The reason this is so important is that while the incidence of TCa is on the risk, as survival exceeds 99%, more and more surviving TCa patients are around. For a 30-year old man, that means 45-50 year additional life-expectancy – routine surveillance is not practical.
The basics of follow-up for TCa is below:
First 5 years following primary diagnosis and treatment:
- The goal is early detection of relapse – the first 2-3 years are the highest risk period
- Also, aim to minimize treatment and diagnostic scan intensity for cure
- The primary goal is detection and treatment of late toxicities – as the risk of recurrence is so low
To address this, there has been increased emphasis on risk-adapted planning of follow-up. In order to understand the rationale, have to answer the following questions:
- How often does relapse occur?
- When does relapse occur?
- Where does relapse occur?
In the early experience with AS and long-term follow-up, and before we understood the long term implications of repeated scanning, routine imaging was recommended. The 2008 NCCN surveillance for stage 1 NSGCT men included 13-16 CT scan in the first 5 years. Mettler FA et al. (Radiology 2008) noted that a single CT Chest is worth 400 chest x-rays; even a low-dose CT Chest is ~200. Repeated scans in this younger population are not benign. Another reason to cut down on scans and repeat visits is that adherence to guidelines is already relatively low. Yu et al. JCO 2009 noted that adherence to NCCN guidelines ranged between 7-72% for abdominal imaging, 13-49% for chest imaging, and 20-49% for tumor markers. Putting this all together, reducing the burden of follow-up protocols is important to improve adherence and reduce long-term morbidity.
Next, work by Kollmannsberger et al. (JCO 2015) demonstrates the time frame of recurrence. Risk of recurrence in men with NSGCT who are LVI negative (lower risk) is about 14% - of which 90% occur in the first 2 years. Only 1.8% occur after 2 years. In men who are LVI positive (high risk), the risk of recurrence is 44% - but still, the majority (95%) occur in the first 2 years, and only 1.9% occur after 2 years. Based on this, the greatest intensity of surveillance needs to be in the first 2-3 years (up to 3 years for seminoma).
To that end, the first consensus conference was in 2011 between EAU and ESMO – but they could not come to an agreement on the definition of follow-up groups. They did provide some broad recommendations, but no specifics.
They reconvened in 2016 and were able to reach an agreement. They grouped the patients into the following:
1. Seminoma stage 1: irrespective of treatment
2. NSGCT Stage 1 on AS
3. All other patients in complete remission after treatment
Patients with poor prognosis and/or active disease are excluded. They allowed for MRI instead of CT if needed – but need an experienced radiologist to read it. No chest x-ray for seminoma patients. Further reduced the number of visits.
The guidelines for the 3 categories are listed below: (and can be found only as the EAU/ESMO 2018 guidelines, Annals of Oncology 2018)
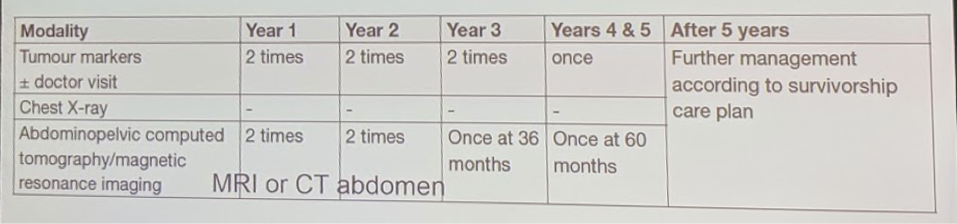
Seminoma on AS:
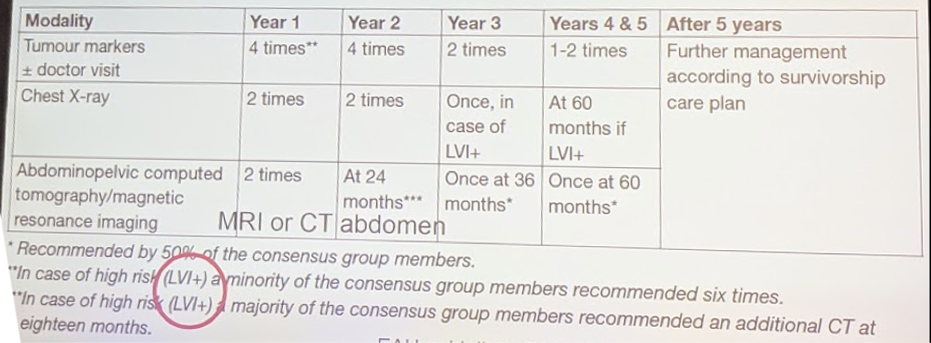
NSGCT on AS:
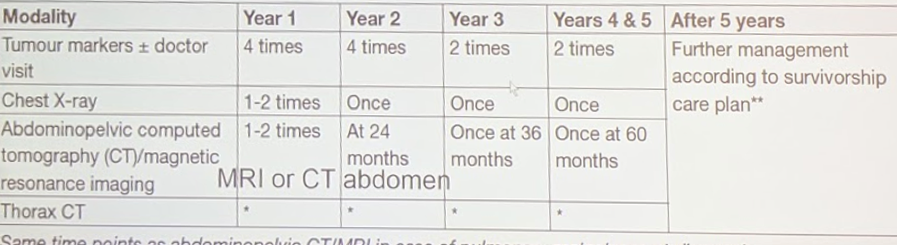
All other patients not in remission:
Lastly, after 5 years, all the guidelines indicate further management according to a survivorship care plan. This can vary from institution to institution and physician to physician. But it should entail clear instructions and guidance to primary care physicians that are likely to take over long-term surveillance and monitoring- with a focus on detecting and identifying long-term late toxicities. Aboussaly at al. (EU 2011) provide an example in their paper – and includes a handout to the patient.
Presented by: Richard Cathomas, PD Dr. med. Kantonsspital Graubünden, Chur, Switzerland
Written by: Thenappan Chandrasekar, MD (Clinical Instructor, Thomas Jefferson University) (twitter: @tchandra_uromd, @JEFFUrology) at the 34th European Association of Urology (EAU 2019) #EAU19, conference in Barcelona, Spain, March 15-19, 2019.