According to the AUA/SUO Guideline on the diagnosis and treatment of NMIBC, a complete TURBT is critical in the management of NMIBC for accurate tumor type, staging, grading, and optimization of patient outcomes.1 The guidelines state that in a patient with NMIBC, a clinician should offer blue light cystoscopy at the time of TURBT, if available, to increase detection and decrease recurrence (Moderate recommendation, Grade B). Furthermore, in a patient with a history of NMIBC with normal cystoscopy and positive cytology, a clinician should consider a prostatic urethral biopsy and upper tract imaging, as well as enhanced cystoscopic techniques (blue light cystoscopy, when available), ureteroscopy, or random bladder biopsies (Expert Opinion).
Similarly, the EAU guidelines also make several pertinent recommendations2:
- Fluorescence-guided biopsy and resection are more sensitive than conventional procedures for the detection of malignant tumors, particularly CIS (LE: 2a)
- A meta-analysis reported that blue light cystoscopy arms increase the detection of tumor lesions across all risk groups and an absolute reduction of <10% in recurrence rates within 12 months (LE: 1a)
- In patients with a history of Ta LG/G1 tumors, fulguration of small papillary recurrences on an outpatient basis can reduce the therapeutic burden and can be an option (LE: 3)
- Use methods to improve tumor visualization (fluorescence cystoscopy, narrow band imaging) during TURBT if available (LE: weak)
Dr. Lotan was part of a phase III comparative, multi-center study assessing the safety of blue light flexible cystoscopy with hexaminolevulinate (HAL) in surveillance of bladder cancer patients.3 The patient flow diagram for this study is as follows:
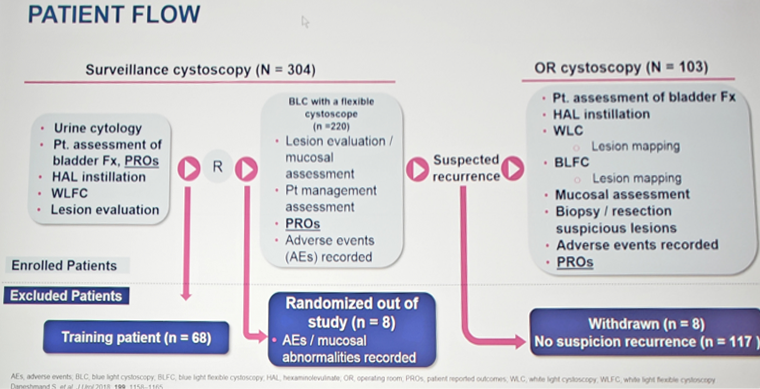
The primary end point of this study (n=304) was the proportion of patients with histologically confirmed malignancy detected only with blue light flexible cystoscopy. Following surveillance, 103 of the 304 patients were referred, including 63 with confirmed malignancy, of whom 26 had CIS. In 13 of the 63 patients (20.6%) recurrence was seen only with blue light flexible cystoscopy (p <0.0001); five cases were confirmed as CIS. Operating room examination confirmed CIS in 26 of 63 patients (41%), which was detected only with blue light cystoscopy in 9 of the 26 (34.6%, p <0.0001). Blue light cystoscopy identified additional malignant lesions in 29 of the 63 patients (46%). The false-positive rate was 9.1% for white and blue light cystoscopy. Additionally, patient-reported outcomes were collected for this study, including anxiety (PROMIS Anxiety 4a Short Form), pain (PROMIS Pain Intensity 1a), and perceived value (“Was it worth it” questionnaire; willingness to pay). There was an 86% response rate among the 304 patients included in the study with regards to the baseline survey, and 85% response rate for the post-surveillance survey. Overall, patients that underwent blue light surveillance and OR cystoscopy felt less fearful after the procedure than prior to the procedure, and 94% of patients felt that it was worthwhile4 Furthermore, 94.2% would do it again and 89.6% would recommend blue light cystoscopy to others. Since blue light cystoscopy may incur an out of pocket cost, when surveyed 50% of patients were willing to pay $100 or more for blue light cystoscopy.
A subsequent consensus panel had the following recommendations:
- A strong recommendation for the value of blue light cystoscopy at initial 3-month cystoscopy for AUA intermediate and high-risk patients
- Most recommended blue light cystoscopy at 3 and 6 months and then every 6 months for high-risk patients in the first two years
- Most recommended use prior to intravesical therapy if there is a concern for residual disease after TURBT
- Most recommended for use at the time of office and/or biopsy for low grade tumors
- Blue light cystoscopy may have a role in evaluating patients with positive cytology or equivocal lesions on white-light cystoscopy
Dr. Lotan concluded his talk with several key messages:
- Blue light cystoscopy improves the detection of patients with recurrent bladder cancer (20.6%)
- Blue light cystoscopy significantly improves the detection of patients with CIS (34.6%)
- Tumor detection was improved in 46% of patients who underwent repeat blue light cystoscopy
- Patients found the procedure worthwhile
- Several future needs include assessing whether low and intermediate risk patients will benefit from blue light cystoscopy, how often it should be performed, and analyzing cost-effectiveness models
Presented by: Yair Lotan, MD, The University of Texas Southwestern Medical Center, Dallas, Texas
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University - Medical College of Georgia Twitter: @zklaassen_md at the 34th European Association of Urology (EAU 2019) #EAU19 conference in Barcelona Spain, March 15-19, 2019.
References:
- Chang SS, Boorjian SA, Chou R, et al. Diagnosis and treatment of non-muscle invasive bladder cancer: AUA/SUO Guideline. J Urol 2016;196(4):1021-1029.
- Babjuk M, Bohle A, Burger M, et al. EAU Guidelines on Non-Muscle-Invasive Urothelial Carcinoma of the Bladder: Update 2016. Eur Urol 2017 Mar;71(3):447-461.
- Daneshmand S, Patel S, Lotan Y, et al. Efficacy and safety of blue light flexible cystoscopy with hexaminolevulinate in the surveillance of Bladder Cancer: A Phase III, Comparative, Multicenter Study. J Urol 2018 May;199(5):1158-1165.
- Smith AB, Daneshmand S, Patel S, et al. Patient-reported outcomes of blue-light flexible cystoscopy with hexaminolevulinate in the surveillance of bladder cancer: Results from a prospective multicentre study. BJU Int 2019 Jan;123(1):35-41.