(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a urology trials in bladder and prostate cancer session and a presentation by Dr. Christian Engesser discussing DISSECTION 2.0, a multicenter, randomized phase III trial assessing extended pelvic lymph node dissection versus no pelvic lymph node dissection at radical prostatectomy in PSMA PET negative staged men. Pelvic lymph node dissection during radical prostatectomy remains controversial. EAU guidelines neither recommend nor advise against pelvic lymph node dissection, but suggest performing an extended pelvic lymph node dissection if pelvic lymph node dissection is done. While extended pelvic lymph node dissection offers prognostic information, its oncological benefit is uncertain. The DISSECTION 2.0 trial addresses this in PSMA-PET-negative, higher-risk patients who may harbor occult nodal metastases missed by current imaging.
This prospective, randomized multicenter trial (NCT03921996) conducted in 15 Swiss centers, began enrollment in March 2025. It plans to include 400 patients with higher-risk localized prostate cancer (ISUP Grade Group ≥3, or ISUP Grade Group 2 with PSA ≥20 ng/ml) and negative PSMA-PET. Patients are randomized 1:1 to radical prostatectomy with extended pelvic lymph node dissection or radical prostatectomy without pelvic lymph node dissection:
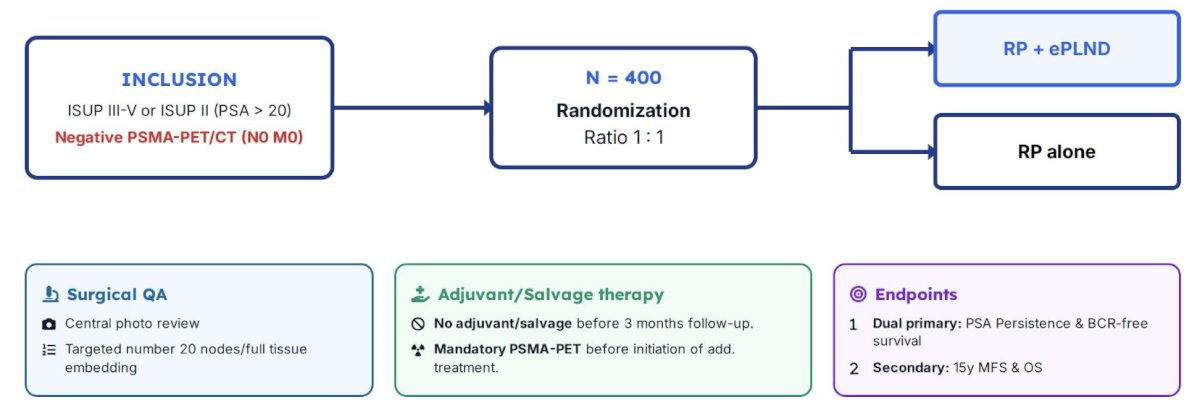
Extended pelvic lymph node dissection extent and quality will be confirmed by standardized intraoperative imaging of the lymph node dissection areas bilaterally. At least 20 lymph nodes must be identified or, if fewer are found, all fatty tissue embedded and examined to ensure diagnostic accuracy. The dual primary endpoints are PSA persistence (PSA ≥ 0.1 ng/ml at 3 months) and biochemical recurrence free survival (PSA > 0.2 ng/ml after 3 months). PSA persistence has the advantage of not being influenced by salvage or adjuvant treatments. The trial is positive if either endpoint is met. A planned interim analysis will assess whether sample size adjustment is needed to achieve meaningful metastasis-free and overall survival outcomes. Treatment algorithms with PSMA guided salvage therapy for PSA persistence and biochemical recurrence free survival aim to reduce bias. Completion is expected in 2027, with PSA persistence results the same year.
Presented by: Christian H. Engesser, Universitatsspital Basel, Basel, Switzerland
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.