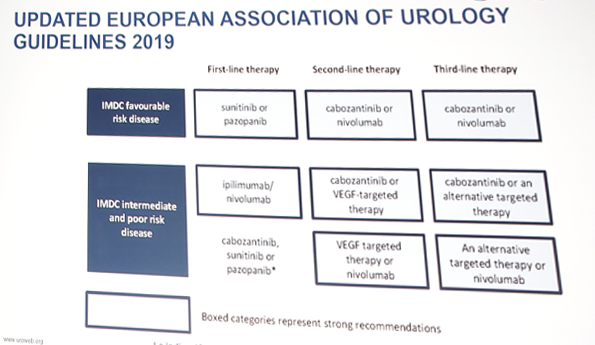
EAU guidelines
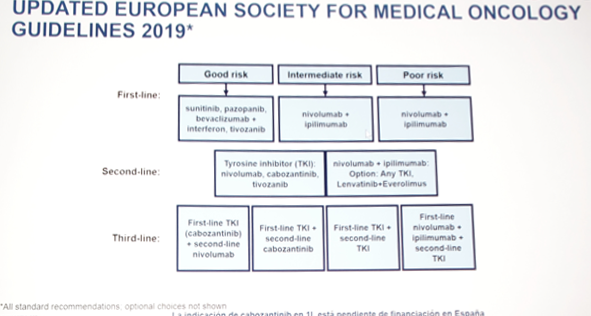
ESMO guidelines
Dr. Grimm then highlighted the new first line data, starting with CheckMate 214 trial 1. In this phase III trial, 1,096 patients were assigned to receive nivolumab plus ipilimumab (550 patients) or sunitinib (546 patients), including 425 and 422, respectively, that had intermediate or poor risk disease. At a median follow-up of 25.2 months in intermediate- and poor-risk patients, the 18-month overall survival rate was 75% with nivolumab plus ipilimumab and 60% with sunitinib. The median OS was not reached with nivolumab plus ipilimumab versus 26.0 months with sunitinib (HR for death 0.63; p <0.001). Furthermore, the objective response rate was 42% versus 27% (P<0.001), and the complete response rate was 9% versus 1%. The median PFS was 11.6 months (nivolumab + ipilimumab) and 8.4 months (sunitinib) (HR 0.82; p = 0.03, but significant per the prespecified 0.009 threshold). The recent update at GU ASCO 2019 (30 months of follow-up) showed durable responses in the good risk group (ORR nivolumab + ipilimumab 39% vs sunitinib 50%, p=0.14; PFS HR 1.23, 95%CI 0.90-1.65; OS HR 1.22, 95%CI 0.73-2.04).
Next, Dr. Grimm discussed the recently presented results (GU ASCO 2019) of the KEYNOTE-426 trial2.
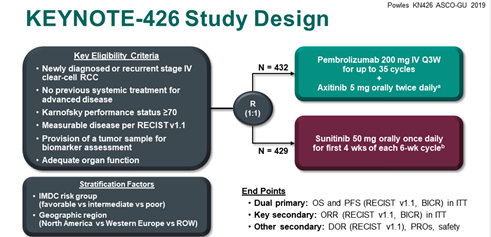
This trial was an international, multi-institutional open label phase III trial evaluating the efficacy and safety of pembrolizumab + axitinib versus sunitinib as first-line therapy. There were 432 patients with newly diagnosed or recurrent stage IV clear cell RCC and no previous systemic treatment that were randomized to pembrolizumab 200mg IV Q3 weeks plus axitinib 5mg PO BID and 429 patients randomized to sunitinib 50mg PO daily. At this first interim analysis, patients had a median follow up of 13 months. Pembrolizumab with axitinib significant improved OS (HR 0.53, 95%CI 0.38-0.74; 12-month rate 89.9% vs 78.3%), PFS (HR 0.69, 95%CI 0.57-0.84; median 15.1 vs 11.1 months), and ORR (59.3% vs 35.7%; p< 0.0001) compared to sunitinib. In subgroup analyses, outcome benefit was demonstrated in the pembrolizumab + axitinib cohort in all IMDC risk groups and PD-L1 expression positivity. Higher grade (3-5) adverse effects were seen in 63% of patients in the pembrolizumab + axitinib cohort compared to 58% in the sunitinib arm.
As follows are first line phase III trials with PD-1 immune checkpoint inhibitor vs sunitinib in advanced/mRCC:

CABOSUN was a randomized phase II multicenter trial evaluating cabozantinib compared with sunitinib as first-line therapy in patients with mRCC3. Patients had untreated clear cell mRCC and ECOG performance status of 0 to 2 and were intermediate or poor risk per IMDC criteria. There were 157 patients randomly assigned 1:1 to cabozantinib (60 mg once per day) or sunitinib (50 mg once per day; 4 weeks on, 2 weeks off), with PFS as the primary end point. Compared with sunitinib, cabozantinib treatment significantly increased median PFS (8.2 v 5.6 months) and was associated with a 34% reduction in rate of progression or death (aHR 0.66, 95%CI 0.46-0.95). ORR was 46% for cabozantinib versus 18% for sunitinib. All-causality grade 3 or 4 adverse events were 67% for cabozantinib and 68% for sunitinib.
Dr. Grimm concluded this section of his talk regarding first-line therapy by noting several points:
- Nivolumab + ipilimumab: intermediate and poor risk patients have a proven OS benefit, long-term remissions, favorable toxicity and moderate ORR with high complete response rates. PD-L1 positive patients benefit most.
- VEGFR-TKI + PD-L1/PD-1 Inhibition:
- Demonstrate a high ORR with a known toxicity profile
- Axitinib + pembrolizumab has an OS, PFS and ORR benefit in all risk groups
- Avelumab + axitinib have no proven OS benefit as of yet

In the second line setting, Dr. Grimm highlighted the phase III METEOR trial testing cabozantinib vs everolimus 4. This trial randomized 658 patients that had progressed on VEGFR-targeted therapy to cabozantinib (n=330) vs everolimus (n=328) with a median time to progression of 7.4 months with cabozantinib compared to 3.8 months with everolimus (HR 0.58, 95%CI 0.45-0.75). OS also favored cabozantinib over everolimus (HR 0.67, 95%CI 0.51-0.89).
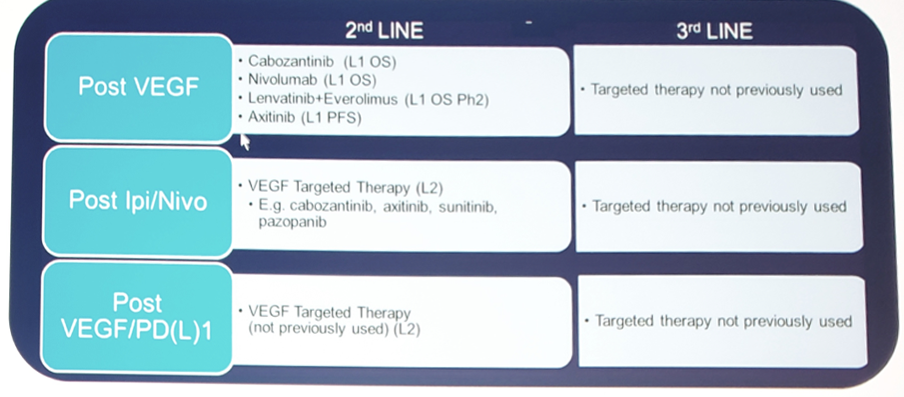
In 2019, we are finally developing some clarity as to the sequential treatment of mRCC:
Dr. Grimm concluded this high-level, comprehensive talk with several important take home messages:
- Management of advanced RCC has evolved with the approval of immune-checkpoint inhibitors (nivolumab) and new multikinase inhibitors (cabozantinib, lenvatinib, tivozanib)
- In the front-line setting: (i) CABOSUN demonstrated prolonged PFS of cabozantinib versus sunitinib in patients with intermediate/poor risk disease; (ii) CheckMate 214 demonstrated a significantly higher ORR and OS versus sunitinib in IMDC intermediate/poor risk patients; (iii) PD-1 immune checkpoint inhibitor + axitinib (KEYNOTE 426; JAVELIN 101) showed improved outcomes over sunitinib but are not yet approved
- Numerous combination therapies are being tested and are likely to change the treatment landscape for advanced RCC
- Identifying optimal treatment sequencing and tailoring treatment approach to individual patient characteristics is fundamental to maximize patient outcomes.
Written By: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University - Medical College of Georgia Twitter: @zklaassen_md at the 34th European Association of Urology (EAU 2019) #EAU19 conference in Barcelona, Spain, March 15-19, 2019.
References:
- Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carinoma. N Engl J Med 2018;378(14):1277-1290.
- KEYNOTE-426, ASCO GU 2019.
- Choueiri TK, Halabi S, Sanford BL, et al. Cabozantinib versus Sunitinib as initial targeted therapy for patients with metastatic renal cell carcinoma of poor or intermediate risk: The Alliance A031203 CABOSUN Trial. J Clin Oncol 2017;35(6):591-597.
- Choueiri TK, Escudier B, Powles T, et al. Cabozantinib versus Everolimus in Advanced Renal-Cell Carcinoma. N Engl J Med 2015;373(19):1814-1823.