily (55 Gy in 20 fractions over 4 weeks) or weekly (36 Gy in six fractions over 6 weeks) schedule that was nominated before randomization. Median follow up was 37 months, median patient age was 68.0 years, and median PSA was 97 ng/ml. There were 18% of patients that received early docetaxel. In the overall cohort, radiotherapy improved failure-free survival (HR 0.76, 95% CI 0.68 to 0.84) but not overall survival (HR 0.92, 95% CI 0.80 to 1.06) in the overall cohort. However, when stratified by metastatic burden, OS benefits were seen in the low volume group (HR 0.68, 95% CI 0.52 to 0.90) with restricted mean survival time improved by 3.6 months from 45.4 to 49.1.
Updated results of STAMPEDE Arm H were published in 2022.2 With a median follow up of 61.3 months, prostate radiotherapy continued to demonstrate overall survival benefit in patients with low metastatic burden (HR: 0.64, 95% CI: 0.52 - 0.79, p < 0.001):
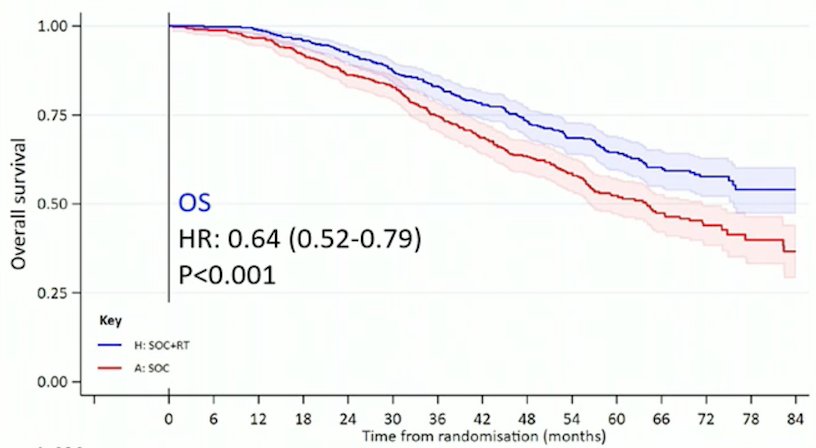
whereas no benefit was seen in patients with a high metastatic burden (HR: 1.11, 95% CI: 0.96 - 1.28, p = 0.164; interaction p = 0.001). No evidence of difference in time to symptomatic local events was found, and there was no evidence of difference in Global QoL or QLQ-30 Summary Score.
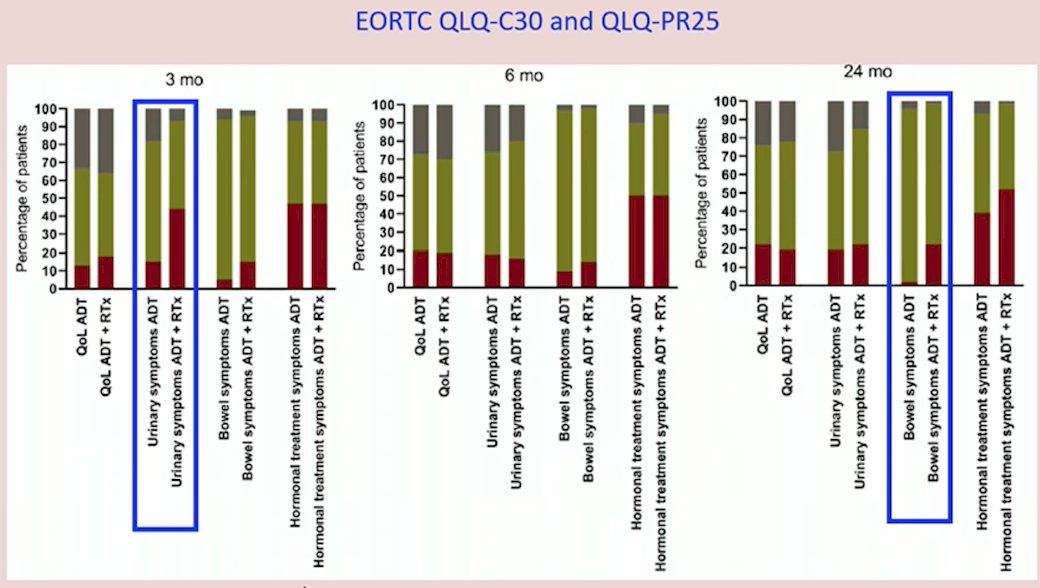
Dr. Mottet notes that if the patient receives prostate radiotherapy, the rationale is to improve outcomes (ie. survival) and to lower the risk of local progression and side effects. This would mean no/minimal local side effects and thus a clear benefit. However, patient reported outcome data from the HORRAD trial3 suggests that radiotherapy to the primary is not trivial. Patients reported significantly more diarrhea (difference between the groups 10.8; 95% CI 7.3-14.2), bowel symptoms (4.5; 95% CI 2.1-6.8), and urinary symptoms (11.9; 95% CI 8.9-14.8) after external beam radiotherapy + ADT compared with ADT alone (all between-arm difference p < 0.001). Urinary complaints were comparable between the two groups at 6 months, however at 2 years, only bowel symptom scores were significantly different (8.0; 95% CI 4.8-11.1, p ≤ 0.001):
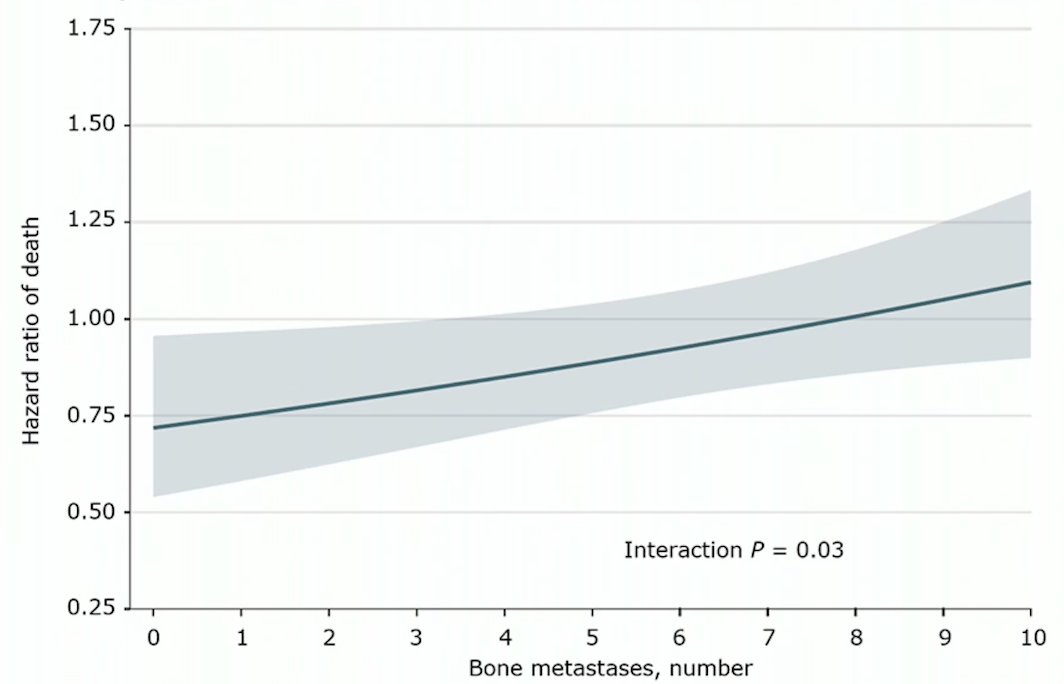
In a secondary analysis of STAMPEDE Arm H,4 Dr. Mottet notes that number of metastases matters to who derives a benefit from prostate radiotherapy. Survival benefit decreased continuously as the number of bone metastases increased, with benefit most pronounced at up to 3 bone metastases. The magnitude of benefit from the addition of prostate radiotherapy was greater in patients with low metastatic burden with only nonregional lymph nodes (M1a) or 3 or fewer bone metastases without visceral metastasis (HR for overall survival: 0.62; 95% CI: 0.46 - 0.83; HR for failure-free survival: 0.57; 95% CI: 0.47 - 0.70) than among patients with 4 or more bone metastases or any visceral/other metastasis (HR for overall survival: 1.08; 95% CI: 0.91 - 1.28; interaction p= 0.003; HR for failure-free survival: 0.87; 95% CI: 0.76 - 0.99).
Dr. Mottet concluded his part of the debate by emphasizing again that this patient has low volume disease and that standard of care is ADT + external beam radiotherapy to the primary.
Radiotherapy to the Primary + ADT + ARPI
The position of radiotherapy to the primary + ADT + ARPI was taken by Dr. Gerhardt Attard. Dr. Attard started his portion of the debate, similarly to Dr. Mottet, highlighting the benefit of ADT + radiotherapy to the primary in low volume M1 based on the extended follow-up reported for Arm H of STAMPEDE.2 In his opinion, PSMA PET is blurring the distinction between very high-risk localized and M1 volume disease. Dr. Attard also emphasized the secondary analysis of Arm H4 in that the benefit from adding radiotherapy to ADT does not stop with detection of any metastases on bone scan but tapers off with increasing metastatic volume:
In addition to imaging, molecular studies also suggest that disease volume is a continuum, with molecular signatures showing progressive changes across disease states. Notably, in STAMPEDE, based on molecular signatures, there is no significant differences between N1M0 and M1 low volume disease:5

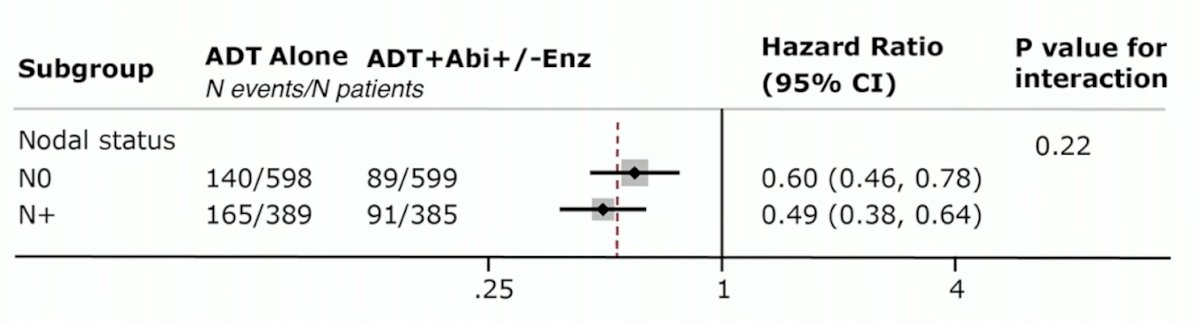
In the STAMPEDE arm of high-risk localized prostate cancer treated with either abiraterone or enzalutamide, there was a consistent effect with ARPI regardless of metastatic burden.6 Local radiotherapy (74 Gy in 37 fractions to the prostate and seminal vesicles or the equivalent using hypofractionated schedules) was mandated for node negative and encouraged for node positive disease. There were 1,974 patients randomized and over a median follow-up of 72 months (IQR 60–84), metastasis-free survival was significantly longer in the combination-therapy groups (median not reached, IQR NE–NE) than in the control groups (not reached, 97–NE; HR 0.53, 95% CI 0.44–0.64). Overall survival (median not reached [IQR NE–NE] in the combination-therapy groups vs not reached [103–NE] in the control groups; HR 0.60, 95% CI 0.48–0.73):

Additionally, the abiraterone effect was consistent with increasing node burden:
Finally, Dr. Attard highlighted that ADT + radiotherapy could be synergistic, given that ADT inhibits upregulation of Ku70 after radiotherapy. The implications of this are that more effective AR inhibition (ADT + ARPI) may increase radiotherapy effect, and may improve local control, especially in men with T3b/T4 disease. Abiraterone costs < 11 pounds/day and is cost-dominate in high-risk localized disease, such that generic drugs reduce barriers to combination with radiotherapy + ADT.
Dr. Attard concluded his portion of the debate with the following statements:
- There is no level 1 evidence for ADT + radiotherapy + ARPI
- But definite level 1 evidence may not be forthcoming (PEACE-1 is awaited)
- Thus, clinically pragmatic decisions will be required:
- Well tolerated and no overlapping toxicity
- Distinct and potentially synergistic mechanisms of action
- No biologic rationale to suggest that the benefit of adding abiraterone to ADT + radiotherapy stops on detection of bone metastases on Technetium scans
Case presented by: Giorgio Gandaglia, MD, IRCCS Ospedale San Raffaele, Milan, Italy
Debater 1: Nicolas Mottet, MD, PhD, University Hospital, Saint-Etienne, France
Debater 2: Gerhardt Attard, MD, PhD, University College London Cancer Institute, London, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2023 European Association of Urology (EAU) Annual Meeting, Milan, IT, Fri, Mar 10 – Mon, Mar 13, 2023.
References:
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomized controlled phase 3 trial. Lancet 2018 Dec 1;392(10162):2353-2366.
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the prostate for men with metastatic prostate cancer in the UK and Switzerland: Long-term results from the STAMPEDE randomised controlled trial. PLoS Medicine. 2022;19(6):e1003998.
- Boeve L, Hulshof MCCM, Verhagen PCMS, et al. Patient-reported quality of life in patients with primary metastatic prostate cancer treated with androgen deprivation therapy with and without concurrent radiation therapy to the prostate in a prospective randomized clinical trial: Data from the HORRAD trial. Eur Urol. 2021 Feb;79(2):188-197.
- Ali A, Hoyle A, Haran AM, et al. Association of Bone Metastatic Burden With Survival Benefit From Prostate Radiotherapy in Patients With Newly Diagnosed Metastatic Prostate Cancer: A Secondary Analysis of a Randomized Clinical Trial. JAMA Oncol. 2021;7(4):555-563.
- Grist E, Friedrich S, Brawley C, et al. Accumulation of copy number alterations and clinical progression across advanced prostate cancer. Genome Med. 2022 Sep 5;14(1):102.
- Attard G, Murphy L, Clarke NW, et al. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: A meta-analysis of primary results from two randomized controlled phase 3 trials of the STAMPEDE platform protocol. Lancet 2022 Jan 29;399(10323):447-460.