(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to a thematic session jointly organized by the Advanced Prostate Cancer Consensus Conference (APCCC) and the EAU. Dr. Chris Parker presented on the management of macroscopic local relapse after radical prostatectomy in the setting of high-risk non-metastatic hormone-sensitive prostate cancer (nmHSPC), focusing on three practical questions: what radiotherapy dose should be used, what should be included in the radiotherapy target volume, and what role systemic therapy should play.
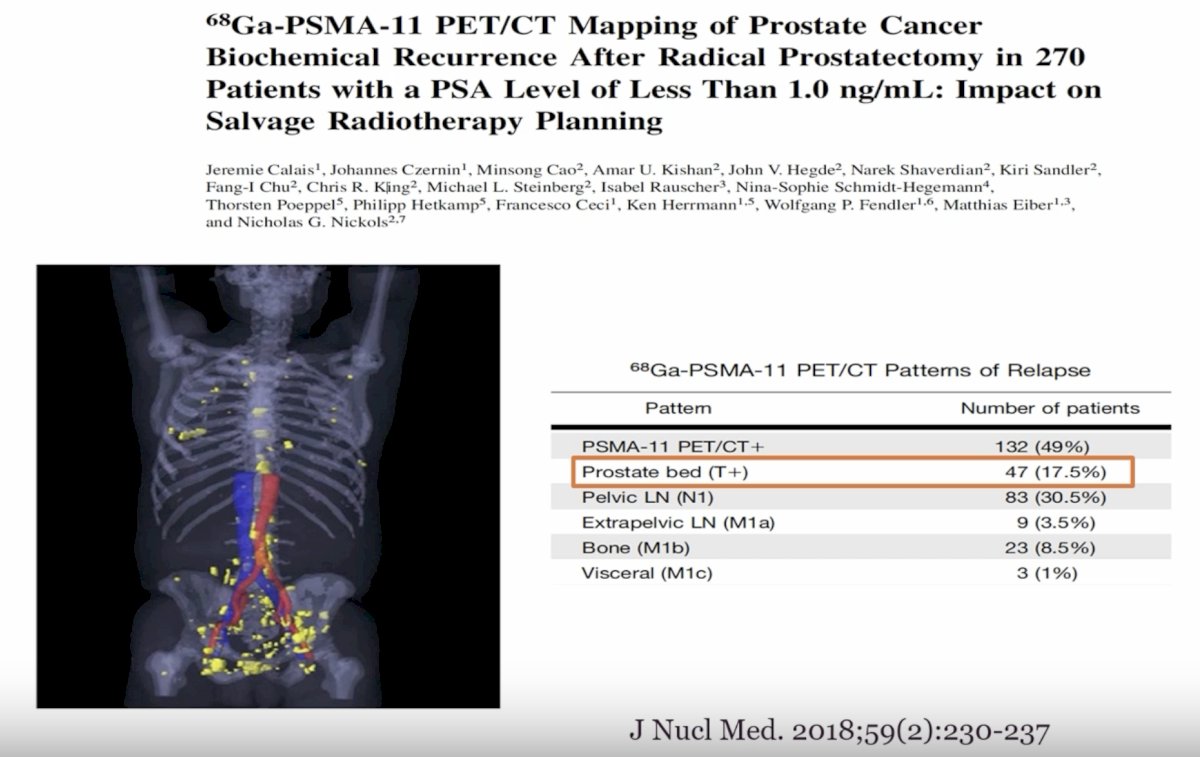
Dr. Parker began by emphasizing that this is an unusual clinical scenario. In routine practice, salvage prostate bed radiotherapy is usually delivered much earlier, often when the PSA is around 0.2 ng/mL. By the time a patient develops a visible or macroscopic relapse after radical prostatectomy, the concern is that recurrence may not be confined to the prostate bed. This point is supported by PSMA PET imaging data. He highlighted the 68Ga-PSMA-11 PET/CT mapping study by Calais and colleagues, which evaluated 270 patients with biochemical recurrence after radical prostatectomy and a PSA <1.0 ng/mL. In that cohort, 132 patients (49%) had a positive PSMA PET scan. Importantly, only 47 patients (17.5%) had recurrence confined to the prostate bed, whereas pelvic lymph node involvement was seen in 83 patients (30.5%), extrapelvic lymph nodes in 9 patients (3.5%), bone metastases in 23 patients (8.5%), and visceral disease in 3 patients (1%).1 These data reinforce that relapse after radical prostatectomy is commonly not local only, even at relatively low PSA values, and that visible local recurrence should be interpreted in the broader context of potential occult regional or distant disease.
Dr. Parker then structured the remainder of his talk around three management domains: radiotherapy dose, radiotherapy target, and systemic treatment.
With respect to radiotherapy dose, he argued that there is no good evidence supporting dose escalation in the postoperative salvage setting. He referenced the SAKK 09/10 trial, a randomized phase III study evaluating conventional-dose versus dose-intensified salvage radiotherapy for biochemically recurrent prostate cancer after prostatectomy. In this study, 344 men were randomized to prostate bed radiotherapy to either 64 Gy (n=170) or 70 Gy (n=174). The primary endpoint was freedom from biochemical progression. At long-term follow-up, dose intensification did not improve outcomes, with a hazard ratio of 1.14 (95% CI: 0.82–1.60; log-rank p=0.44).2 Thus, escalating from 64 Gy to 70 Gy did not translate into better biochemical control, while previous reports from this trial have also shown greater toxicity with the higher dose. Based on these data, Dr. Parker concluded that there is no good evidence for routine dose escalation. His practical recommendation was to use 52.5 Gy in 20 fractions to the prostate bed and 55 Gy in 20 fractions to the macroscopic recurrence.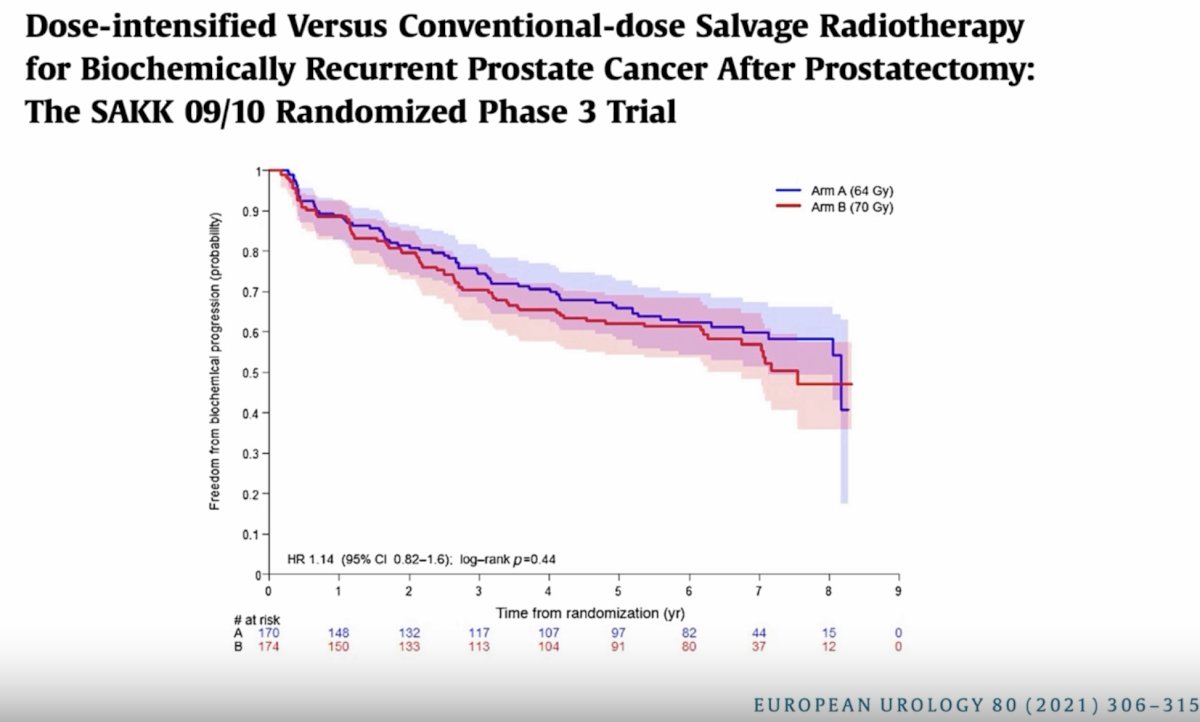
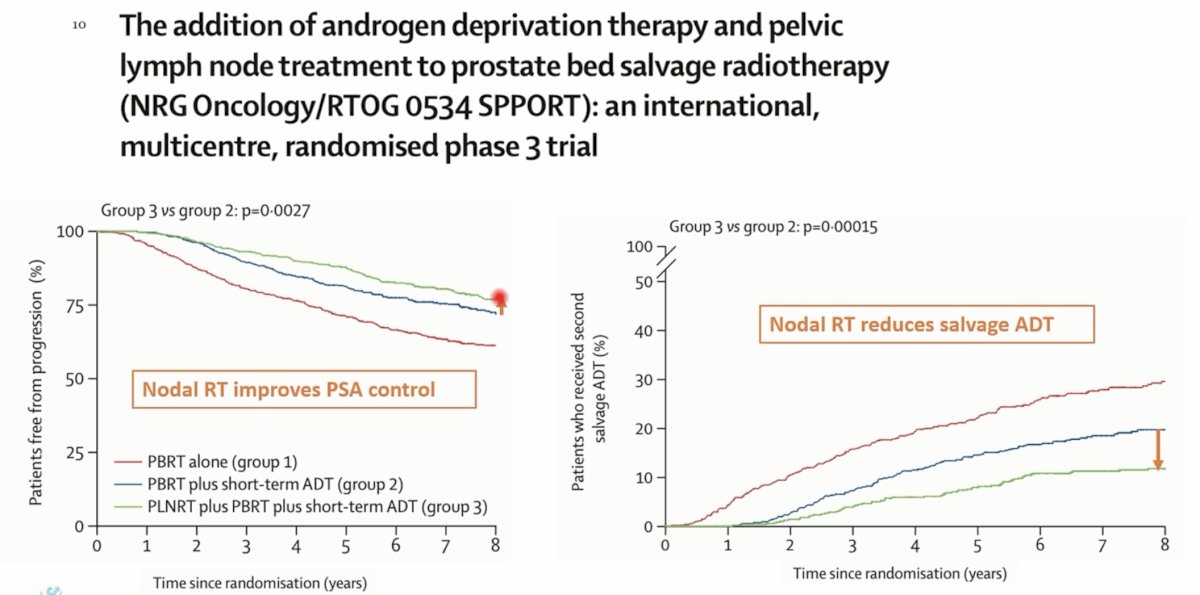
The second question is radiotherapy target volume, specifically whether treatment should be limited to the prostate bed or should also include pelvic lymph nodes. Dr. Parker highlighted the SPPORT trial, NRG Oncology/RTOG 0534, an international, multicenter, randomized phase III trial evaluating whether short-term androgen deprivation therapy (ADT) and pelvic nodal radiotherapy improve outcomes when added to salvage prostate bed radiotherapy. A total of 1,764 patients were randomized to one of three groups: prostate bed radiotherapy alone, prostate bed radiotherapy plus 4–6 months of hormone therapy, or prostate bed plus pelvic lymph node radiotherapy plus 4–6 months of hormone therapy. The main endpoint was biochemical progression-free survival.3
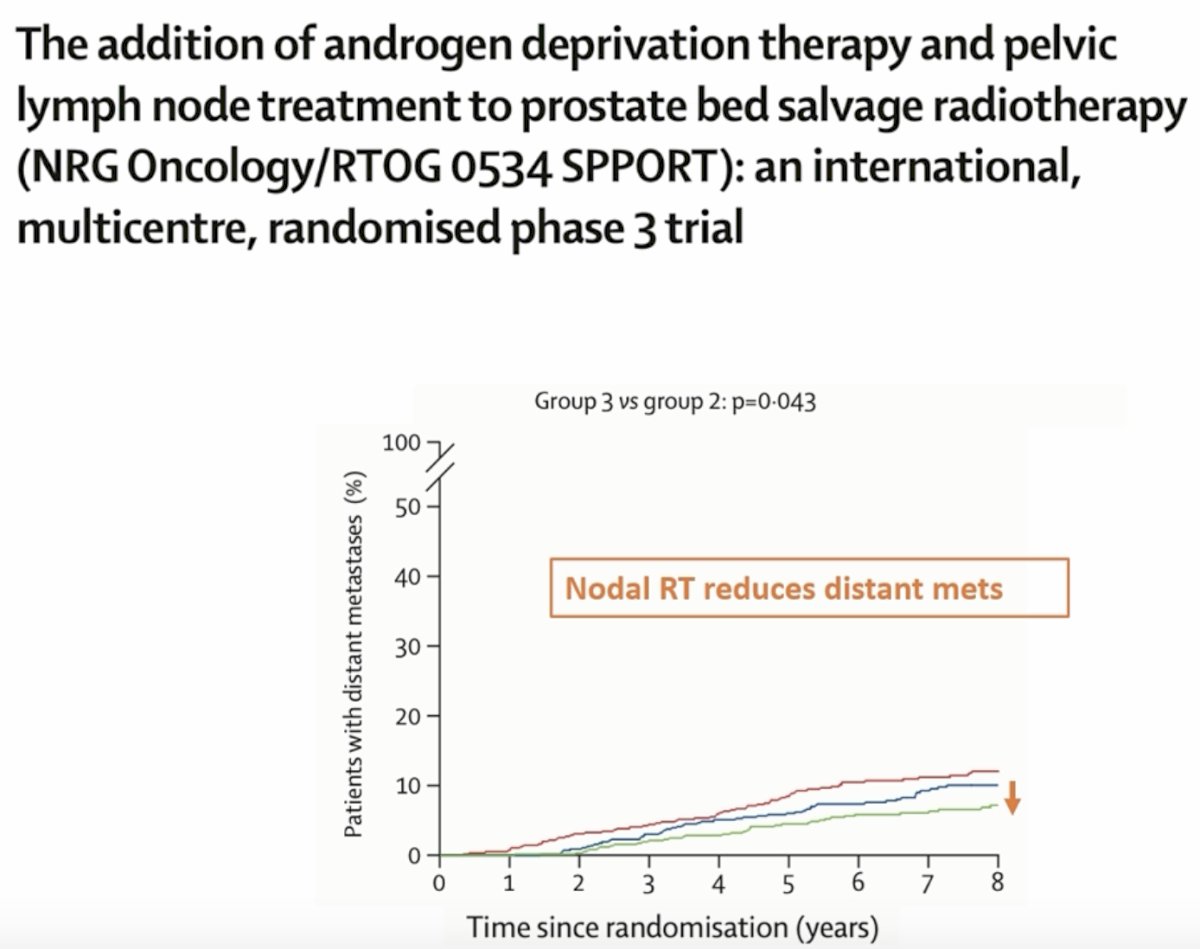
Dr. Parker focused on the comparison most relevant to the management of high-risk macroscopic local relapse, namely the addition of pelvic nodal radiotherapy to prostate bed radiotherapy plus short-term ADT. This intensification strategy improved PSA control, with the comparison between group 3 and group 2 reaching significance (p=0.0027). It also reduced the need for salvage ADT (p=0.00015) and reduced the rate of distant metastases (p=0.043). On this basis, he concluded that there is evidence of benefit for nodal radiotherapy, particularly in terms of time to ADT and freedom from distant metastases. He therefore recommended that nodal radiotherapy should be considered in light of broader clinicopathologic risk features, including T stage, tumor volume, Gleason score, extent of nodal dissection, PSA doubling time, and time since radical prostatectomy.
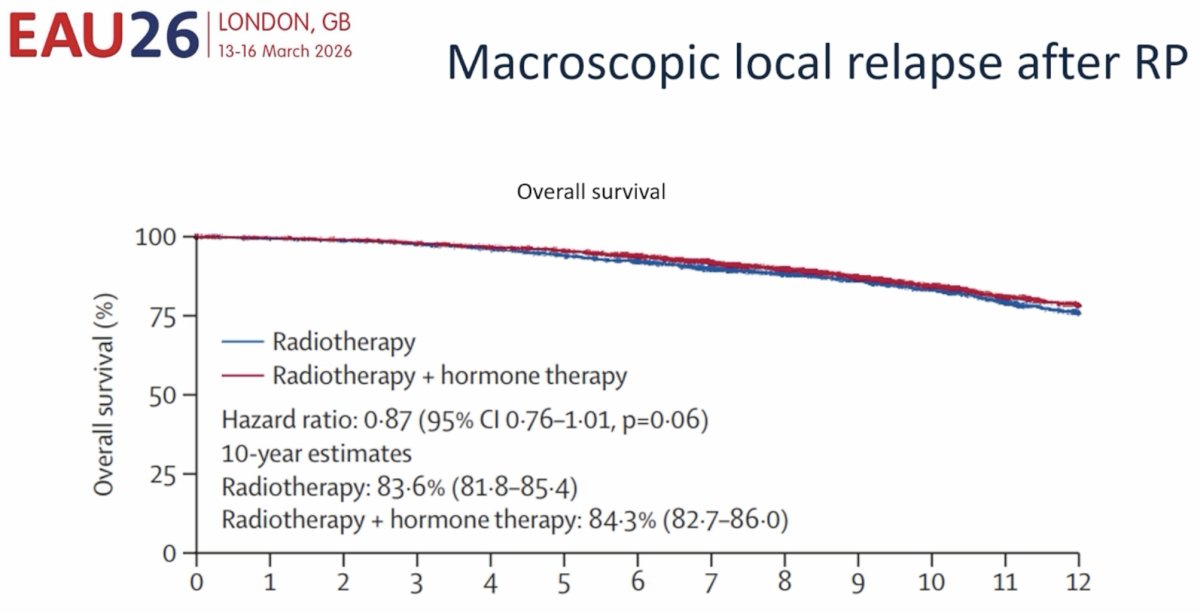
The third domain was systemic treatment. Dr. Parker reviewed the recently presented individual patient data meta-analysis examining hormone therapy use and duration with postoperative radiotherapy for recurrent prostate cancer. This meta-analysis, referred to in the talk as POSEIDON and presented by Kishan et al. at GU ASCO 2026,4 pooled approximately 5,000 patients. The comparison included 2,216 patients treated with radiotherapy alone and 2,810 treated with radiotherapy plus hormone therapy, with a median follow-up of 9.10 years in both groups. Baseline characteristics were broadly balanced, with a median PSA of 0.3 ng/mL in both cohorts, and the majority of patients had Gleason 7 disease.
In the overall population, the addition of hormone therapy to radiotherapy produced at most a modest overall survival benefit, which did not meet conventional statistical significance. The hazard ratio for overall survival was 0.87 (95% CI: 0.76–1.01; p=0.06). Ten-year overall survival estimates were 83.6% (95% CI: 81.8–85.4) with radiotherapy alone and 84.3% (95% CI: 82.7–86.0) with radiotherapy plus hormone therapy.
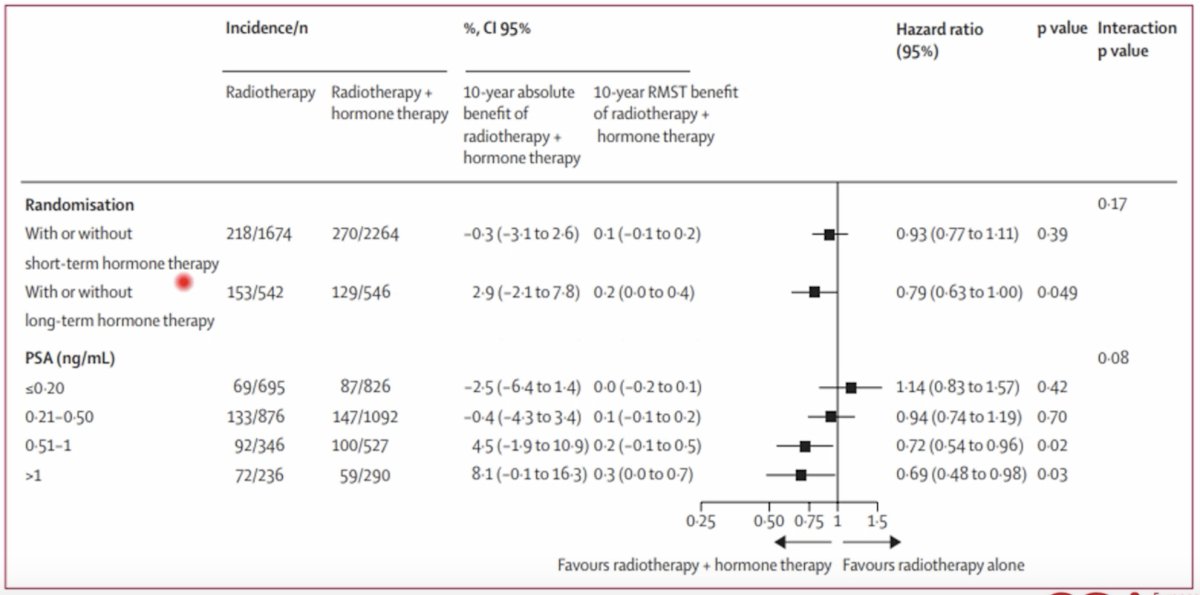
However, subgroup analyses were informative. Short-term hormone therapy was not associated with a significant OS benefit compared with no hormone therapy (HR: 0.93, 95% CI: 0.77–1.11; p=0.39), whereas long-term hormone therapy was associated with a borderline significant benefit (HR: 0.79, 95% CI: 0.63–1.00; p=0.049). The apparent benefit of hormone therapy also varied according to PSA level at the time of salvage treatment. For PSA ≤0.20 ng/mL, the hazard ratio was 1.14 (95% CI: 0.83–1.57; p=0.42); for PSA 0.21–0.50 ng/mL it was 0.94 (95% CI: 0.74–1.19; p=0.70); for PSA 0.51–1.0 ng/mL it was 0.72 (95% CI: 0.54–0.96; p=0.02); and for PSA >1.0 ng/mL it was 0.69 (95% CI: 0.48–0.98; p=0.03). Although the interaction p-value was 0.08, the pattern suggests that any overall survival benefit from hormone therapy is more likely to emerge in patients treated at higher PSA levels.
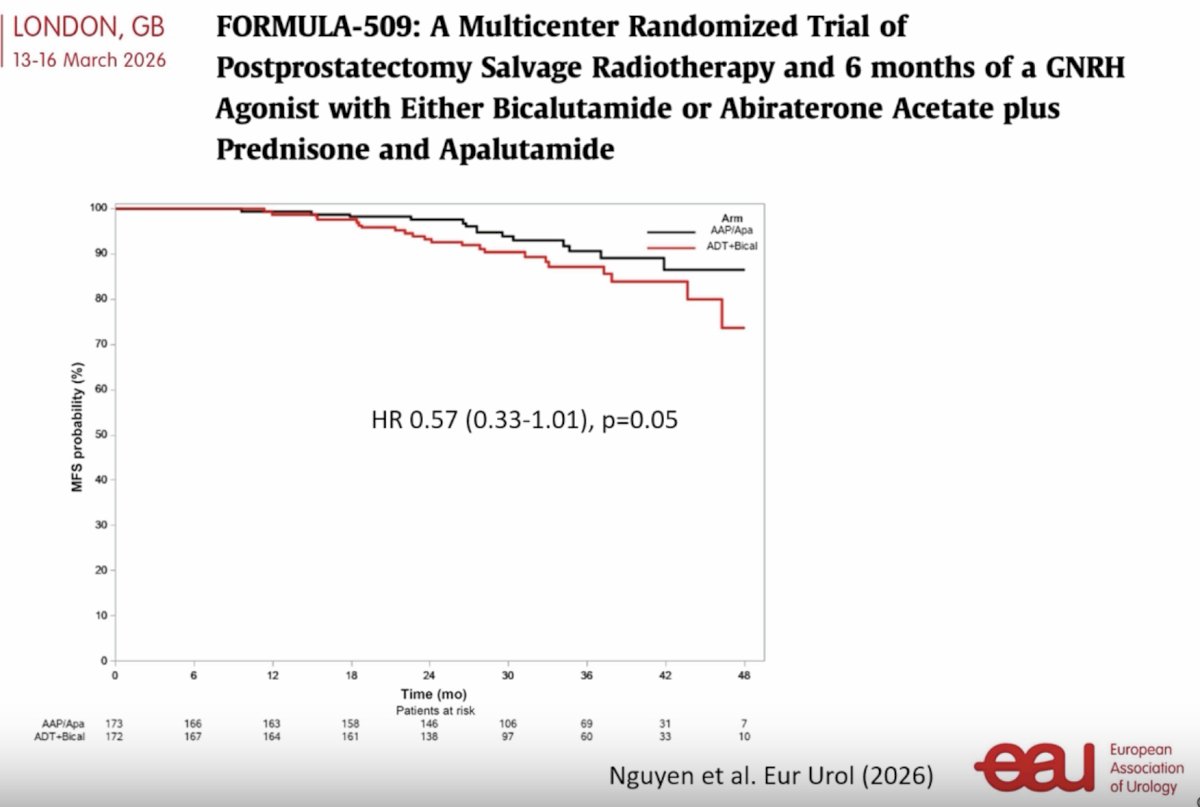
Dr. Parker also reviewed the FORMULA-509 trial, a multicenter randomized study of post-prostatectomy salvage radiotherapy plus 6 months of a GnRH agonist combined with either bicalutamide or intensified androgen receptor pathway inhibition using abiraterone acetate/prednisone plus apalutamide. Approximately 345 patients were randomized, with 173 in the abiraterone/apalutamide arm and 172 in the ADT plus bicalutamide arm. The metastasis-free survival curves favored intensified therapy, with a hazard ratio of 0.57 (95% CI: 0.33–1.01; p=0.05). While not definitively practice-changing on its own, this study suggests that systemic intensification may improve outcomes in selected high-risk patients, though the magnitude of benefit remains modest and should be weighed against toxicity and patient risk profile.
Integrating these data, Dr. Parker’s practical conclusions were straightforward:
- For radiotherapy dose, there is no good evidence to support dose escalation; he favored 52.5 Gy in 20 fractions to the prostate bed and 55 Gy in 20 fractions to the macroscopic recurrence.
- For radiotherapy target volume, there is evidence supporting nodal radiotherapy, particularly through improvements in PSA control, time to salvage ADT, and freedom from distant metastases, and nodal treatment should be considered in light of adverse pathologic and clinical features.
- For systemic treatment, the evidence suggests a modest, if any, overall survival benefit from ADT overall, with benefit more likely in patients with higher PSA levels and in those receiving longer duration therapy. In particular, he recommended ADT for patients who are also receiving nodal radiotherapy.
Overall, Dr. Parker highlighted that macroscopic local relapse after RP is an uncommon but clinically important scenario that requires a nuanced, risk-adapted approach. The visible lesion should not be viewed in isolation, as PSMA PET data show that relapse after prostatectomy is frequently not local only. Management, therefore, extends beyond simply targeting the prostate bed lesion. Rather, optimal treatment requires careful consideration of radiotherapy dose, regional target coverage, and judicious use of systemic therapy according to the patient’s broader risk profile.
Presented by: Chris C. Parker, MD, FRCR, Professor, Royal Marsden Hospital, London, UK
References:
- Calais J, Czernin J, Cao M, et al. 68Ga-PSMA-11 PET/CT mapping of prostate cancer biochemical recurrence after radical prostatectomy in 270 patients with a PSA level of less than 1.0 ng/mL: impact on salvage radiotherapy planning. J Nucl Med. 2018;59(2):230-237.
- Ghadjar P, Hayoz S, Bernhard J, et al. Dose-intensified versus conventional-dose salvage radiotherapy for biochemically recurrent prostate cancer after prostatectomy: the SAKK 09/10 randomized phase 3 trial. Eur Urol. 2021;80(3):306-315.
- Pollack A, Karrison TG, Balogh AG Jr, et al. The addition of androgen deprivation therapy and pelvic lymph node treatment to prostate bed salvage radiotherapy (NRG Oncology/RTOG 0534 SPPORT): an international, multicentre, randomised phase 3 trial. Lancet. 2022;399(10338):1886-1901.
- Kishan AU, Sun Y, Parker C, et al. Hormone therapy use and duration with postoperative radiotherapy for recurrent prostate cancer: an individual patient data meta-analysis. Lancet. 2026;S0140-6736(26)00137-6.
- Nguyen PL, Kollmeier MA, Rathkopf DE, et al. FORMULA-509: A multicenter randomized trial of postprostatectomy salvage radiotherapy and 6 months of a GnRH agonist with either bicalutamide or abiraterone acetate plus prednisone and apalutamide. Eur Urol. 2026.