(UroToday.com) The 2023 EAU annual meeting included a session on clinically meaningful questions in the management of advanced, hormone-sensitive prostate cancer, featuring a state-of-the-art presentation by Dr. Piet Ost discussing which patients with low-volume hormone-sensitive prostate cancer should use metastases directed therapy. Dr. Ost started his presentation emphasizing that in the synchronous mHSPC disease space, data from STAMPEDE Arm H guides who will benefit from radiotherapy to the primary (only low volume patients).1
Low burden is defined as: patients with only non-regional lymph nodes or 3 or fewer bone metastases with or without non-regional lymph nodes, regardless of axial or extra axial location and without any visceral/other metastases. With regards to metastasis-directed therapy in de novo M1 HSPC, there is currently no high quality evidence.
For metachronous mHSPC, there is prospective data on metastasis-directed therapy, with a typical trial design in this space as follows:

When considering metastasis directed therapy, Dr. Ost notes that it is important to have good quality imaging, thus a prominent role for PSMA PET/CT. In the ORIOLE trial, all patients received conventional imaging and PSMA PET/CT and physicians were blinded to the PSMA result.2 In the following Kaplan-Meier curve for distant metastasis free survival, it is clear that no untreated lesions had significantly improved outcomes compared to any untreated lesions (HR 0.19, p = 0.0002):

Dr. Ost notes that published pooled data from the two metastasis directed therapy trials (STOMP and ORIOLE) demonstrates that metastasis-directed therapy in these patients improves progression-free survival from 5.9 months (95% CI: 3.2 – 7.1) to 11.9 months (95% CI: 8.0 – 18.3; HR: 0.44, p < 0.001), however without any significant improvements seen in radiographic progression-free survival, time to castration-resistant disease, or overall survival.3
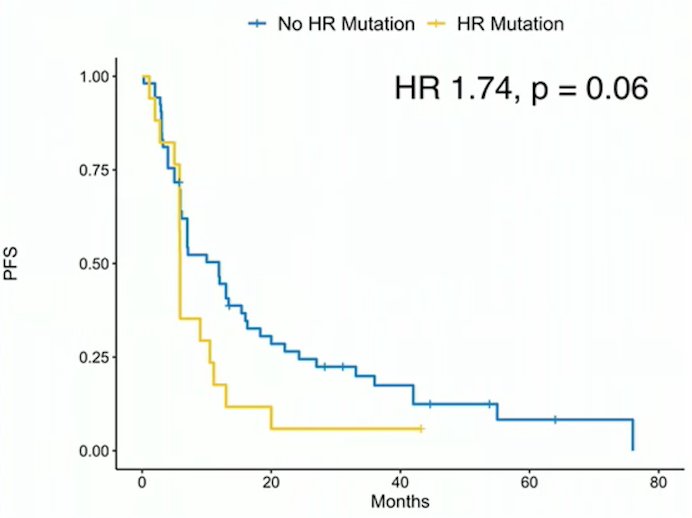
 Dr. Ost also highlighted that HR mutatation status is important when discussing metastasis directed therapy with patients. In the combination analysis of STOMP and ORIOLE, almost all patients with a high risk mutation relapsed within 2 years, with the hypothesis being that such patients should proceed straight to systemic therapy:3
Dr. Ost also highlighted that HR mutatation status is important when discussing metastasis directed therapy with patients. In the combination analysis of STOMP and ORIOLE, almost all patients with a high risk mutation relapsed within 2 years, with the hypothesis being that such patients should proceed straight to systemic therapy:3
With regards to metastasis directed therapy + ADT versus ADT alone, Dr. Ost highlighted the EXTEND trial, whereby men with <= 5 metastases were randomized to metastasis directed therapy + 6 months of ADT versus 6 months of ADT alone. The primary endpoint for this trial is progression free survival (biochemical, clinical, radiographic progression or death) with the following trial design:

Over a median follow-up of 22.1 months, the median PFS for the combined therapy arm was not reached and was 15.8 months for the ADT only arm (HR 0.25, 95% CI 0.12-0.55):

Dr. Ost concluded his presentation discussing which patients with low-volume hormone-sensitive prostate cancer should use metastases directed therapy with the following take-home messages:
- Metastasis directed therapy improves PFS as compared to observation
- Metastasis directed therapy + temporary ADT improves PFS as compared to ADT alone
- Use of the most sensitive imaging is crucial (ie. PSMA PET/CT)
- The duration of response depends on the presence of high risk mutations
Presented by: Piet Ost, Iridium Network, Antwerp, Belgium
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2023 European Association of Urology (EAU) Annual Meeting, Milan, IT, Fri, Mar 10 – Mon, Mar 13, 2023.
References:
- Parker CC, James ND, Brawley CD, et al. Radiotherapy to the primary tumour for newly diagnosed, metastatic prostate cancer (STAMPEDE): A randomized controlled phase 3 trial. Lancet 2018 Dec 1;392(10162):2353-2366.
- Phillips R, Shi WY, Deek M, et al. Outcomes of Observation vs Stereotactic Ablative Radiation for Oligometastatic Prostate Cancer: The ORIOLE Phase 2 Randomized Clinical Trial. JAMA Oncol 2020 Mar 26;6(5):650-659.
- Deek MP, Van der Eecken K, Sutera P, et al. Long-term outcomes and genetic predictors of response to metastasis-directed therapy versus observation in oligometastatic prostate cancer: Analysis of STOMP and ORIOLE trials. J Clin Oncol. 2022;40(29):3377-3382.