(UroToday.com) The European Association of Urology (EAU) 2026 Annual Congress was host to an advanced prostate cancer session hosted jointly by the Advanced Prostate Cancer Consensus Conference (APCCC) and the EAU. Dr. Isabel Heidegger delivered an update on high-risk, non-metastatic hormone-sensitive prostate cancer (nmHSPC).
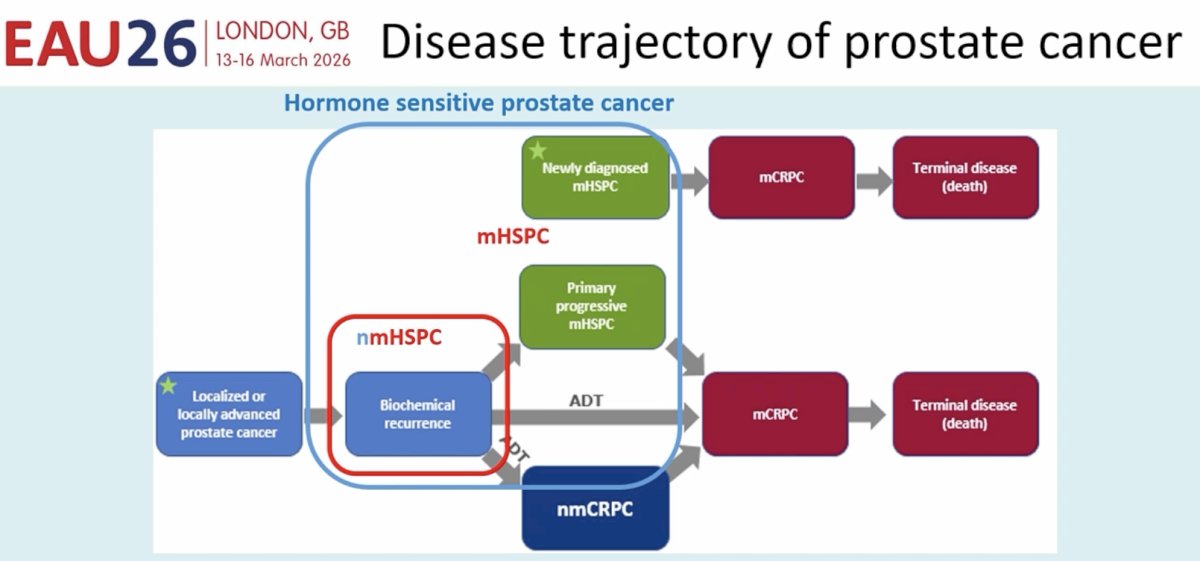
She noted that nmHSPC exists on a ‘continuum’ from localized/locally advanced prostate cancer to metastatic HSPC, with 25-30% of patients receiving primary localized therapy experiencing biochemical recurrence within 10 years of therapy.
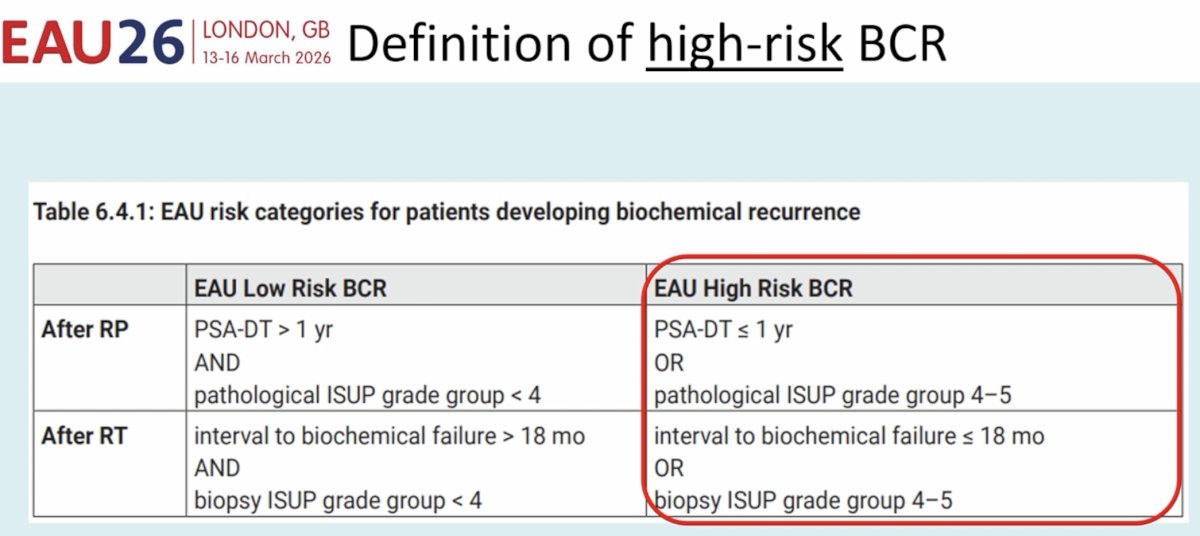
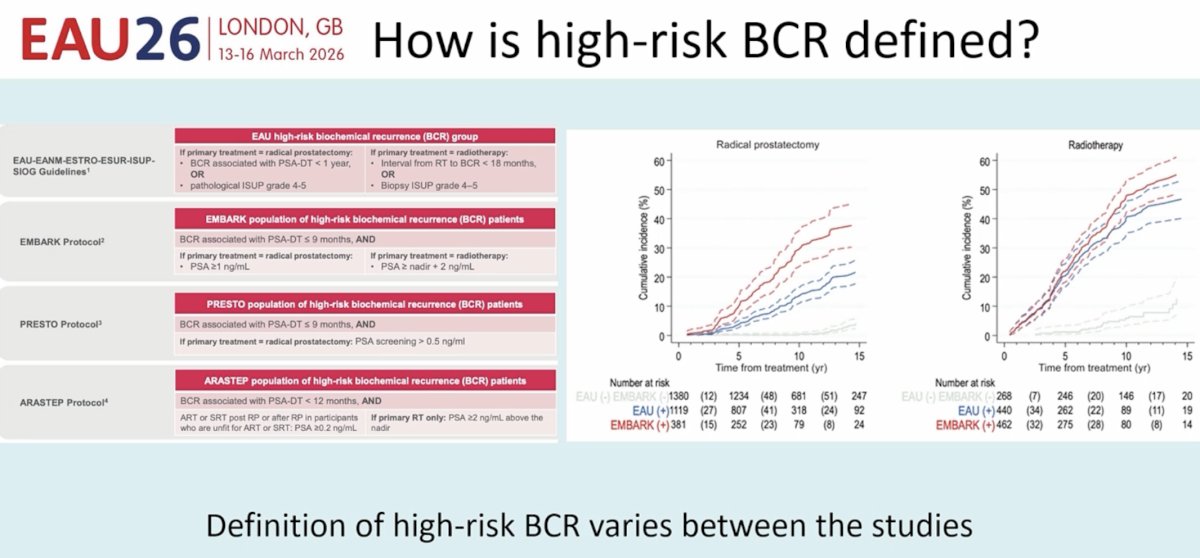
As such, stratifying patients with biochemical recurrence into low- and high-risk groups becomes important to guide management decisions. Following radical prostatectomy, EAU high-risk biochemical recurrences are those that are associated with a PSA doubling time ≤1 year or occurring in patients with pathologic ISUP Grade Group 4-5 disease. Conversely, following radiotherapy, high-risk features include an interval of ≤18 months to biochemical failure or biopsy ISUP Grade Group 4-5 disease.
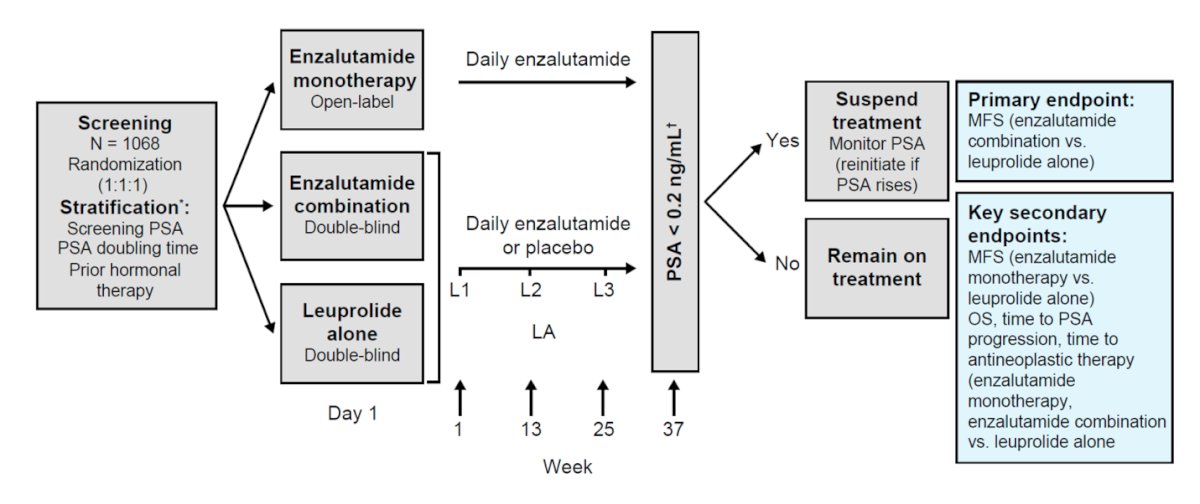
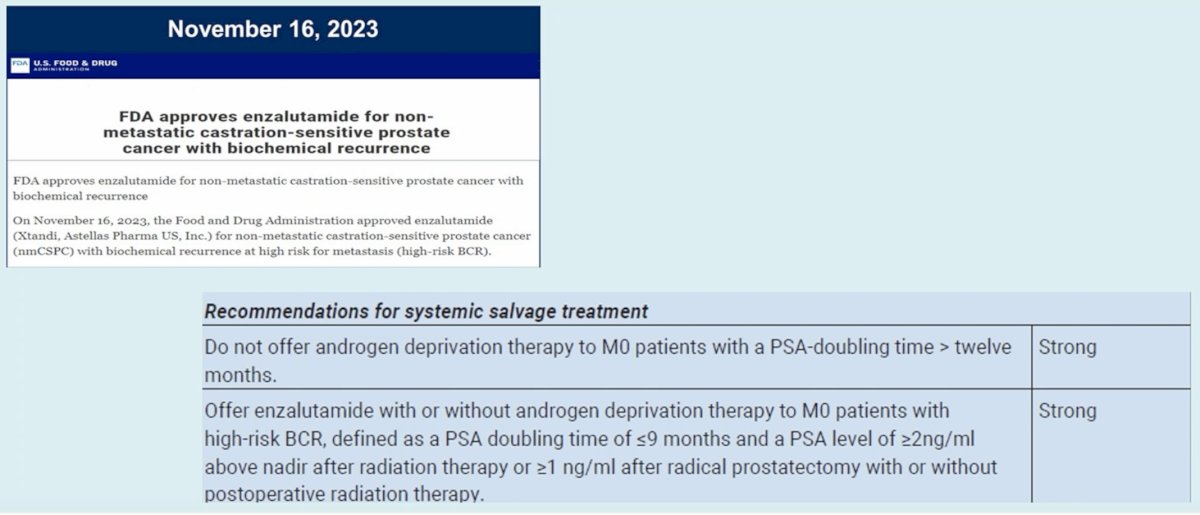
Dr. Heidegger next discussed the use of enzalutamide +/- ADT for patients with high-risk biochemical recurrence. EMBARK is a randomized phase III trial of biochemically recurrent prostate cancer patients who had evidence of high-risk disease, defined as PSADT ≤9 months and a PSA level of ≥2 ng per milliliter above nadir following radiation therapy or ≥1 ng per milliliter after radical prostatectomy, with or without postoperative radiation therapy.1 Eligible patients had no evidence of metastasis on conventional imaging and baseline eugonadal testosterone levels ≥150 ng/dL. Hormone therapy ≥9 months prior to enrolment was permitted. Patients underwent 1:1:1 randomization as follows:
- Enzalutamide 160 mg + leuprolide acetate (blinded arm)
- Placebo + leuprolide acetate (blinded arm)
- Enzalutamide monotherapy (unblinded arm)
Notably, EMBARK was not only a trial of systemic therapy intensification, but also evaluated treatment de-intensification based on the 36-week serum PSA level, as follows:
- PSA <0.2: Treatment was suspended at week 37, and PSA was monitored with treatment reinitiated if PSA rose again
- PSA >0.2: Treatment was continued
The primary study endpoint was metastasis-free survival, assessed via blinded independent central review, in the enzalutamide + leuprolide versus leuprolide arms only. The study design is summarized below:
The study cohort included 1,068 patients. The median serum PSA level at study entry was 5–5.5 ng/ml. The median PSADT was 4.6–5 months, with approximately 20% of patients having a PSADT ≤3 months. Half of the cohort had undergone both radical prostatectomy and radiation therapy. 30% of patients had received prior hormonal therapy.
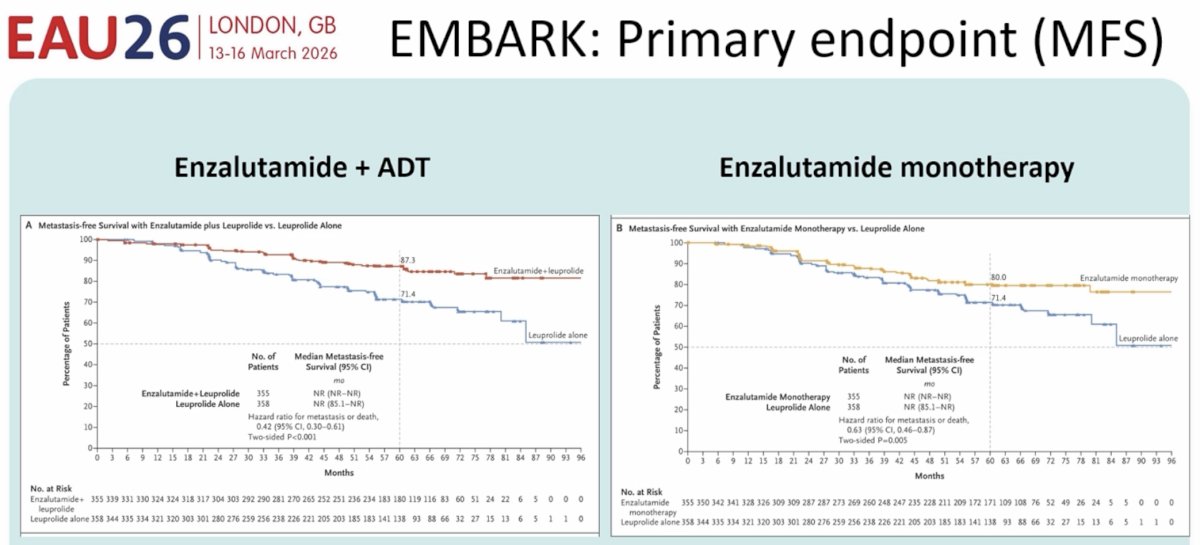
At a median follow-up of 60.7 months, patients in the combination arm of enzalutamide + leuprolide had significantly superior 5-year metastasis free survival rates (87.3% versus 71.4%; HR: 0.42, 95% CI: 0.30–0.61, p<0.001). For the comparison of enzalutamide monotherapy to leuprolide monotherapy, patients in the enzalutamide monotherapy arm had superior 5-year metastasis-free survival (80% versus 71.4%; HR: 0.63, 95% CI: 0.46–0.87, p=0.005).1
Based on these results, enzalutamide gained FDA approval in 2023 in this high-risk, biochemically recurrent, non-metastatic setting, and the EAU guidelines now strongly recommend enzalutamide in such patients.
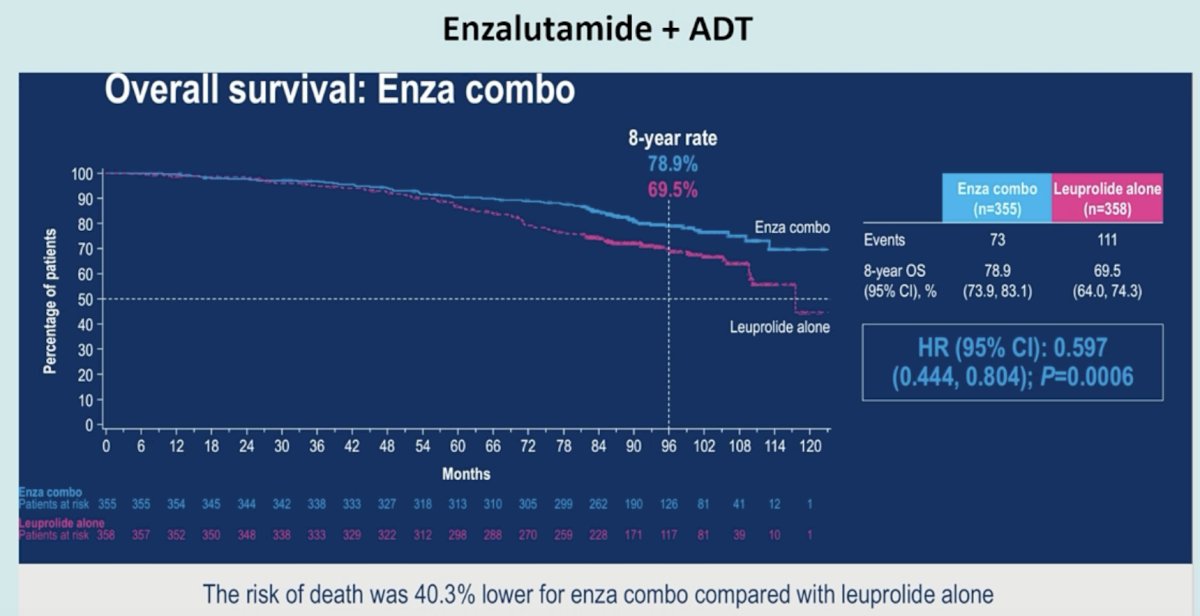
More recently, the overall survival data were presented at ESMO 2025. Compared to leuprolide monotherapy, patients receiving the combination of enzalutamide + leuprolide had significantly improved overall survival (8-year rate: 78.9% versus 69.5%; HR: 0.60, 95% CI: 0.44-0.80, p=0.0006).
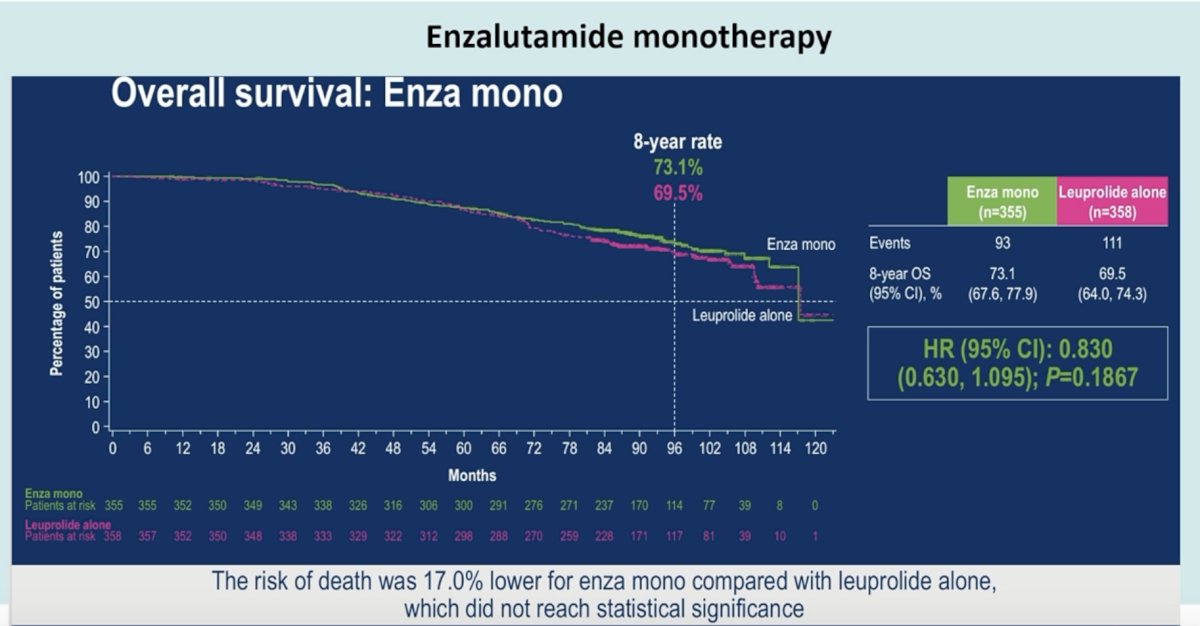
No significant overall survival benefit was observed with enzalutamide monotherapy, versus leuprolide monotherapy (8-year rate: 73.1% versus 69.5%; HR: 0.83, 95% CI: 0.63-1.10, p=0.19).
Overall, enzalutamide monotherapy, compared to leuprolide monotherapy, demonstrated a greater 5-year probability of remaining free from distant metastasis (86.8% vs 81.5%), symptomatic progression (66.6% vs 53.3%), and first symptomatic skeletal event (95.8% vs 91.5%), compared to ADT monotherapy. However, patients receiving enzalutamide monotherapy resumed hormonal therapy sooner after treatment suspension (HR 1.6; p<0.0001) compared to other treatment arms, and breast-related adverse events (gynecomastia, nipple pain, breast pain/tenderness) were more common in patients receiving enzalutamide monotherapy.
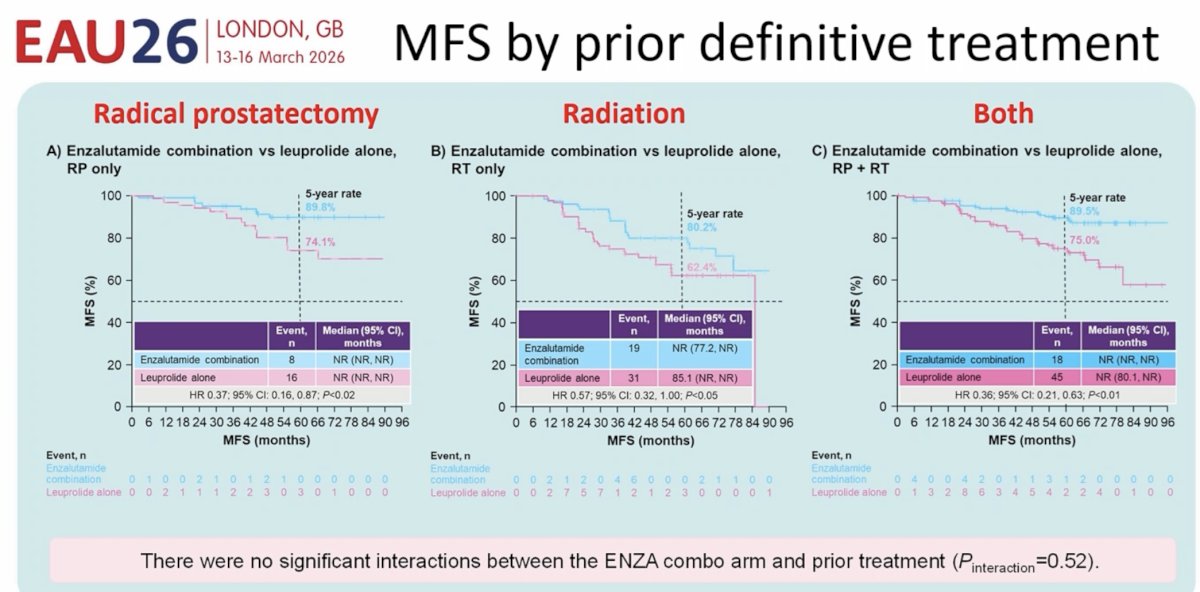
Was there a treatment effect based on prior local therapy received? Subgroup analyses by prior definitive treatment demonstrated that there was no significant interaction between prior definitive therapy and metastasis-free survival benefit with enzalutamide combination.
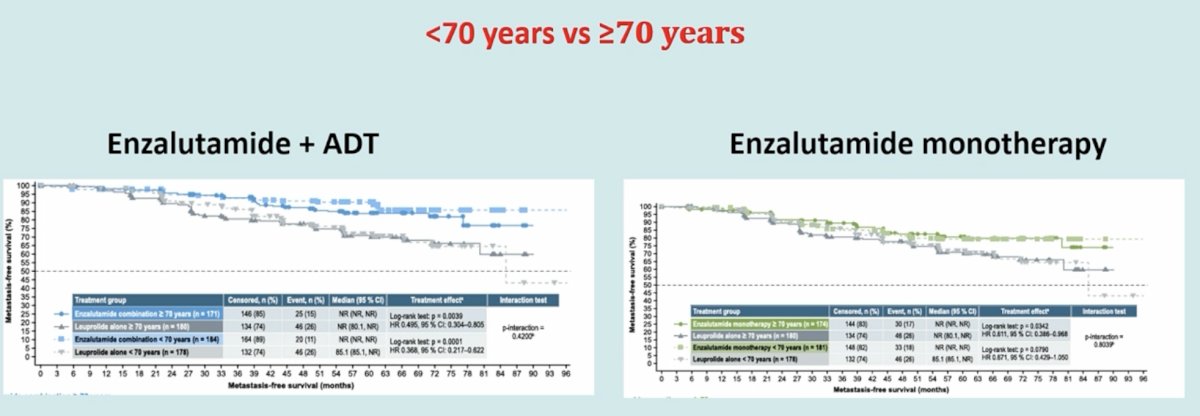
Similarly, the survival benefits were consistent across age strata (<70 years versus ≥70 years).2
What about differences in sexual activity?3 Compared to leuprolide monotherapy, enzalutamide monotherapy was associated delayed (i.e. worsened) time to:
- Interest in sex (8.5 vs 5.6 months)
- Sexual activity extent (5.7 vs 3 months)
- Satisfaction with sex life (11.1 vs 5.4 months)
- Erectile function (5.5 vs 2.9 months).
Notably, there were no meaningful differences in sexual activity between enzalutamide monotherapy and combination therapy.
What was the impact of treatment suspension on health-related quality of life? Treatment suspension occurred in:
- Enzalutamide + ADT: 90%
- Enzalutamide monotherapy: 86%
- ADT: 67%
There were no meaningful changes in any treatment arm after treatment suspension across all assessed patient-reported outcome measures, except for hormonal treatment-related symptoms. The time to clinically meaningful improvements was as follows:
- Enzalutamide + ADT: 12 months after stopping
- Enzalutamide monotherapy: 6 months
- ADT: 9 months
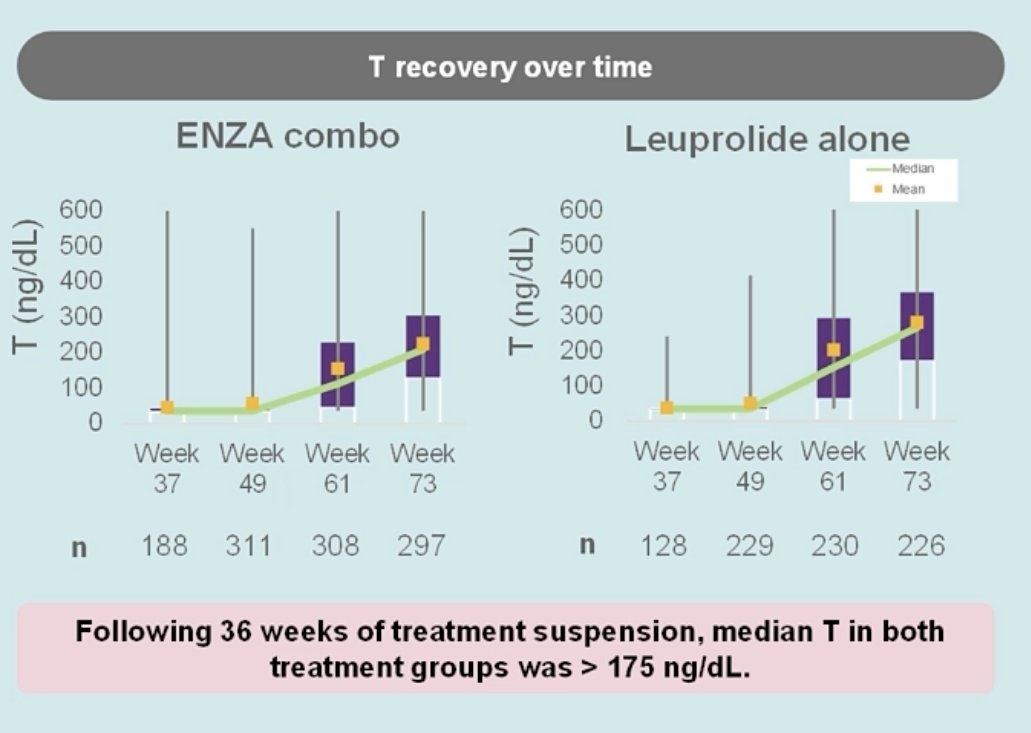
What about testosterone recovery during the treatment suspension period? Following 36 weeks of treatment suspension, the median testosterone in both enzalutamide combination and leuprolide monotherapy arms was>175 ng/dL. Notably, only 4% of patients treated for 9 months with combination enzalutamide + ADT had a PSA <0.2 ng/ml with normal testosterone 3 years after therapy.
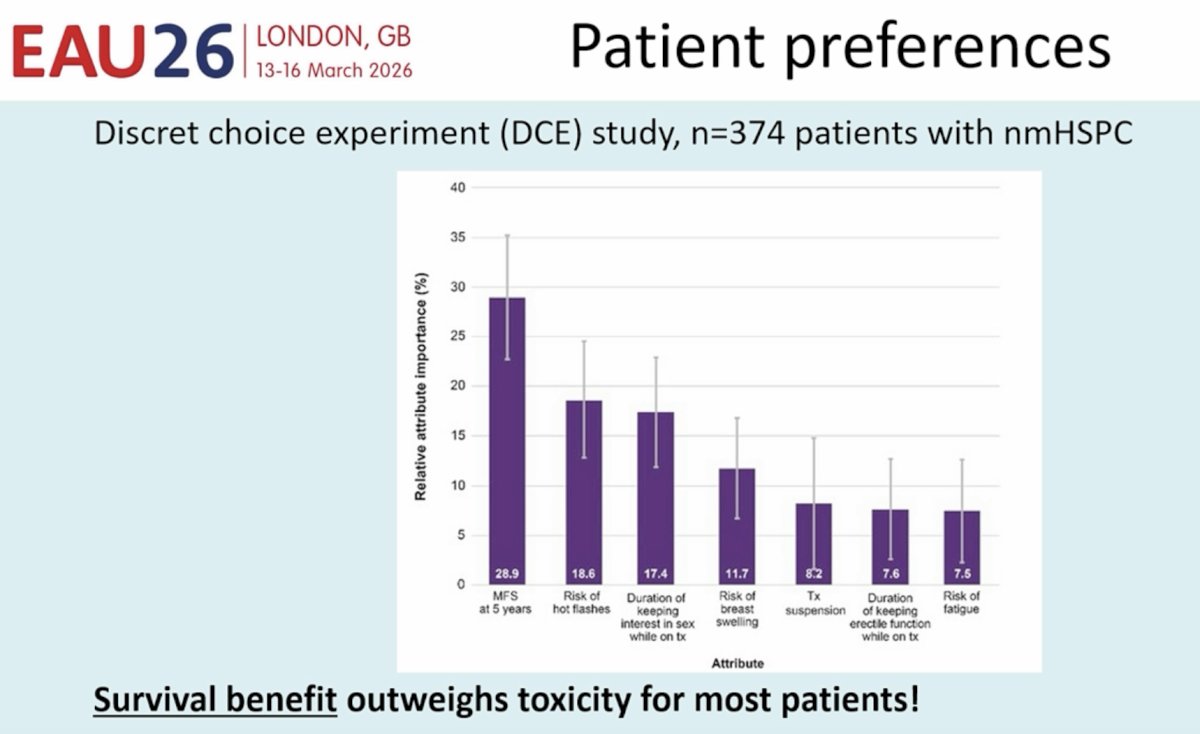
Most importantly, however, what matters most to patients in this setting? Survival or treatment-related toxicity? A study presented by Dr. Neal Shore at ASCO GU 2026 demonstrated that metastasis-free survival at 5 years was the most important factor for such patients when considering therapy (29%), followed by risk of hot flashes (18.6%).
What improvements can we make to the treatment/stratification of biochemically recurrent patients? Dr. Heidegger highlighted that an important, fixable issue is to harmonize the definition of high-risk biochemical recurrence across studies.
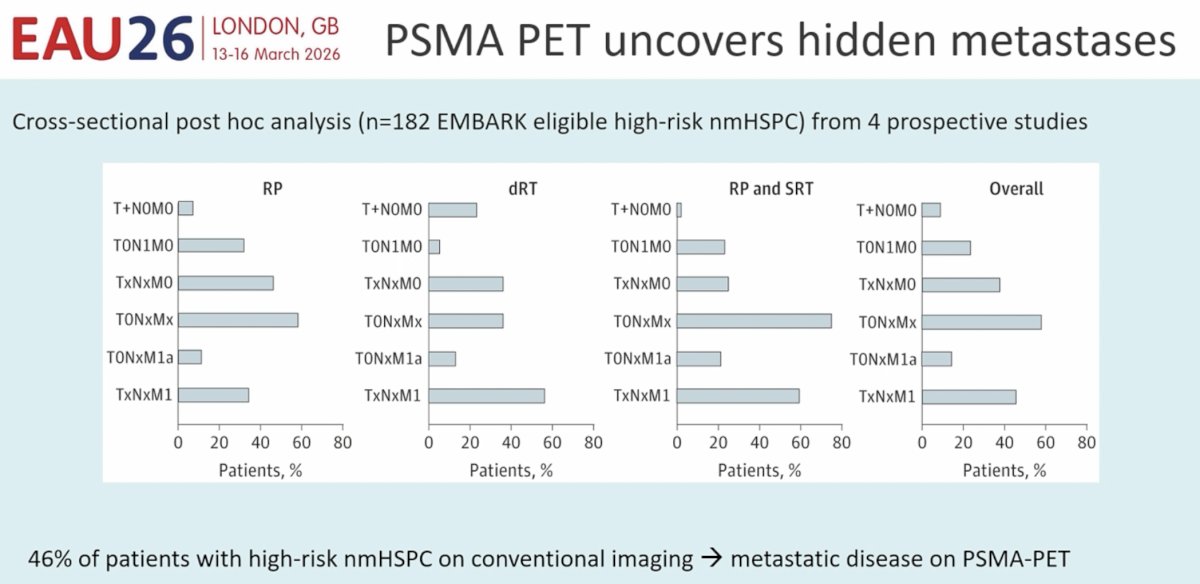
Another important limitation of the literature is the inconsistency of imaging modalities used to stage patients with high-risk biochemical recurrence. The EAU guidelines currently strongly recommend the use of PSMA PET imaging in such patients; however, EMBARK patients were staged using conventional imaging tools.
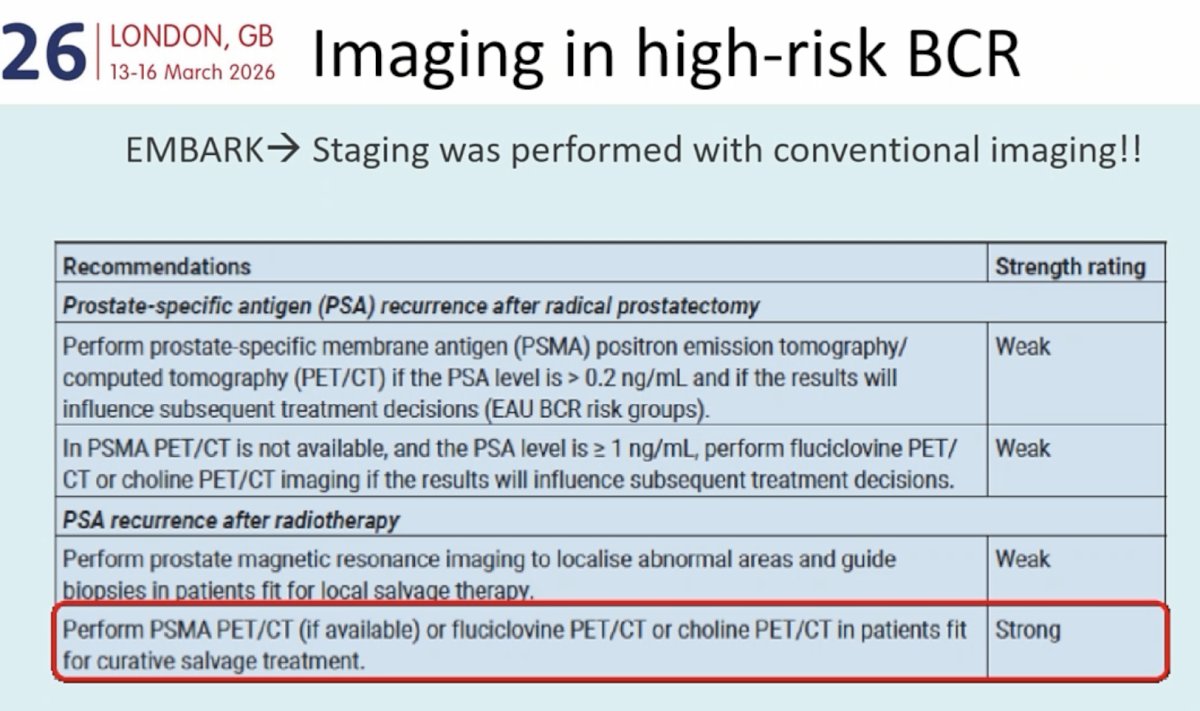
This is important given that 46% of patients with high-risk nmHSPC on conventional imaging will be found to have metastatic disease on PSMA PET.4
Another important issue is the underutilization of commonly available PSA kinetics, such as PSA doubling time, to risk stratify these patients. Morgans et al. estimated that 63% of patients in clinical practice do not have a documented PSA doubling time at biochemical recurrence diagnosis.5 Dr. Heidegger also noted that there is a growing body of evidence supporting the molecular profiling of biochemically recurrent patients. Homologous recombination repair (HRR) gene alterations are associated with more aggressive disease, and genetic tests, such as Decipher and Prolaris, are being increasingly studied and used in this setting, with the goal of identifying patients at the highest risk of disease recurrence and progression.
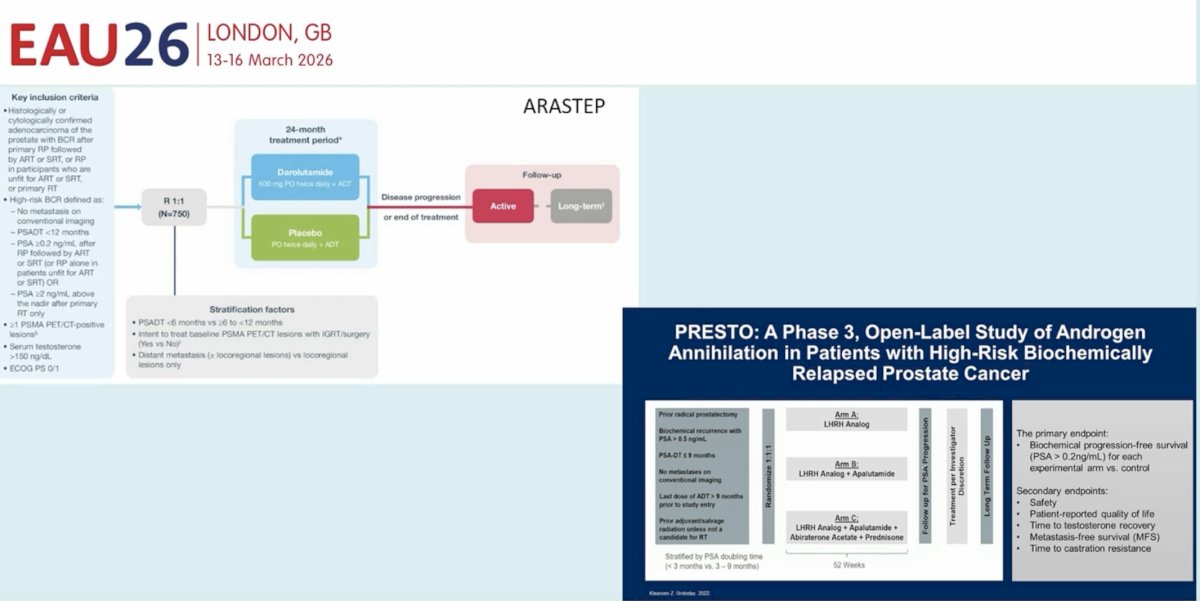
Dr. Heidegger highlighted that there are ongoing studies evaluating whether alternative androgen receptor pathway inhibitors can be used in this setting, including ARASTEP (darolutamide) and PRESTO (apalutamide).
Dr. Heidegger concluded her presentation as follows:
- Enzalutamide +/- ADT is the current standard for high-risk nmHSPC
- Enzalutamide monotherapy shows no overall survival benefit and leads to earlier therapy re-start
- Enzalutamide monotherapy, compared to ADT monotherapy, is associated with delayed time to sexual activity, but shorter time to improvement of hormone-related symptoms after treatment discontinuation
- Future directions are as follows:
- Unified disease definition
- Integration of PSMA PET/CT
- Molecular profiling to identify patients who truly require treatment intensification
Presented by: Isabel Heidegger, MD, PhD, FEBU, Professor, Department of Urology, Medical University Innsbruck, Innsbruck, Austria
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Freedland SJ, de Almeida Luiz M, De Giorgi U, et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med. 2023; 389(16):1453–65.
- Shore N, De Giorgi U, Kalac M, et al. Enzalutamide with or without leuprolide in patients with high-risk biochemically recurrent prostate cancer: EMBARK post hoc analysis by age. Eur J Cancer. 2026;232:116110.
- Freedland SJ, Mulhall JP, Gleave M, et al. Effects of Enzalutamide on the Sexual Activity of Patients with Biochemically Recurrent Prostate Cancer: A Post Hoc Analysis of Patient-reported Outcomes in the EMBARK Study. Eur Urol 2025;87:507–11.
- Holzgreve A, Armstrong WR, Clark KJ, et al. PSMA-PET/CT Findings in Patients With High-Risk Biochemically Recurrent Prostate Cancer With No Metastatic Disease by Conventional Imaging. JAMA Netw Open. 2025;8(1):e2452971.
- Morgans AK, Touya M, El-Chaar N, et al. Does Physician Documentation of Patients’ Prostate-Specific Antigen Doubling Time Affect Treatment Decisions in High-Risk Biochemically Recurrent Prostate Cancer? Clin Genitourin Cancer. 2026;24(2):102496.