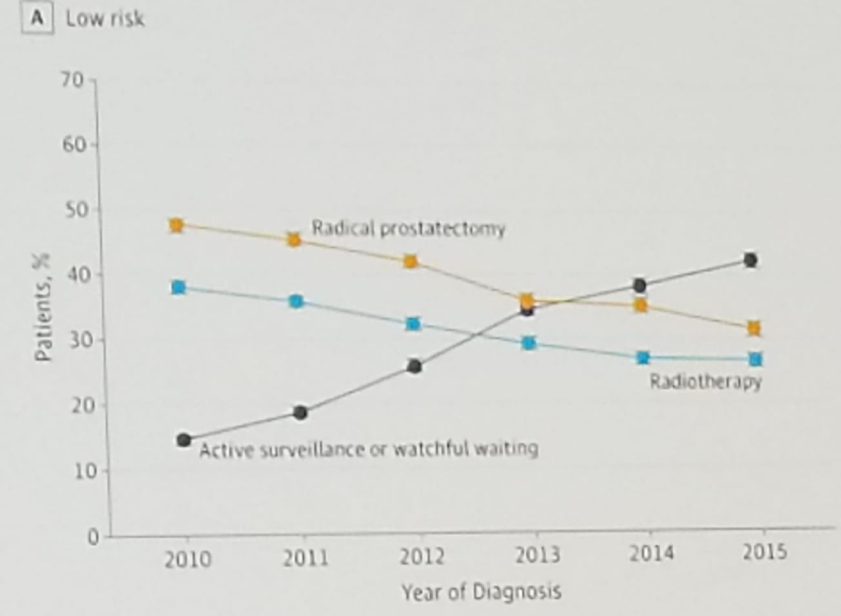
Figure 1 – The rising use of active surveillance in low-risk prostate cancer:
The use of multiparametric MRI (mpMRI) and mpMRI-informed targeted biopsies has improved the risk stratification. Importantly, the use of systematic biopsies in low-risk disease is still important, as combined with targeted biopsy it raises the percentage of patients with cancer upgrading.1 However, mpMRI is not always better, and data have shown that confirmatory targeted vs. systematic biopsy of active surveillance patients demonstrated upgrading to Gleason 7 in 25.9% vs. 26.1%, respectively.2 Currently, the risk stratification is changing, and targeted biopsy is more frequently used. It is important to remember that one core of a targeted biopsy showing Gleason 7 (3+4) does not equal one systematic biopsy core of Gleason 7 (3+4) disease. Dr. van den Bergh believes that new risk stratification is needed for inclusion of patients in active surveillance.
Another important point to remember when treating patients on active surveillance is the high drop-out rate. (3) We may need to have less strict follow-up criteria to make sure more patients stay on the active surveillance protocol. Dr. van den Bergh believes we need to move from fixed thresholds during follow-up to dynamic follow-up strategies.4
The next topic discussed was the new imaging modality that can be used in patients monitored with active surveillance. Local PSMA activity has been shown to be associated with Gleason score, and it may be possible to use it for active surveillance inclusion and follow-up.5
Incorporating genetics in active surveillance was another important topic discussed, and it is the next step in improving active surveillance. In a study assessing 1,211 patients on active surveillance, 26 patients were found to have BRCA 1&2, and ATM mutations. Patients who were reclassified with an upgrade of their Gleason score had a higher rate of BRCA 2 (4.1% vs. 0.7% for Gleason >=4+3, and 2.1% vs. 0.6% for Gleason 3+4).6
Concluding his presentation, Dr. van den Bergh stated that active surveillance is currently a standard option, and we need to incorporate it as a standard part of screening policies. It is important to focus on the timing of the treatment and not only on avoiding treatment. Lastly, the inclusion criteria for active surveillance should be widened, and targeted biopsy risk stratification should be used with a personalized approach.
Presented by: Roderick van den Bergh, University Medical Center Utrecht, Nieuwegein, the Netherlands
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at the 34th European Association of Urology (EAU 2019) #EAU19 conference in Barcelona, Spain, March 15-19, 2019.
References
1. Schoots et al. Is magnetic resonance imaging-targeted biopsy a useful addition to systematic confirmatory biopsy in men on active surveillance for low-risk prostate cancer? A systematic review and meta-analysis. BJU Int. 2018 Dec;122(6):946-958. doi: 10.1111/bju.14358. Epub 2018 Jun 6.
2. Klotz et al. Active Surveillance Magnetic Resonance Imaging Study (ASIST): Results of a Randomized Multicenter Prospective Trial. Eur Urol. 2019 Feb;75(2):300-309. doi: 10.1016/j.eururo.2018.06.025. Epub 2018 Jul 13.
3. Bokhorst et al. A Decade of Active Surveillance in the PRIAS Study: An Update and Evaluation of the Criteria Used to Recommend a Switch to Active Treatment. Eur Urol. 2016 Dec;70(6):954-960. doi: 10.1016/j.eururo.2016.06.007. Epub 2016 Jun 19.
4. Cooperberg et al. Eur Urol 2016
5. Ergul et al. Clin Nucl Med 2018
6. Carter et al. Germline Mutations in ATM and BRCA1/2 Are Associated with Grade Reclassification in Men on Active Surveillance for Prostate Cancer. Eur Urol. 2018 Oct 8. pii: S0302-2838(18)30684-5. doi: 10.1016/j.eururo.2018.09.021. [Epub ahead of print]
Urolog