At this point the patient was offered 3 treatment options:
- Radical cystectomy
- Bladder preservation with chemoradiation (Trimodal therapy)
- Active surveillance
Furthermore, the MRI has the additional value of functional sequences such as diffuse weighted imaging and dynamic contrast-enhanced imaging. Lastly, MRI also has the advantage of not harboring any associated radiation, like CT scans.
Two meta-analyses have shown that mpMRI has a pooled sensitivity of 87% and 92%, and a specificity of 79% and 87%, respectively, in distinguishing between muscle-invasive bladder cancer and non-muscle invasive bladder cancer1,2. MRI is impressively successful 95% of cases in differentiating muscle-invasive disease from non-muscle invasive disease3.
The VIRADS scoring system is a standardized approach to imaging and reporting mpMRI from bladder cancer, defining the risk of muscle-invasive disease. It was created through consensus using the existing literature. The scoring is applicable preferably to untreated patients before TURBT or at least 2 weeks after diagnostic TURBT or intravesical treatment. A 5-point VIRADS score is generated using the individual T2W, DWI, and DCE MRI categories and suggests the probability of muscle invasion, as seen in table 1, figure 1 and figure 2.
Dr. Panebianco concluded her talk stating that despite the tremendous improvement that has been achieved in bladder cancer, there are still certain issues that can be improved. These include:
- Better preoperative planning
- Local staging
- Improve the quality of TURBT resection and surgical confidence
- Consider incorporating the use of MRI before planning a re-TURBT
- Standardize the VIRADS scoring system and implement it on a regular basis to all patients
- Improve the response to therapy
Table 1 – VIRADS scoring system:
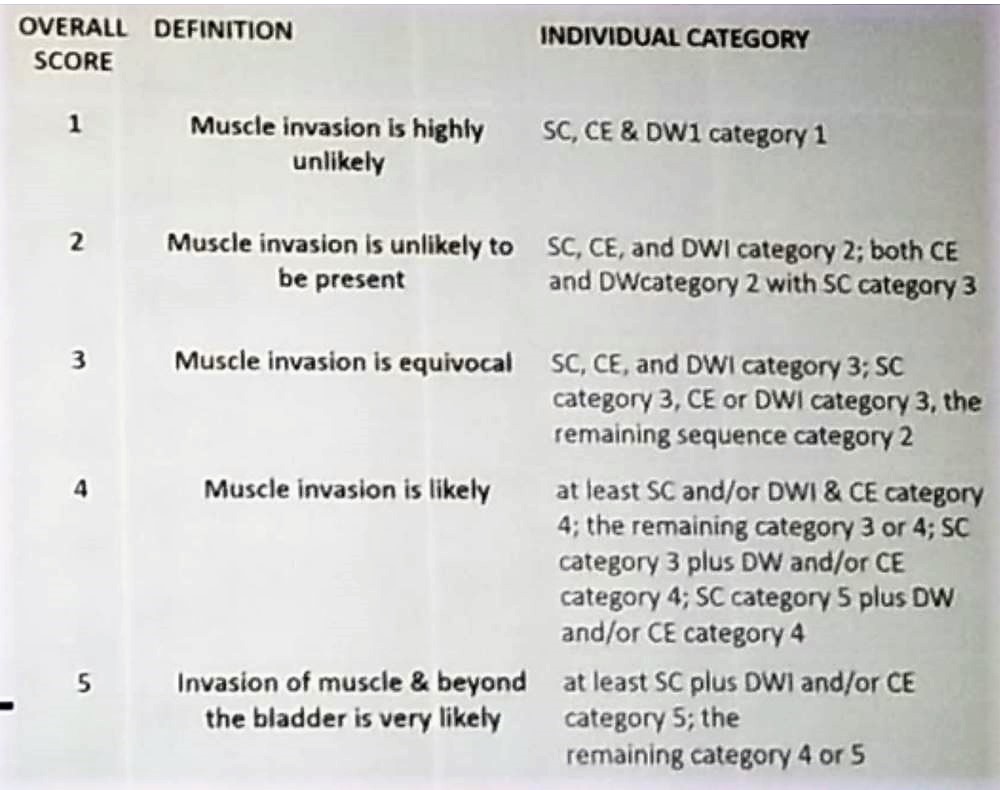
Figure 1 – VIRADS score 1,2,3:
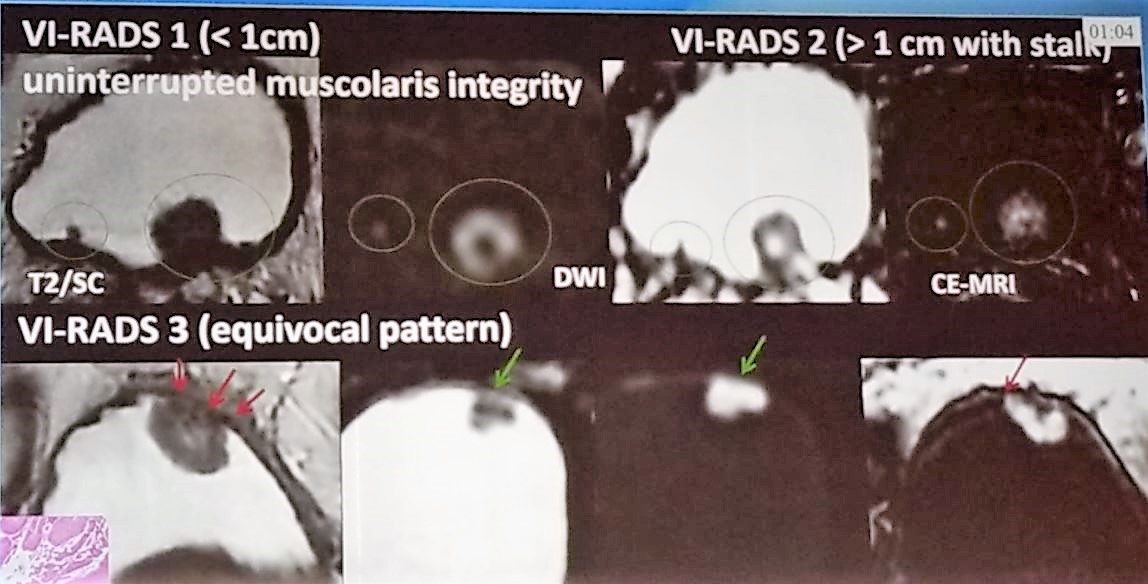
Figure 2 – VIRADS score 4 and 5:

References:
1. Gandhi N et al. (2018), Diagnostic accuracy of magnetic resonance imaging for tumour staging of bladder cancer: systematic review and meta‐analysis. BJU Int, 122: 744-753. doi:10.1111/bju.14366
2. Woo S. et al. Eur J Radiol 2017
3. Panebianco V et al. Eur Rad 2017
Presented by: Valeria Panebianco, Department of Radiology, University Sapienza, Rome, Italy
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at the 34th European Association of Urology (EAU 2019) #EAU19 conference in Barcelona, Spain, March 15-19, 2019
Further Related Content: What Can We Expect from Trimodal Therapy - Case-Based Debate No Evidence of Disease After Neoadjuvant Chemotherapy for MIBC: What Next?