(UroToday.com) The 2023 European Association of Urology (EAU) annual congress held in Milan, Italy between March 10th and 13th, 2023 was host to an EAU Section of Oncologic Urology (ESOU) session addressing progress and controversies in urologic oncology. In this case-based debate moderated by Dr. Michael Baboudjian, Professor Andrea Necchi was tasked with arguing in favor of a combined neoadjuvant and adjuvant systemic therapy approach in patients with high-risk muscle-invasive bladder cancer (MIBC).
Dr. Baboudjian began with the following case presentation:
- 59-year-old woman with a performance status of 0 presents with gross hematuria.
- Her past medical history is notable for a history of tobacco smoking
- Urinary cytology positive for high-grade urothelial carcinoma
- A flexible cystoscopy demonstrates a 4 cm lesion at the left bladder wall and another 1 cm lesion at the trigone
- She undergoes a TURBT with photodynamic diagnosis with a complete resection, which demonstrates HG T2 MIBC without CIS
- She has normal renal function with an eGFR of 92 ml/min
- Staging work-up with a CT + bone scan demonstrates cN0cM0 disease with no UTUC present and no hydronephrosis
- The patient’s case is discussed within a multi-disciplinary care team:
- Standard option: radical cystectomy with urinary diversion
- Other option: trimodality therapy (TMT): TURBT + chemotherapy + radiotherapy
- Third option: Enrollment in RECHIVE trial (NCT01093066: a phase 2 trial that includes 6 cycles of MVAC administered every 2 weeks + TURBT)
- The patient enrolls in the RECHIVE trials
- Good compliance but experiences grade 4 cisplatin-related ototoxicity
- Re-TUR post-MVAC: persistent T2 tumor
- Undergoes subsequent RC + urinary diversion with a Miami pouch
- Final pathology: ypT2bN1R0
- Undergoes surveillance with subsequent development of retroperitoneal recurrence with duodenal invasion
- Receives 4 cycles of gemcitabine + carboplatin
- Well-tolerated by experiences grade 3 thrombocytopenia
- CT and PET-CT scan: stable
- Starts avelumab maintenance, as pet the JAVELIN-100 trial
- In February 2023, experiences progression with a hepatic lesion: still alive and treated with enfortumab vedotin
At this point, the discussion was turned over to Dr. Necchi to debate in favor of a combined neoadjuvant/adjuvant approach to the treatment of high-risk MIBC patients.
Dr. Necchi began by highlighting that perioperative therapies are gaining momentum in the MIBC space. Currently, the EAU, ESMO, and NCCN guidelines all acknowledge the use of neoadjuvant and/or adjuvant approaches (recommendation strength varying from weak to strong) for MIBC patients.
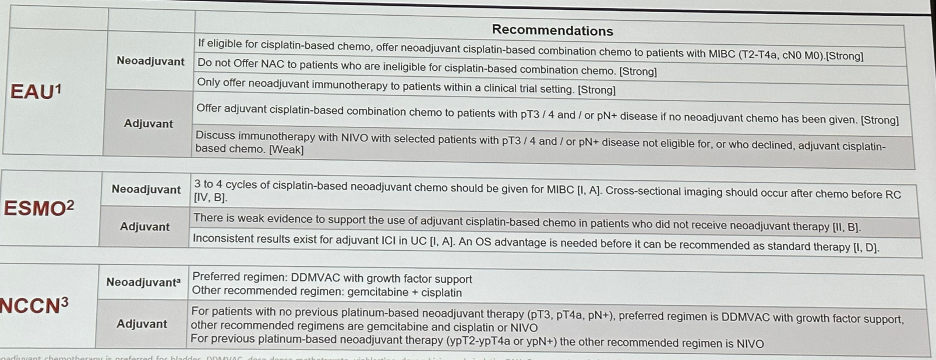
While guidelines have acknowledged the use of neoadjuvant and/or adjuvant systemic therapies, key questions remain unanswered in perioperative MIBC:
- Which is better: the neoadjuvant or adjuvant approach?
- Is dd-MVAC or GC the preferred neoadjuvant approach
- What is the optimal duration/intensity of treatment?
- Does adjuvant radiation play a role?
- There is a lack of reliable biomarkers: who needs/benefits from systemic therapy?
- What is the role of newer agents beyond checkpoint inhibitors?
With regards to the optimal neoadjuvant chemotherapy regimen, the recently published GETUG/AFU VESPER V05 phase III trial randomized 500 patients to either six cycles of dd-MVAC once every 2 weeks or four cycles of gem/cis once every 3 weeks before surgery (neoadjuvant group: ~90% of total cohort) or after surgery (adjuvant group: ~10% of total cohort).
60% of patients received the planned six cycles in the dd-MVAC arm and 84% received four cycles in the GC arm, and thereafter, 91% and 90% of patients underwent surgery, respectively. Organ-confined response (< ypT3N0) was observed more frequently in the dd-MVAC arm (77% v 63%, P = .001). 3-year PFS was improved in the dd-MVAC arm, but the study did not meet its primary end point (3-year rate: 64% v 56%, hazard ratio [HR] = 0.77 [95% CI, 0.57 to 1.02], P = .066); nevertheless, the dd-MVAC arm was associated with a significantly longer time to progression (66% versus 56%; HR: 0.70, 95% CI: 0.51 to 0.96, p=0.025). Overall survival outcomes to date have favored dd-MVAC (HR: 0.66, 95% CI: 0.47 to 0.92), albeit without statistical significance and with data not yet fully mature for this outcome.1

What about the adjuvant space? Updated disease-free survival (DFS) outcomes from the CheckMate-274 trial of adjuvant nivolumab, with a median follow-up of 36 months, has demonstrated a DFS benefit for nivolumab versus placebo in both the IRR and PD-L1 ≥1% groups, as well as in most pre-specified clinical subgroups.

Significantly, a pronounced DFS benefit was maintained in the subcohort of patients who had received prior neoadjuvant cisplatin (HR: 0.54, 95% CI: 0.40-0.72), which argues in favor of a combined neoadjuvant/adjuvant approach for such HR MIBC patients.
There are currently several ongoing phase 3 trials with perioperative immunotherapy, particularly in the cisplatin ineligible disease space. Drawing parallels from the advanced melanoma disease space, will we see a similar approach extrapolated pan cancer-wide?
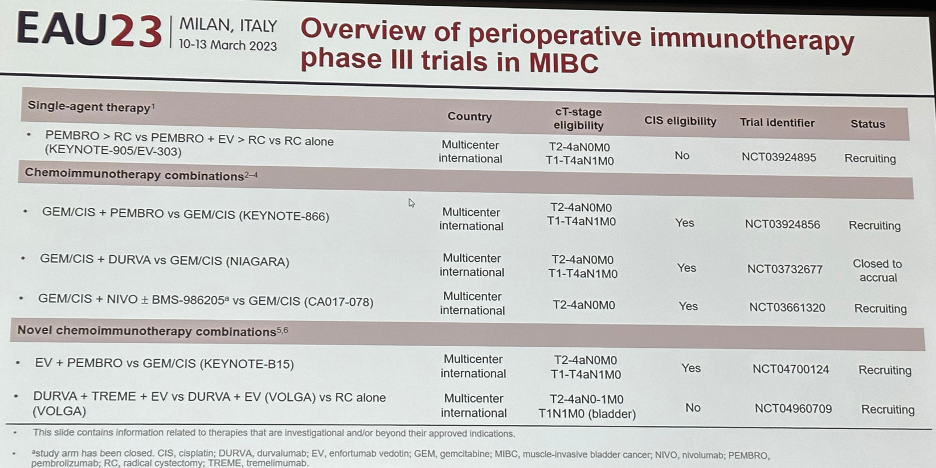
Dr. Necchi highlighted the KEYNOTE-905/EV-303 (NCT03924895) study design that will randomize treatment naïve, cisplatin ineligible or refusing MIBC patients with cT2-4aN0M0 or cT1-4aN1M0 to one of three arms:
- Arm A: Pembrolizumab 200 mg IV q3w x 3 cycles
- Arm B: Observation
- Arm C: Pembrolizumab x3 cycles + enfortumab vedotin (1.25 mg/kg IV Q3 weeks x 3 cycles)
Patients will subsequently undergo a RC +PLND and continue perioperatively/adjuvantly on the same treatment to which they were randomized to preoperatively. The primary endpoint is event-free survival in arm C versus arm B.

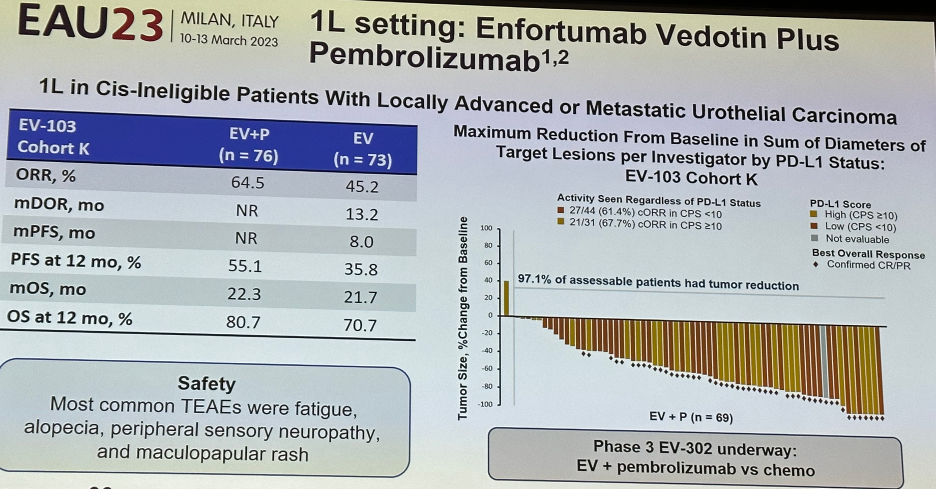
The rationale for the combination approach of pembrolizumab + enfortumab vedotin comes from results of the EV-10 cohort K assessing the efficacy of enfortumab vedotin monotherapy or in combination with pembrolizumab in previously untreated cisplatin-ineligible patients with locally advanced or metastatic urothelial cancer. Patients in this trial were randomized 1:1 to EV (1.25 mg/kg) as monotherapy on Days 1 and 8 or in combination with pembrolizumab (200 mg) on Day 1 of 3-week cycles (EV-103, NCT03288545). The primary endpoint of this study was confirmed objective response rate (ORR) per RECIST v1.1 by BICR.149 patients were enrolled. The confirmed ORR was 64.5% (95%CI 52.7 to 75.1) among patients treated with the combination of EV and pembrolizumab, with a median DOR not reached. Among those treated with EV monotherapy, the confirmed ORR was 45.2% (95% CI 33.5 TO 57.3) and median DOR was 13.2 months (95% CI 6.1 to 16.0).
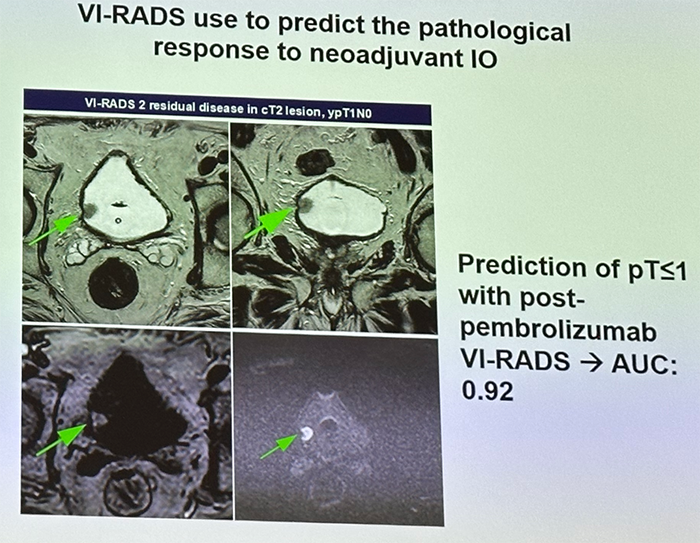
Tumor biomarkers and imaging tools are going to be critical for the appropriate selection of patients for sequential therapies. There is evidence that shifting molecular subtypes (basal, luminal, scar-like, and immune) may have differential responses to different perioperative systemic regimens.

Furthermore, use of MRI with the VI-RADS score may be used to predict the pathologic response to neoadjuvant IO therapy as demonstrated below:
Finally, with regards to the safety/AE profile, what is the safer approach: neoadjuvant or adjuvant systemic therapy? Monitoring the safety of perioperative novel therapies is of utmost importance in a potentially curative setting like in MIBC. Current tools that are used to qualify and grade treatment-related AEs may not necessarily fit the peculiar needs of perioperative therapies. From a practical standpoint, there are too many unanswered questions with regards to defining a safety event:
- What is the maximum acceptable wait time between end of neoadjuvant therapy and RC?
- What is the maximum acceptable wait time RC and start of adjuvant therapy?
- Should we count any logistical issues preventing therapy administration as safety events?
- What is the acceptable threshold of grade 3-5 treatment related AEs within a trial?
Dr. Necchi concluded as follows:
- Safety remains a concern requiring continuous patient and physician education. The safety/efficacy threshold remains uncertain in the perioperative setting.
- Different neoadjuvant therapy options could be used but their optimal positioning with regards to RC and adjuvant therapy remain uncertain
- Most people are still far behind the forefront of such tremendous achievements
- Shared decision-making still enables patients to engage and find the right treatment for them
- Never forget the importance of offering patients enrolment in clinical trials
Presented by: Professor Andrea Necchi, MD, Director of GU Medical Oncology, San Raffaele Hospital and Scientific Institute, Milan, Italy
Written by: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 European Association of Urology (EAU) Annual Meeting, Milan, IT, Fri, Mar 10 – Mon, Mar 13, 2023.
References: