(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to a trials-in-progress poster session. Dr. Surena Matin presented the study design of SURF303, a phase 2a/b trial evaluating dabogratinib (TYRA-300), a highly selective FGFR3 inhibitor, in patients with low-grade upper tract urothelial carcinoma (UTUC).
UTUC is a relatively rare malignancy, representing approximately 5–10% of all urothelial carcinomas,1,2 yet it is associated with diagnostic challenges, invasive disease potential, high recurrence rates, and treatment complexity.1-5 Low-grade UTUC is characterized by a high prevalence of FGFR3 alterations, reported in approximately 80% and up to 96% of tumors across studies.5-8
Current standard management for low-grade UTUC includes endoscopic tumor ablation with or without intraluminal chemotherapy or radical nephroureterectomy.1,2,5,9,10 Intracavitary therapy is technically challenging due to the unique anatomy of the upper urinary tract,11 is most effective in low-volume disease and often results in nephroureterectomy as the default curative option for patients with multifocal or high-volume tumors.12
A recent preoperative phase 1b study of pan-FGFR inhibition demonstrated the potential for FGFR3 inhibition in UTUC, enabling renal preservation in a subset of patients.5 However, currently available FGFR inhibitors lack FGFR3 isoform specificity and are associated with off-target toxicities resulting from inhibition of FGFR1/2/4, including nail disorders, stomatitis, hyperphosphatemia, central serous retinopathy, and other class-related adverse events.13
Dabogratinib is an oral, highly selective FGFR3 inhibitor designed to minimize off-target inhibition while maintaining activity against activating FGFR3 alterations.13 In the phase 1 portion of the SURF301 study in metastatic urothelial carcinoma, early clinical data demonstrated infrequent pan-FGFR-associated toxicities, including no hyperphosphatemia and no dose reductions or discontinuations at doses of 60 mg once daily or lower (n = 22; data cutoff August 15, 2024).14 Dabogratinib is currently being evaluated in the global phase 2a/b SURF303 study in patients with low-grade UTUC.15
Notably, in vitro analyses demonstrate marked FGFR isoform selectivity of dabogratinib. As shown in Table 1, the half-maximal inhibitory concentration (IC50) for FGFR3 is 11 nM, compared with 278 nM for FGFR1, 157 nM for FGFR2, and 405 nM for FGFR4, corresponding to approximately 25-fold selectivity for FGFR3 over FGFR1. By comparison, erdafitinib demonstrates less selectivity, with IC50 values of 2.6 nM for FGFR3 and 5.2 nM for FGFR1, corresponding to only approximately 2-fold selectivity.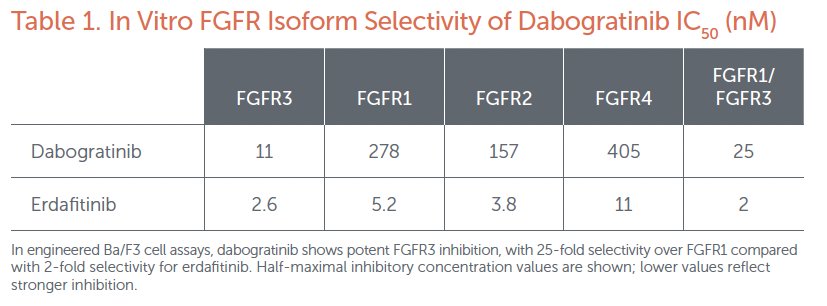
SURF303 (NCT07265947) is a phase 2a/b, multicenter, open-label, randomized study evaluating the efficacy and safety of oral dabogratinib administered once daily in adults with low-grade UTUC. Participants are enrolled in a biomarker-unselected population with retrospective assessment of FGFR3 alterations and are stratified according to aggregate baseline marker lesion size (<1.5 cm versus ≥1.5 cm).
Phase 2a employs a parallel randomized (1:1) design evaluating two dose cohorts:
• Cohort A: dabogratinib 60 mg once daily
• Cohort B: dabogratinib 80 mg once daily
An optional third cohort may be initiated if warranted based on emerging safety or efficacy data from the initial cohorts. Following dose optimization, phase 2b will enroll additional participants to further evaluate the efficacy, safety, pharmacokinetics, and therapeutic activity of dabogratinib at the selected dose.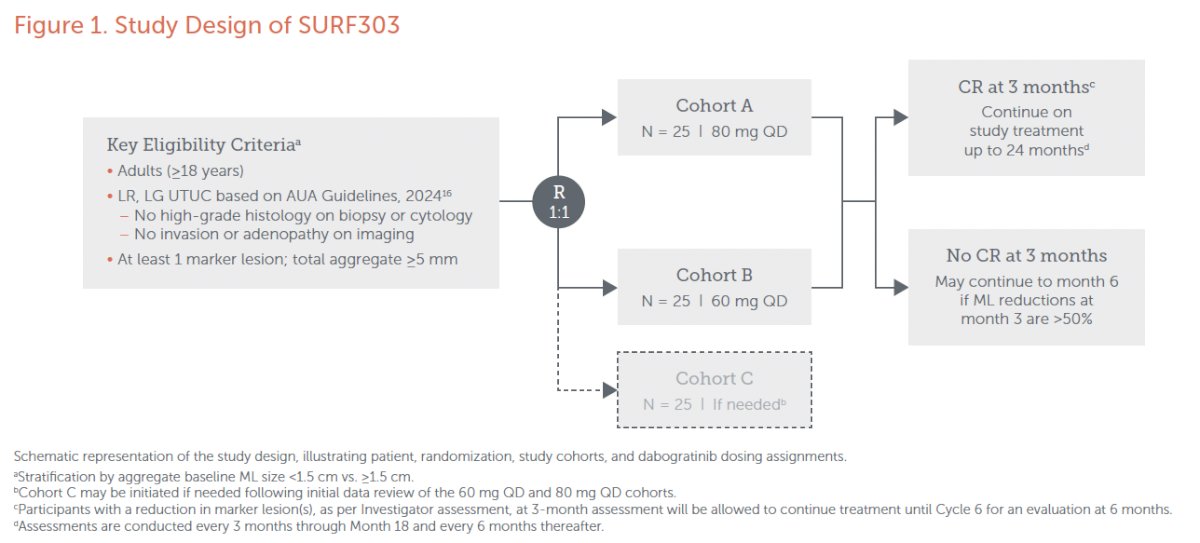
The study design is illustrated in the figure above. Eligible participants are randomized 1:1 to receive dabogratinib at either 60 mg or 80 mg once daily, with approximately 25 patients planned in each cohort. Participants must have at least one marker lesion with a total aggregate size ≥5 mm.
At the 3-month assessment, patients achieving a complete response continue study treatment for up to 24 months with scheduled evaluations every 3 months through month 18 and every 6 months thereafter. Participants without a complete response at 3 months may continue therapy to month 6 if marker lesion reductions exceed 50%.
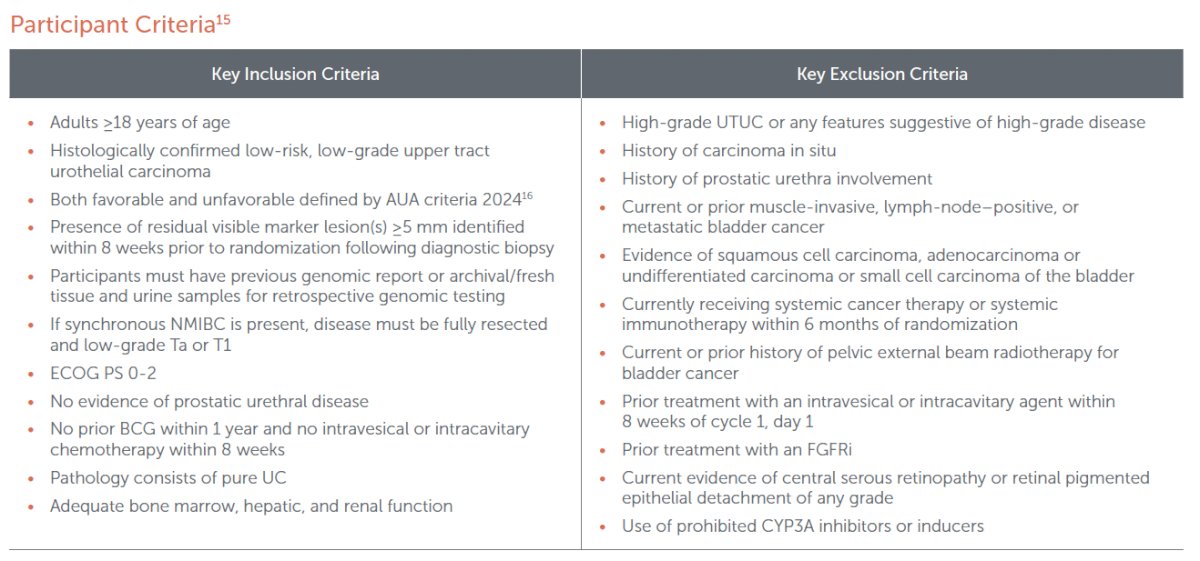
The key eligibility criteria are as follows:
- Histologically confirmed low-risk, low-grade UTUC
- Absence of high-grade UTUC or features suggestive of high-grade disease
- Absence of CIS
- Presence of residual visible marker lesion(s) ≥5 mm identified within 8 weeks prior to randomization following diagnostic biopsy
- Availability of genomic report or archival/fresh tissue and urine samples for retrospective genomic testing
- If synchronous NMIBC is present, the disease must be fully resected and low-grade Ta or T1
- No prior muscle-invasive, node-positive, or metastatic bladder cancer
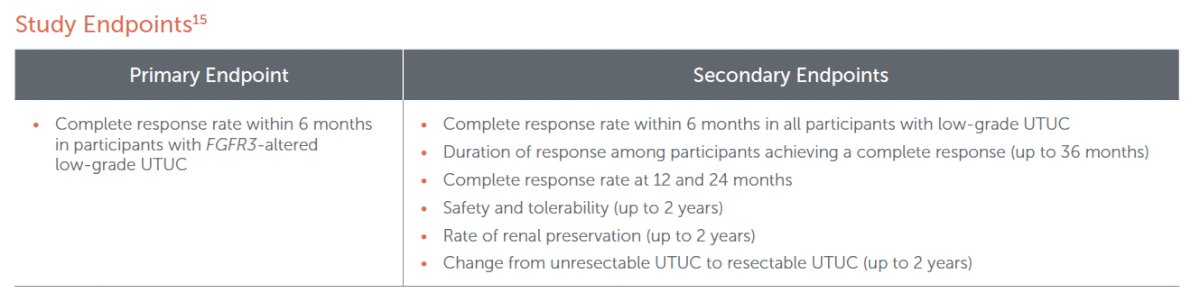
The primary study endpoint is the complete response rate within 6 months in participants with FGFR3-altered low-grade UTUC. Secondary endpoints include:
- Complete response rate within 6 months in all participants with low-grade UTUC
- Duration of response among participants achieving complete response (up to 36 months)
- Complete response rates at 12 and 24 months
- Safety and tolerability (up to 2 years)
- Rate of renal preservation (up to 2 years)
- Conversion from unresectable to resectable UTUC
Dr. Matin concluded that SURF303 is a global multicenter trial evaluating a highly selective FGFR3 inhibitor in patients with low-grade UTUC, a disease characterized by frequent FGFR3 alterations and limited kidney-sparing treatment options. The study aims to determine whether targeted FGFR3 inhibition with dabogratinib can achieve meaningful tumor responses while preserving renal units and minimizing the off-target toxicities associated with pan-FGFR inhibition.
Presented by: Surena Matin, MD, Professor, Department of Urology, Division of Surgery, The University of Texas MD Anderson Cancer Center, Houston, TX, USA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the EAU 2026 Annual Congress, London, UK, March 13th–16th, 2026
References:- Rouprêt M, Babjuk M, Burger M, et al. European Association of Urology guidelines on upper urinary tract urothelial carcinoma: 2017 update. Eur Urol. 2018;73(1):111-122.
- Lonergan PE, Porter SP. Testicular cancer: management of early-stage disease and surveillance strategies. Transl Androl Urol. 2020;9(4):1891-1896.
- Zhao J, Shen SS, Lerner SP, et al. Variant histology in bladder cancer: diagnostic, prognostic, and therapeutic implications. Adv Anat Pathol. 2024;31(2):80-87.
- Cutress ML, Stewart GD, Wells-Cole S, et al. The role of lymph node dissection in upper tract urothelial carcinoma: a systematic review. BJU Int. 2012;110(5):614-628.
- Matin SF, Sfakianos JP, Espiritu PN, et al. Patterns of recurrence and survival after nephroureterectomy for upper tract urothelial carcinoma: implications for postoperative surveillance. J Urol. 2024;211(6):784-793.
- Moss TJ, Qi Y, Xi L, et al. Comprehensive genomic characterization of upper tract urothelial carcinoma. Eur Urol. 2017;72(4):641-649.
- Nassar AH, Umeton R, Kim J, et al. Mutational analysis of upper tract urothelial carcinoma using next-generation sequencing: implications for targeted therapy. Clin Cancer Res. 2019;25(8):2458-2467.
- Sfakianos JP, Cha EK, Iyer G, et al. Genomic characterization of upper tract urothelial carcinoma. Eur Urol. 2015;68(6):970-977.
- Iabatte C, Shariat SF, Chromecki TF, et al. Prognostic factors in upper tract urothelial carcinoma: a comprehensive review. J Urol. 2023;209(5):872-881.
- Coleman JA, Clark PE, Bivalacqua TJ, et al. Contemporary management of upper tract urothelial carcinoma. J Urol. 2023;209(6):1071-1081.
- Khargi R, van Doorn HC, et al. Emerging molecular biomarkers in urothelial carcinoma. Transl Androl Urol. 2023;12(9):1439-1448.
- Chen AI, Kim J, Sfakianos JP, et al. Molecular subtypes of upper tract urothelial carcinoma and their clinical implications. Front Urol. 2022;2:916259.
- Starrett JH, Guo CC, Tamboli P, et al. Molecular characterization of variant histology in urothelial carcinoma. Mol Cancer Ther. 2025. doi:10.1158/1535-7163.MCT-25-0652.
- Tyra Biosciences, Inc. TYRA-300 clinical program corporate deck. Accessed January 9, 2026.
- National Library of Medicine. A study of TYRA-300 in advanced urothelial carcinoma (SURF301). ClinicalTrials.gov identifier: NCT07265947. Accessed January 26, 2026. Available at: https://clinicaltrials.gov/study/NCT07265947