(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to a thematic session jointly organized by the Advanced Prostate Cancer Consensus Conference (APCCC) and the EAU. Dr. Bertrand Tombal delivered a practical presentation titled “What Do You Need for Decision Making in mHSPC in 2026?”, focusing on how contemporary therapeutic choices in metastatic hormone-sensitive prostate cancer (mHSPC) should extend beyond disease volume alone and instead incorporate access to therapy, patient fitness, age, comorbidity burden, cognition, skeletal health, cardiovascular status, and drug-drug interactions.
Dr. Tombal began by outlining what clinicians often discuss in meetings when approaching treatment selection in mHSPC. These familiar domains include low- versus high-volume disease, asynchronous versus synchronous presentation, oligometastatic disease on modern imaging and metastasis-directed therapy, BRCA2 or other homologous recombination repair (HRR) alterations for potential PARP inhibitor use, PTEN loss for AKT inhibition, and PSMA expression for radioligand-based strategies. However, his central argument was that while these biologic and disease-state variables are important, they are insufficient on their own to guide real-world decision-making.
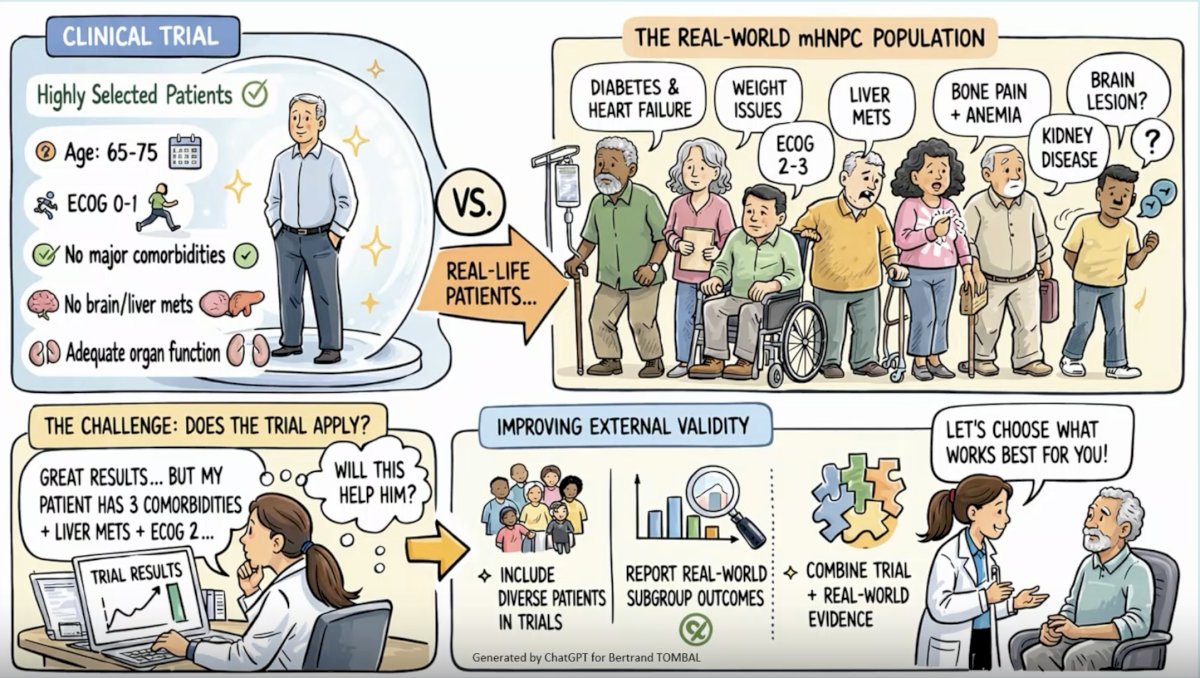
He next highlighted the disconnect between trial populations and real-world mHSPC populations. Clinical trials typically enroll highly selected patients: often age 65–75 years, ECOG performance status 0–1, no major comorbidities, no brain or liver metastases, and preserved organ function. In contrast, the real-world population encountered in the clinic is often older, frailer, and more medically complex, with diabetes, heart failure, weight issues, ECOG 2–3 performance status, liver metastases, bone pain with anemia, kidney disease, possible brain lesions, and multiple competing health concerns. As such, one of the fundamental challenges in treatment selection is external validity: do the trial results truly apply to the patient sitting in front of you? Dr. Tombal emphasized that better decision-making requires broader enrollment in trials, improved reporting of real-world subgroup outcomes, and thoughtful integration of randomized data with real-world evidence.
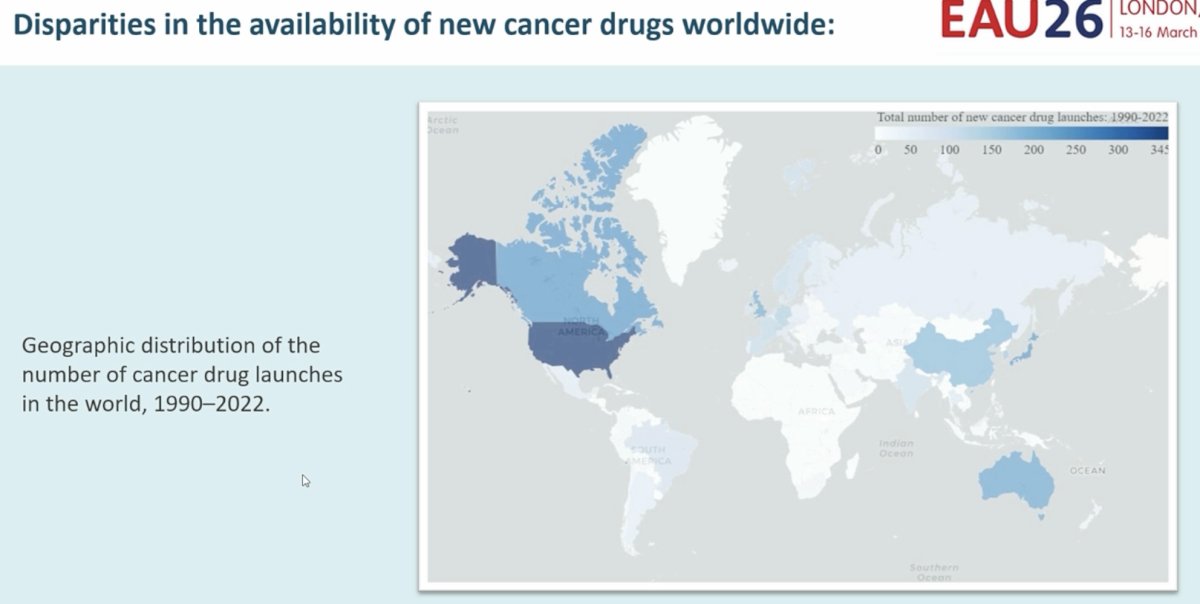
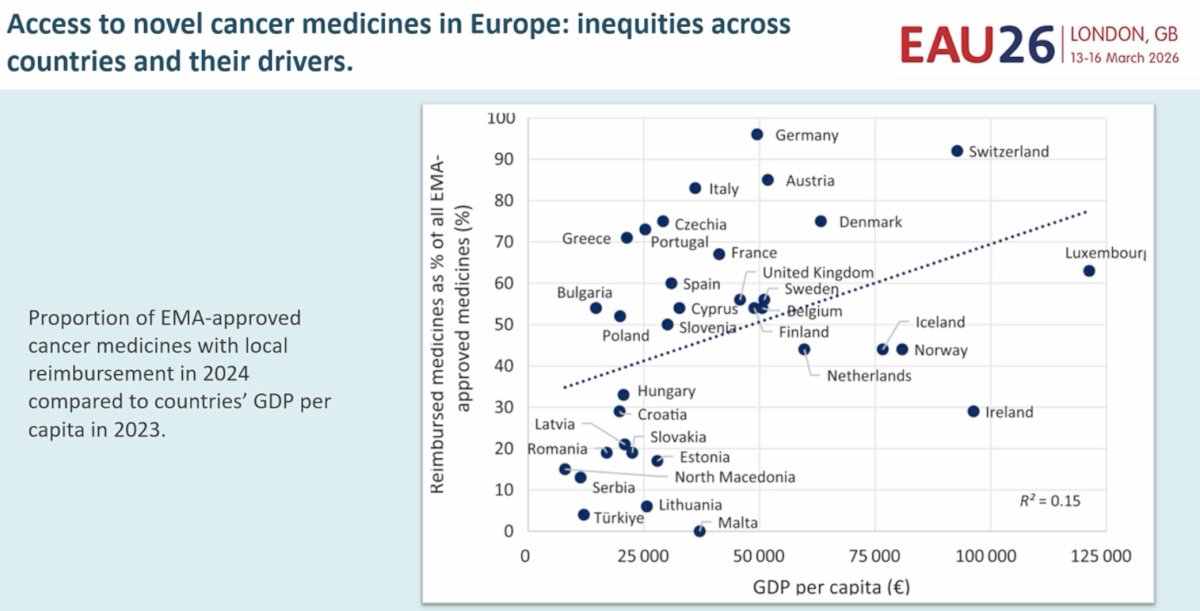
The talk then turned to age, hormone therapy, and ADT. Dr. Tombal asked a very practical question: where does the patient live, and what access or reimbursement coverage does he have for modern drugs? He emphasized that many patients around the world will not have access to modern ARPIs or other novel agents, and in those circumstances, treatment options may be constrained by economics and reimbursement rather than biology alone. To illustrate this point, he highlighted worldwide disparities in new cancer drug launches between 1990 and 2022, showing major geographic inequities, and then presented European data demonstrating that the proportion of EMA-approved cancer medicines reimbursed locally in 2024 varied substantially across countries and correlated only modestly with GDP per capita (R² = 0.15). Thus, access itself is a major determinant of therapeutic decision-making.
After establishing the issue of access, Dr. Tombal shifted to the question of age and treatment intensification. He reviewed data from Morgans and colleagues, published in NEJM Evidence in 2025,1 which assessed age and treatment intensification in metastatic hormone-sensitive prostate cancer. This analysis included 11 randomized comparisons totaling 13,648 patients, with 8,324 younger men and 5,162 older men in the aggregate meta-analysis. Individual patient data from three large trials, TITAN, ARASENS, and LATITUDE, were then used to validate the aggregate findings. Survival analyses were shown according to age (<70 versus ≥70 years), disease volume, and synchronous presentation. Among patients with low-volume synchronous disease aged ≥70 years, 4-year overall survival was 67% (95% CI: 60–74) with standard of care (SOC) plus ARPI versus 68% (95% CI: 63–74) with SOC alone, suggesting essentially no meaningful absolute gain. By contrast, in patients with low-volume synchronous disease <70 years, 4-year overall survival was 83% (95% CI: 79–88) with SOC plus ARPI versus 68% (95% CI: 63–74) with SOC alone, reflecting a substantial absolute benefit. A similar pattern was seen in high-volume synchronous disease. In patients aged ≥70 years, 4-year overall survival was 52% (95% CI: 48–56) with SOC plus ARPI versus 42% (95% CI: 38–47) with SOC alone, an approximate 10% absolute improvement. In those <70 years, 4-year overall survival was 58% (95% CI: 55–62) with SOC plus ARPI versus 41% (95% CI: 38–45) with SOC alone, an approximate 17% absolute gain. These data support the notion that treatment intensification benefits older patients, but to a lesser extent than younger patients.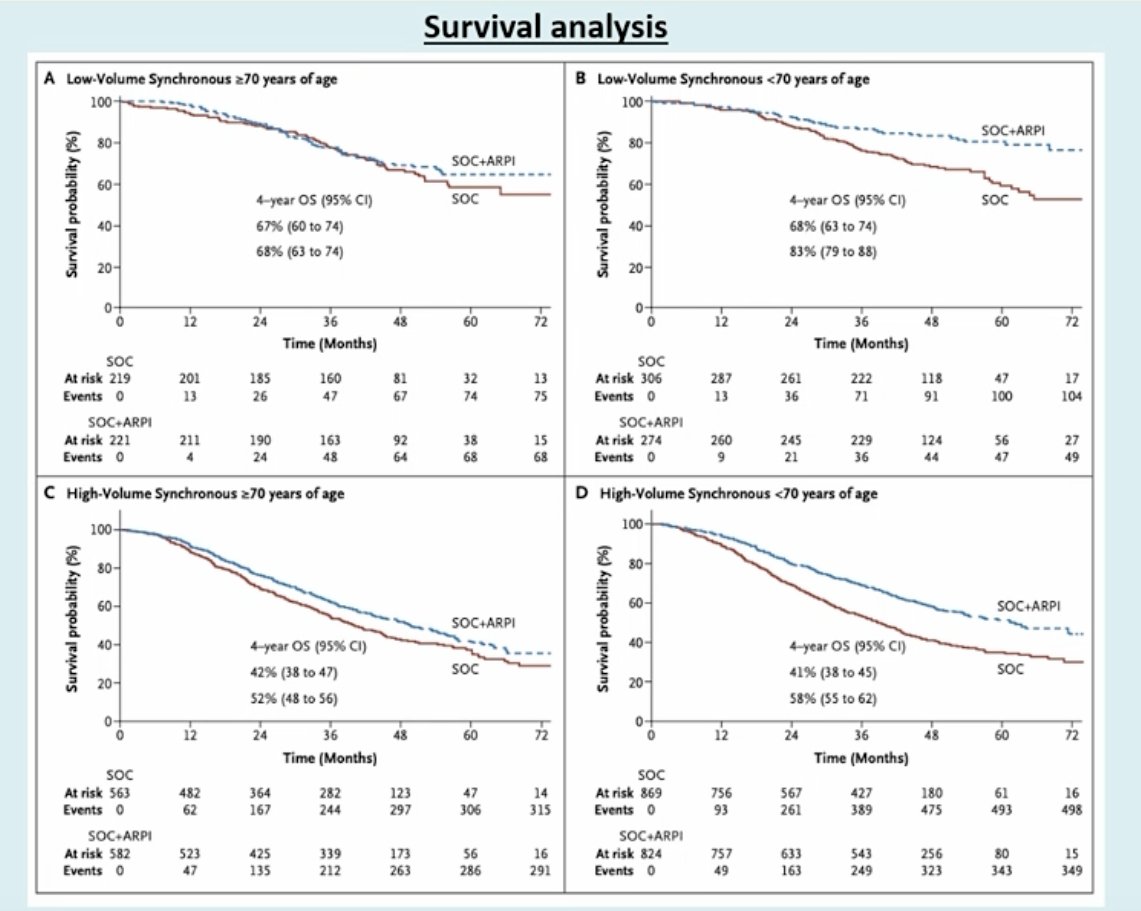
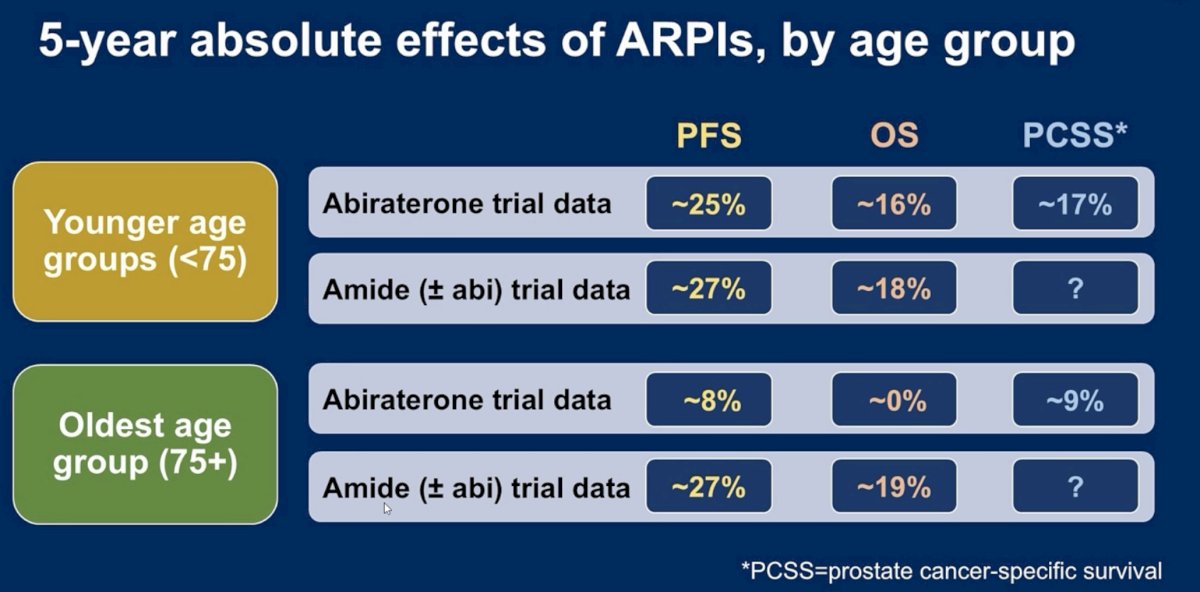
Dr. Tombal then presented a simplified summary of the 5-year absolute effects of ARPIs by age group. In patients younger than 75 years, abiraterone trial data suggested an approximately 25% improvement in progression-free survival, 16% in overall survival, and 17% in prostate cancer-specific survival. In the same younger age group, the “amide” trials, encompassing agents such as enzalutamide, apalutamide, and darolutamide, suggested approximately 27% improvement in PFS and 18% in OS. By contrast, in the oldest age group, defined as age 75 years or older, abiraterone trial data suggested only about an 8% PFS benefit and essentially 0% OS benefit, whereas the “amide” trial data appeared to preserve much of the efficacy, with approximately 27% PFS benefit and 19% OS benefit. This was one of the most practical messages from the talk: elderly patients derive less benefit from ADT plus ARPI overall, but the magnitude of attenuation may vary by agent class, with abiraterone appearing less favorable in the oldest subgroup.
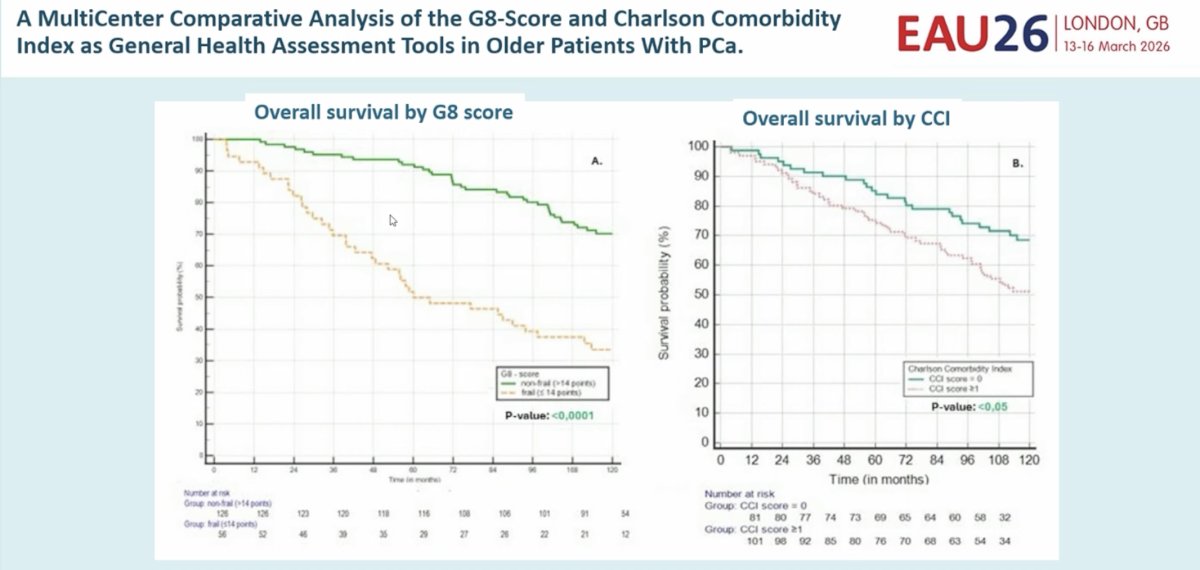
Dr. Tombal was careful to note that age alone is not enough, and he emphasized the need to consider broader health assessment tools. He presented data from a multicenter comparative analysis of the G8 score and the Charlson Comorbidity Index (CCI) as general health assessment tools in older patients with prostate cancer. Overall survival by G8 score showed a striking separation between non-frail patients and frail patients, with p<0.0001, whereas overall survival by CCI also separated significantly, though less robustly, with p<0.05. The implication was that frailty screening tools such as G8 may provide more clinically useful prognostic information than a pure comorbidity count and should be part of treatment decision-making in older patients.
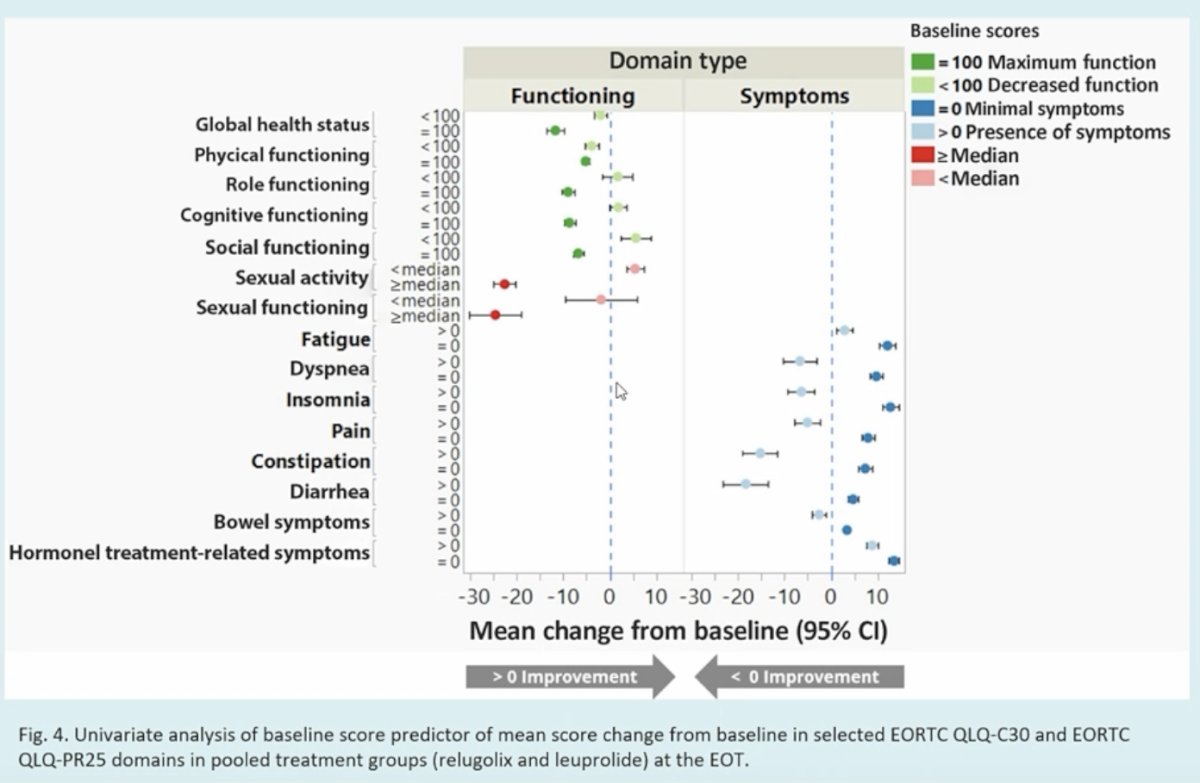
He next focused on quality of life and toxicity related to hormonal therapy. ADT negatively impacts health-related quality of life. In data presented by Tombal et al., baseline scores were strongly associated with the degree and type of deterioration. Patients with low baseline symptom scores, indicating little to no pre-existing symptom burden, were more likely to experience worsening symptoms, whereas those with maximal baseline functioning scores were more likely to experience declines in those functional domains over time.2 This reinforces the concept that ADT toxicity is not uniform and that pre-treatment patient-reported baseline function matters when counseling patients.
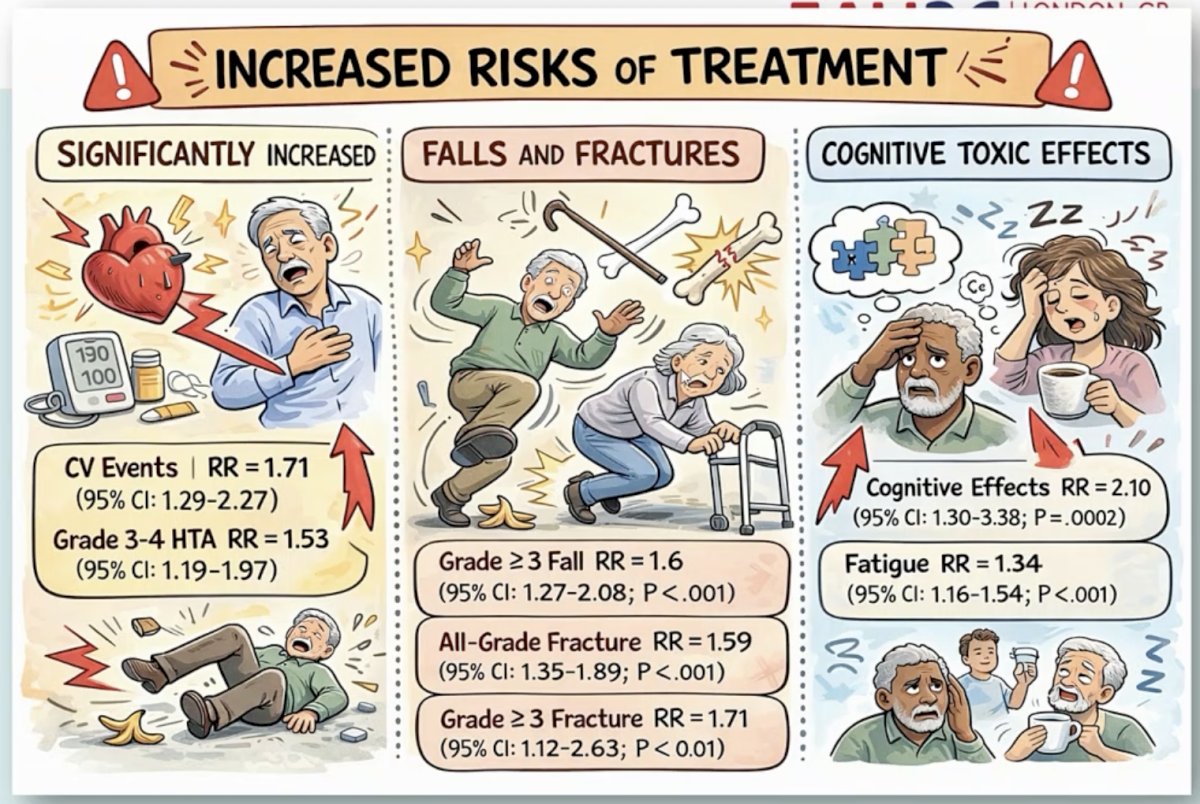
The toxicities associated with ARPIs were then reviewed in more detail. Dr. Tombal presented a summary highlighting increased risks across three major domains: cardiovascular toxicity, falls/fractures, and cognitive toxicity. Cardiovascular events were significantly increased, with a relative risk of 1.71 (95% CI: 1.29–2.27), and grade 3–4 hypertension also increased, with a relative risk of 1.53 (95% CI: 1.19–1.97). Skeletal and fall-related toxicity was also notable: grade ≥3 falls had a relative risk of 1.60 (95% CI: 1.27–2.08; p<0.001), all-grade fractures a relative risk of 1.59 (95% CI: 1.35–1.89; p<0.001), and grade ≥3 fractures a relative risk of 1.71 (95% CI: 1.12–2.63; p<0.01). Cognitive effects were particularly concerning, with cognitive toxicity showing a relative risk of 2.10 (95% CI: 1.30–3.38; p=0.0002), and fatigue also increased, with a relative risk of 1.34 (95% CI: 1.16–1.54; p<0.001). These data formed the basis of his later practical recommendations.
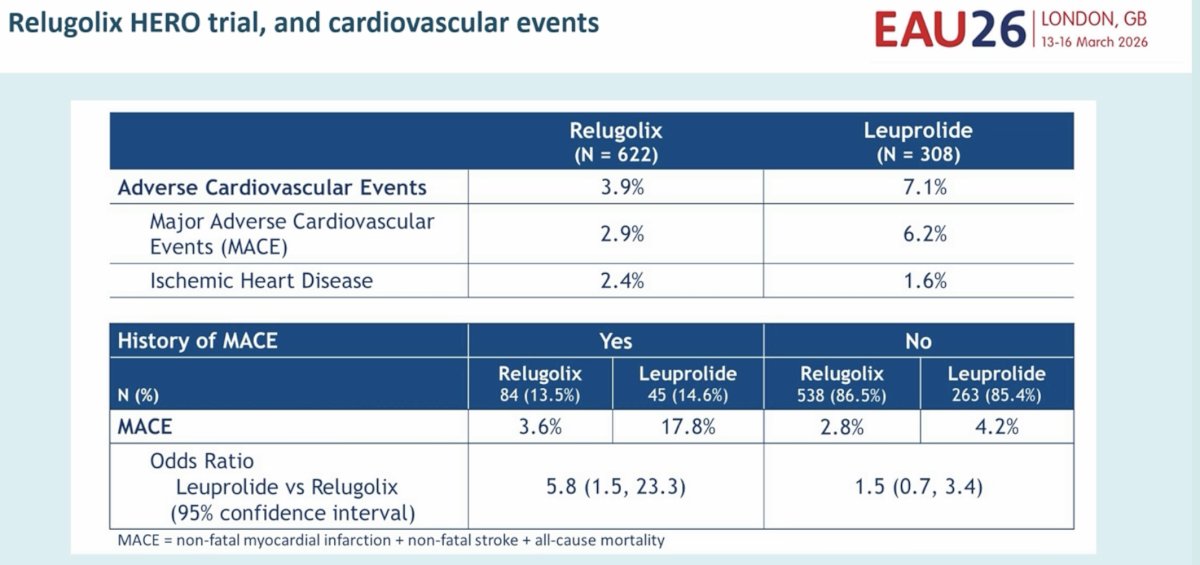
Dr. Tombal reviewed the HERO trial and cardiovascular events with relugolix versus leuprolide. In HERO, 622 patients received relugolix and 308 received leuprolide. Adverse cardiovascular events occurred in 3.9% versus 7.1%, respectively. Major adverse cardiovascular events occurred in 2.9% with relugolix versus 6.2% with leuprolide. Among patients with a prior history of MACE, the MACE rate was 3.6% with relugolix compared to 17.8% with leuprolide, corresponding to an odds ratio for leuprolide versus relugolix of 5.8 (95% CI: 1.5–23.3). In patients without a prior history of MACE, the corresponding rates were 2.8% and 4.2%, with an odds ratio of 1.5 (95% CI: 0.7–3.4).3 This provided strong support for the preferential use of an LHRH antagonist in patients with pre-existing cardiovascular disease. Dr. Tombal connected this directly to the EAU Prostate Cancer Guidelines, which note that cardiovascular side effects may be less frequent with LHRH antagonists than with agonists and that patients with pre-existing cardiovascular disease or other cardiovascular risk factors may be considered for antagonists if chemical castration is chosen.
Cognitive status was another major focus. Dr. Tombal introduced the Mini-Cog test as a brief cognitive screening instrument designed to quickly detect possible cognitive impairment or dementia in older adults, usually in under 3–5 minutes. He emphasized that it is intended as a triage tool to identify patients who may need more comprehensive neurocognitive evaluation, rather than as a stand-alone diagnostic instrument.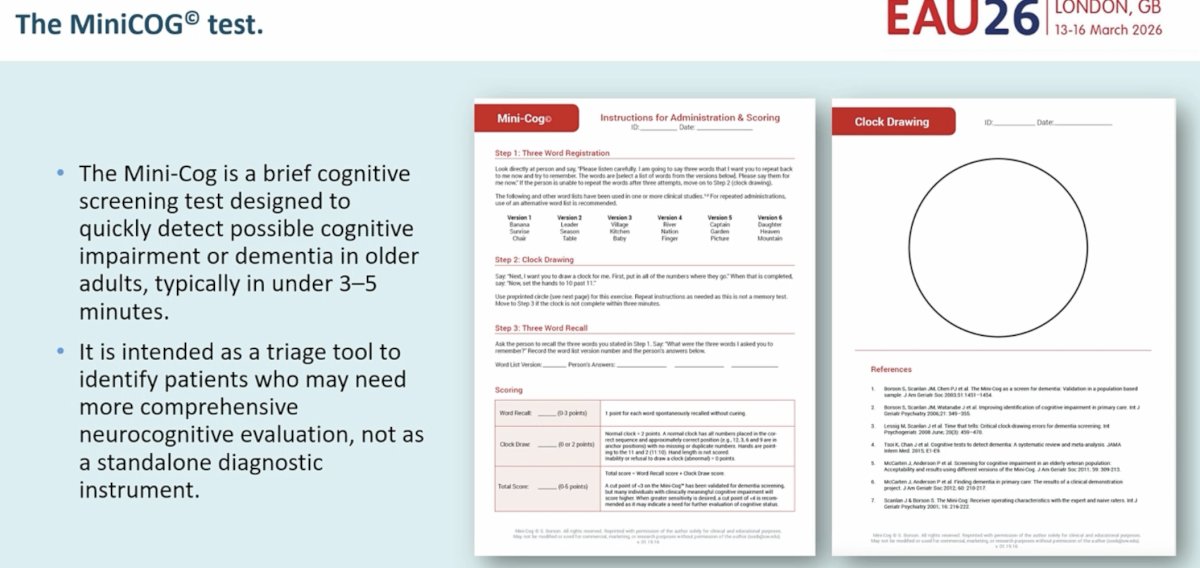
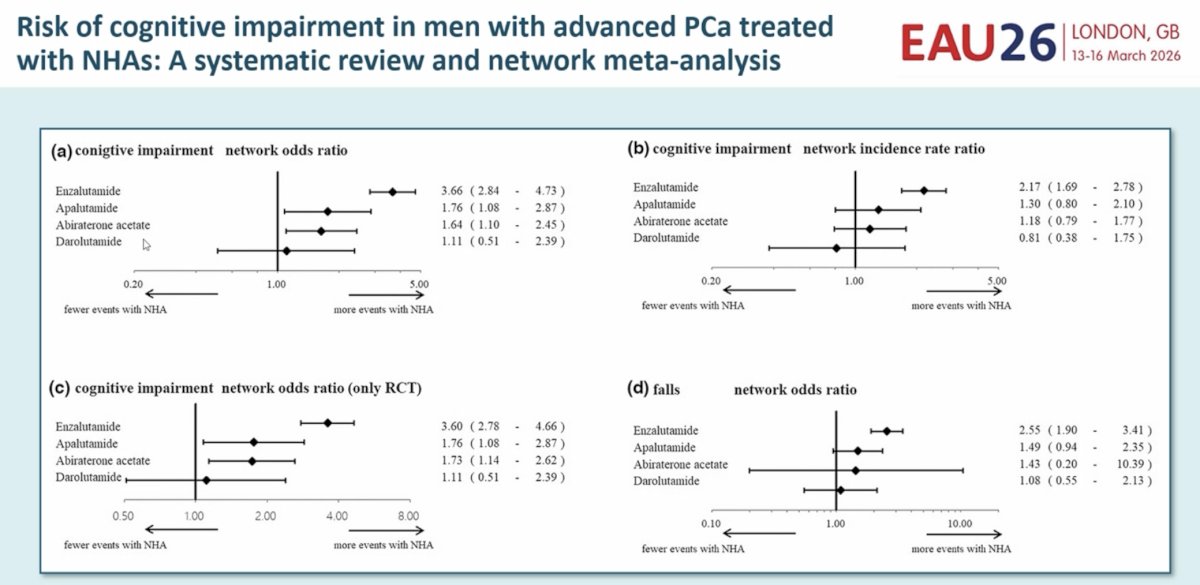
This was followed by a review of a systematic review and network meta-analysis examining the risk of cognitive impairment in men with advanced prostate cancer treated with novel hormonal agents. Compared with control, enzalutamide was associated with the greatest cognitive risk, with a network odds ratio of 3.66 (95% CI: 2.84–4.73) and an incidence rate ratio of 2.17 (95% CI: 1.69–2.78). In the RCT-only analysis, the odds ratio remained high at 3.60 (95% CI: 2.78–4.66). Apalutamide also increased cognitive risk, with an odds ratio of 1.76 (95% CI: 1.08–2.87), while abiraterone acetate showed a smaller but still significant signal, with an odds ratio of 1.64 (95% CI: 1.10–2.45). Darolutamide appeared comparatively neutral, with an odds ratio of 1.11 (95% CI: 0.51–2.39). For falls, enzalutamide again showed the largest signal, with a network odds ratio of 2.55 (95% CI: 1.90–3.41), whereas apalutamide, abiraterone, and darolutamide showed smaller and/or less precise estimates.4 Based on these data, Dr. Tombal recommended that patients with pre-existing cognitive decline should avoid enzalutamide and apalutamide when possible.
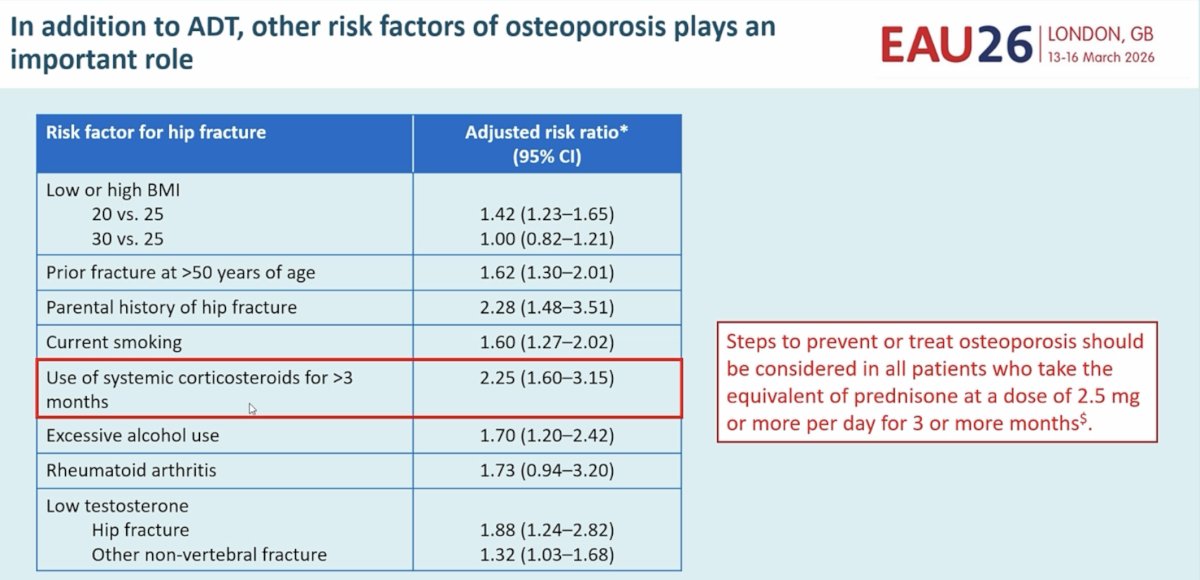
Skeletal health was addressed next. Dr. Tombal reminded the audience that, in addition to ADT itself, other risk factors for osteoporosis and fracture play an important role. He showed data for hip fracture risk demonstrating significant associations with low BMI, prior fracture after age 50 years, parental history of hip fracture, smoking, prolonged corticosteroid use, alcohol excess, rheumatoid arthritis, and low testosterone. Particularly notable was systemic corticosteroid use for more than 3 months, which carried an adjusted risk ratio of 2.25 (95% CI: 1.60–3.15).5 The practical implication is especially relevant for regimens that include chronic prednisone exposure, such as abiraterone. The slide specifically noted that steps to prevent or treat osteoporosis should be considered in all patients receiving the equivalent of prednisone 2.5 mg or more daily for 3 or more months. Consequently, Dr. Tombal recommended upfront bone loss prevention in patients with osteoporosis risk factors.
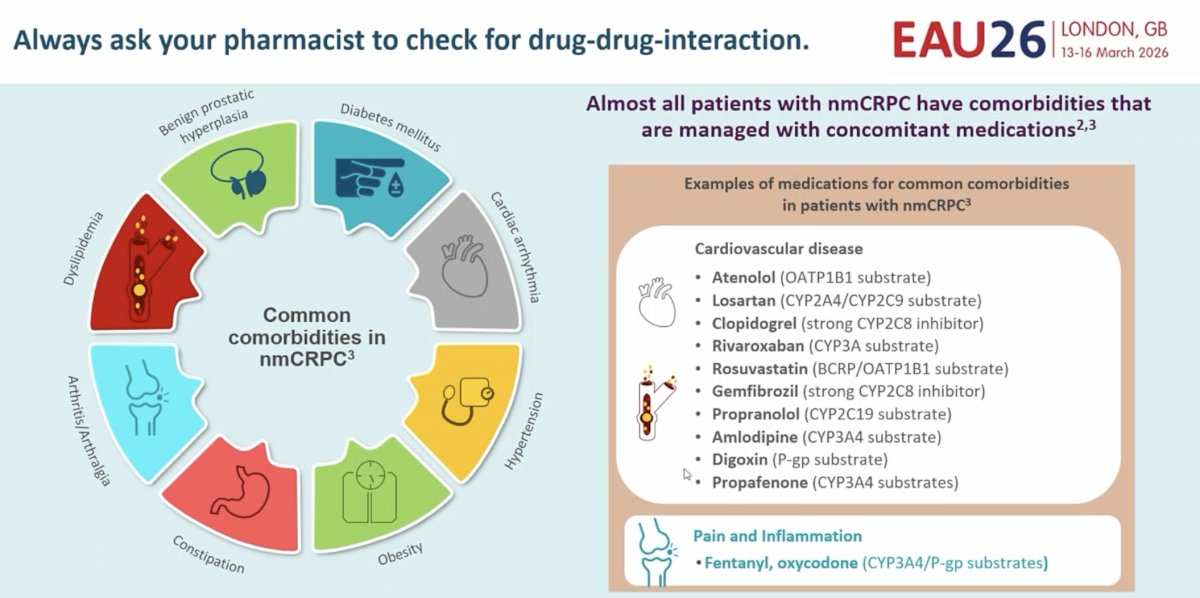
The final practical section addressed pharmacologic complexity. Dr. Tombal stressed that clinicians should always ask pharmacists to check for drug-drug interactions. He illustrated that almost all patients with advanced prostate cancer, particularly in later disease states such as nmCRPC, have comorbidities managed with concomitant medications. He listed common cardiovascular and pain medications with relevant CYP, P-gp, BCRP, or transporter interactions, underscoring how easily treatment exposure can be altered. He also warned clinicians not to forget to ask patients about plant extracts and herbal supplements. For second-generation ARTAs and relugolix, the main concern with plant extracts is indirect interaction through induction or inhibition of CYP3A4, CYP2C8, P-gp, or BCRP, or through androgenic effects that may alter drug exposure or counteract hormonal therapy. He noted that specific, well-studied herb-drug interaction pairs are scarce, which makes this area particularly difficult, but nonetheless clinically important.
Dr. Tombal concluded with a concise set of practical recommendations:
- First, many patients will unfortunately not have access to modern drugs, so real-world options may be limited by reimbursement and geography.
- Second, elderly patients derive less benefit from ADT plus ARPI and may experience more severe side effects; patients with severe comorbid status may die from competing causes more rapidly.
- Third, cognitive, skeletal, and cardiovascular status should be formally assessed prior to treatment selection.
- Specifically, patients with pre-existing cognitive decline should avoid enzalutamide and apalutamide; patients with pre-existing cardiovascular disease should avoid LHRH agonists and abiraterone when possible; and patients with risk factors for osteoporosis should receive upfront bone loss prevention.
- Finally, drug-drug interactions must be carefully checked when choosing and administering an ARPI, and clinicians should remain aware of plant-drug interactions as well.
Overall, Dr. Tombal’s presentation was a timely reminder that decision-making in mHSPC in 2026 is no longer simply a question of disease volume, de novo versus metachronous presentation, or molecular profile. While those tumor-related features remain important, optimal treatment selection increasingly requires integration of access, age, frailty, cognition, cardiovascular risk, skeletal health, quality of life, and concomitant medication burden. In other words, the best therapy is not just the most active regimen from a clinical trial, but the regimen that is both effective and realistically deliverable for the specific patient in front of us.
Presented by: Bertrand Tombal, MD, PhD, Chairman of the Department of Surgery and Full Professor of Urology at the Université Catholique de Louvain, Ottignies-Louvain-la-Neuve, Belgium
- Morgans AK, Chen YH, Sweeney CJ, et al. Age and treatment intensification in metastatic hormone-sensitive prostate cancer. N Engl J Med Evid. 2025;4(11):EVIDoa2500109.
- Tombal B, Saad F, Penson DF, et al. Health-related quality of life effects of androgen deprivation therapy in prostate cancer: a systematic review and meta-analysis. Eur Urol. 2023;84(6):579-587.
- Shore ND, Saad F, Cookson MS, et al. Oral relugolix for androgen-deprivation therapy in advanced prostate cancer. N Engl J Med. 2020;382(23):2187-2196.
- Huang SW, Tsai CY, Hsu CY, et al. Risk of cognitive impairment in men with advanced prostate cancer treated with novel hormonal agents: a systematic review and network meta-analysis. Clin Transl Sci. 2023;16(2):313-325.
- Hayat S, Rosenthal N, Elaraj D, et al. Glucocorticoid-induced osteoporosis: prevention and treatment strategies. Cleve Clin J Med. 2020;87(7):417-426.