(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a PARP inhibitors for prostate cancer session and a state of the art lecture by Dr. David Olmos discussing why germline and somatic alterations in prostate cancer are important. Pathogenic alterations in DNA damage repair genes, causing loss-of-function mutations, have been described in up to 30% of mCRPC patients:
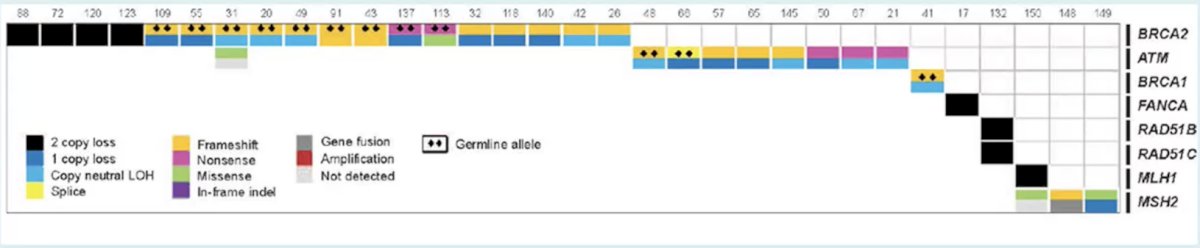
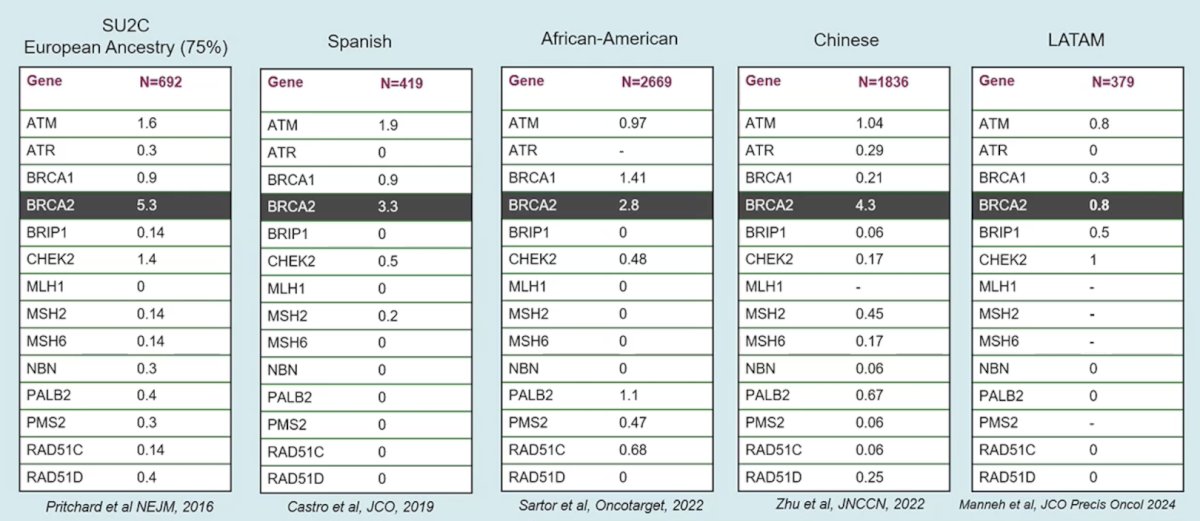
Moreover, defects in different DNA damage repair genes/pathways have been linked to the potential anticancer activity of novel targeted agents, including PARP inhibitors for homologous recombination DNA repair (HRR) deficiency mutations. Deleterious germline BRCA2 mutations have consistently been associated with poor outcomes across prostate cancer stages, including metastatic castration resistant prostate cancer (mCRPC), while the prognostic role of other germline DNA deficiency repair mutations remains unclear. Dr. Olmos provided the following table highlighting the prevalence of germline mutations across multiple populations of patients, which has implications for patients and relatives:
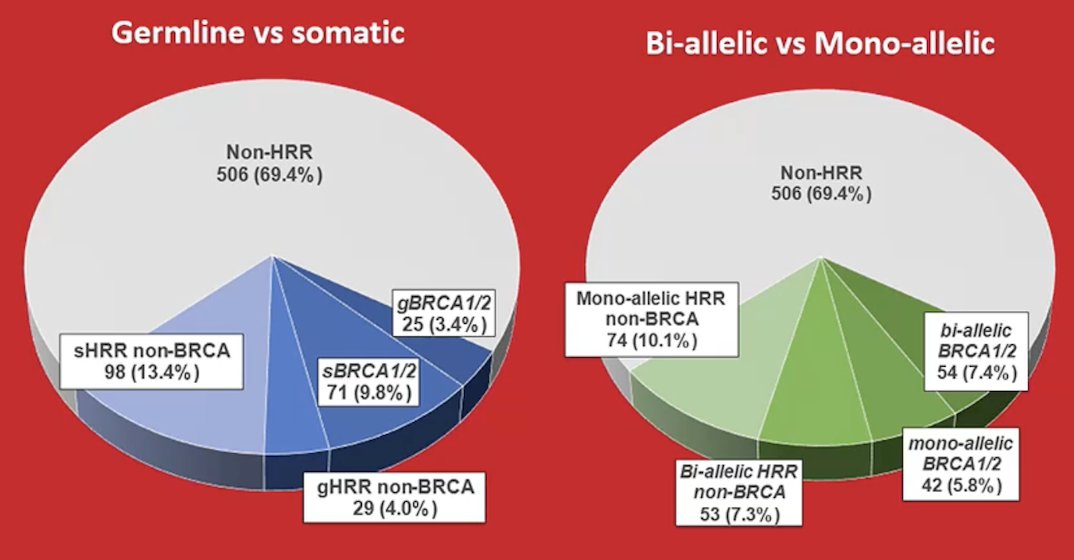
In 2024, Dr. Olmos’ group assessed treatment patterns and outcomes of patients with mCRCP with or without somatic or germline alterations in HRR genes.1 Among 729 mCRPC patients from CAPTURE, 96 (13.2%), 127 (17.4%), and 506 (69.4%) were in the BRCA mutation, HRR non-BRCA mutation, and non-HRR mutation subgroups, respectively. The following shows germline versus somatic and bi-allelic versus mono-allelic mutations in this cohort:
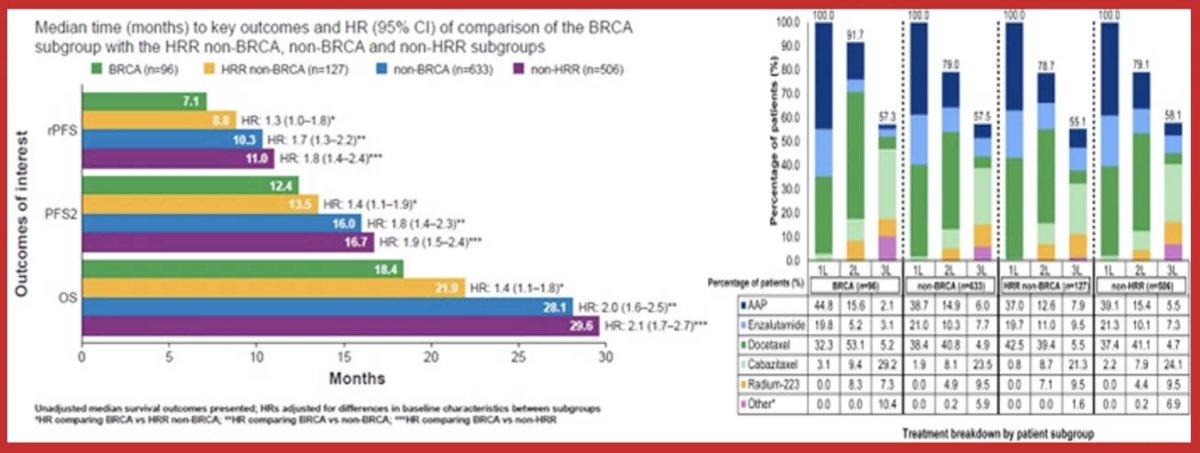
Notably, BRCA patients performed significantly worse for all outcomes compared to non-HRR or non-BRCA patients (p < 0.05), while second progression-free survival and overall survival were significantly shorter for BRCA than HRR non-BRCA patients (p < 0.05):
In 2025, Olmos and colleagues reported outcomes of patients with BRCA1/2 and HRR alterations in high and low volume metastatic hormone-sensitive prostate cancer (mHSPC) [2]. Of 556 patients, 159 (28.6%) had HRR gene alterations: 69 (12.4%) with BRCA and 90 (16.2%) with HRR non-BRCA mutations. mHSPC was synchronous in 451 patients (81.1%) and was classified as high-volume (CHAARTED criteria) in 306 (55%) patients:
![In 2025, Olmos and colleagues reported outcomes of patients with BRCA1/2 and HRR alterations in high and low volume metastatic hormone-sensitive prostate cancer (mHSPC) [2]. Of 556 patients, 159 (28.6%) had HRR gene alterations: 69 (12.4%) with BRCA and 90 (16.2%) with HRR non-BRCA mutations. mHSPC was synchronous in 451 patients (81.1%) and was classified as high-volume (CHAARTED criteria) in 306 (55%) patients:](/images/com-doc-importer/252-eau-2026/eau-2026-state-of-the-art-lecture-why-are-germline-and-somatic-alterations-in-prostate-cancer-important/image-4.jpg)
In both patients with high-volume and low-volume disease, somatic mutations were also more common than germline mutations in the BRCA [27/42 (64.3%) versus 15/42 (35.7%) and 17/27 (63.0%) versus 10/27 (37.0%)] and HRR non-BRCA [31/44 (70.5%) versus 13/44 (29.5%) and 33/46 (71.7%) versus 13/46 (28.3%)] subgroups, respectively:
![In both patients with high-volume and low-volume disease, somatic mutations were also more common than germline mutations in the BRCA [27/42 (64.3%) versus 15/42 (35.7%) and 17/27 (63.0%) versus 10/27 (37.0%)] and HRR non-BRCA [31/44 (70.5%) versus 13/44 (29.5%) and 33/46 (71.7%) versus 13/46 (28.3%)] subgroups, respectively:](/images/com-doc-importer/252-eau-2026/eau-2026-state-of-the-art-lecture-why-are-germline-and-somatic-alterations-in-prostate-cancer-important/image-5.jpg)
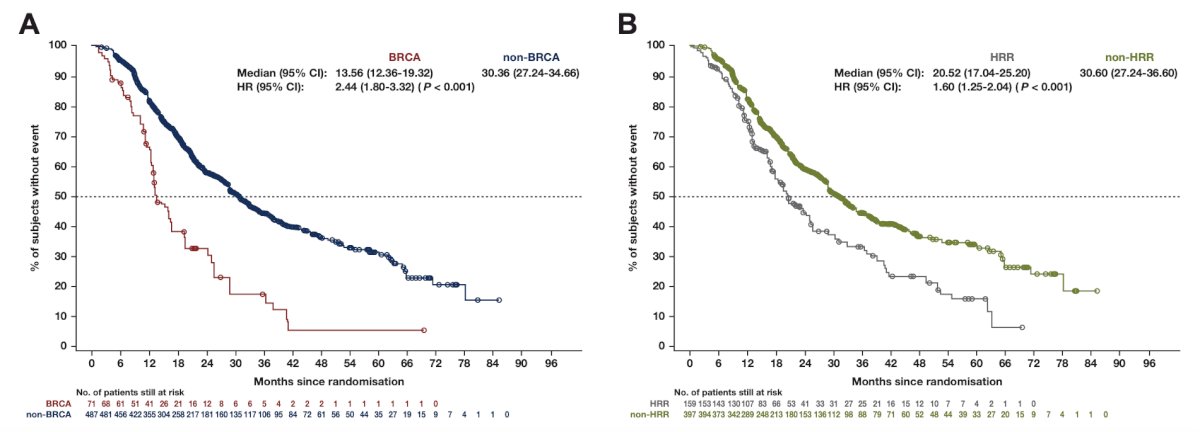
Radiographic progression free survival was significantly shorter in the BRCA than in the non-BRCA subgroup: median 13.6 versus 30.4 months (HR 2.4, 95% CI 1.8-3.3, p < 0.001), and a similar trend was observed when comparing HRR and non-HRR subgroups: median radiographic progression free survival 20.5 versus 30.6 months (HR 1.6, 95% CI 1.3-2.0, p < 0.001):
Overall survival was significantly shorter in the BRCA than in the non-BRCA subgroup: median 26.2 versus 55.1 months (HR 2.7, 95% CI 2.0-3.6, p < 0.001), and a similar trend was observed when comparing HRR and non-HRR subgroups: median overall survival 39.0 versus 55.7 months (HR 1.5, 95% CI 1.1-2.0, p = 0.003):

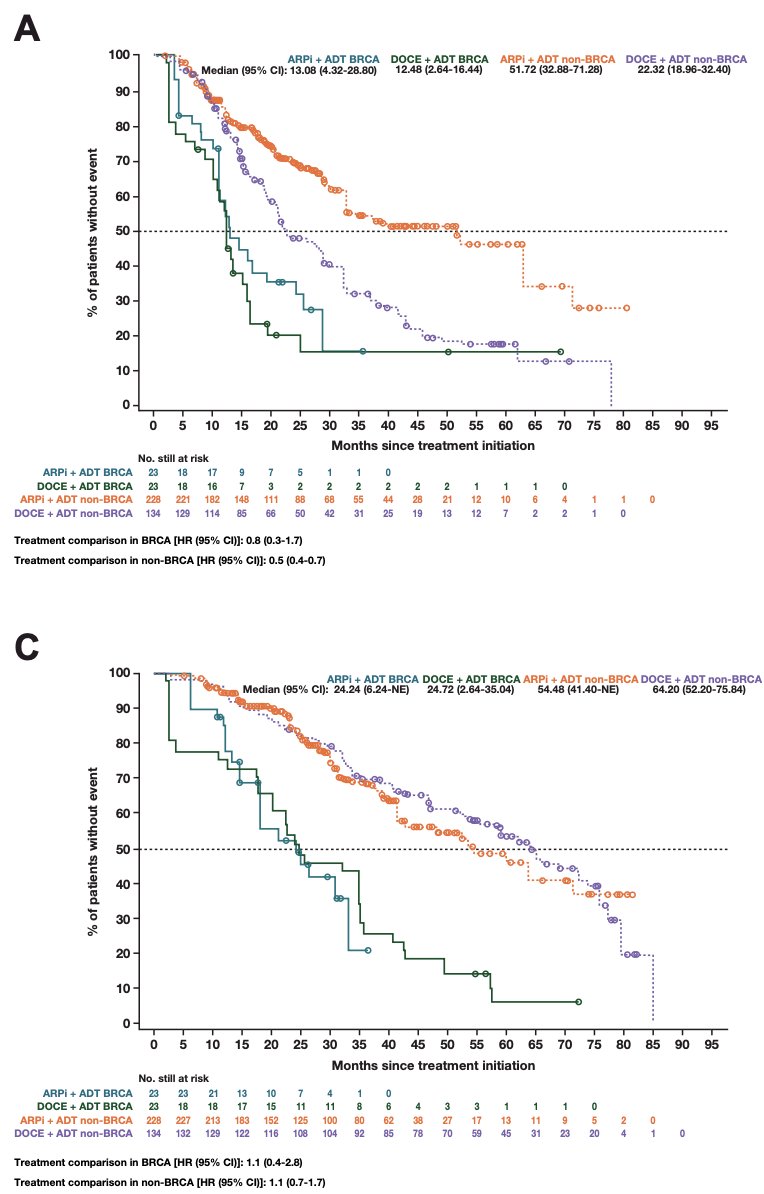
In patients with BRCA alterations, there were no differences in radiographic progression-free survival (13.1 versus 12.5 months) or overall survival (24.2 versus 24.7 months) in patients treated with ADT + androgen receptor pathway inhibitor versus ADT + docetaxel. In contrast, when evaluating the non-BRCA subgroup, a significant benefit in radiographic progression-free survival associated with ADT + androgen receptor pathway inhibitors (HR 0.5, 95% CI 0.4-0.7, p < 0.001) was observed compared to ADT + docetaxel:
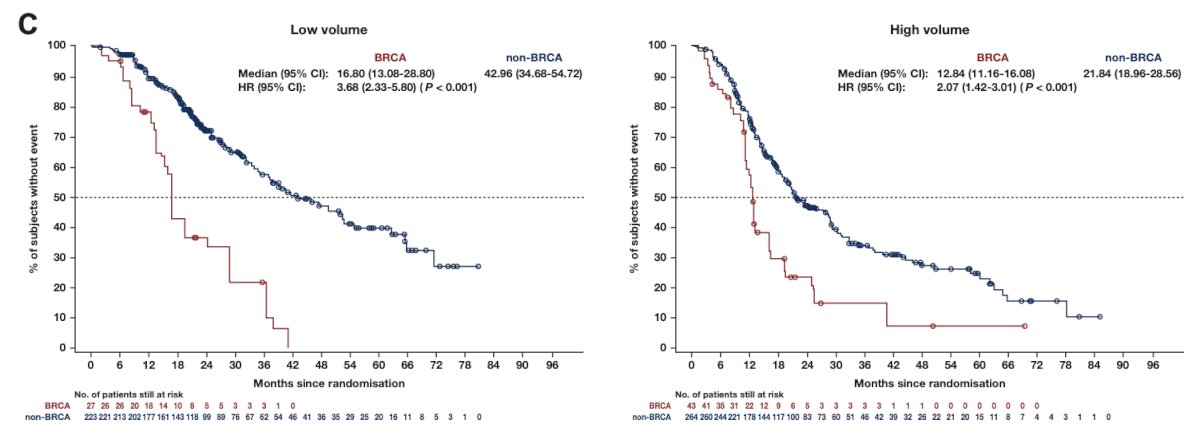
In a comparison of low and high volume patients, those with BRCA mutations versus non-BRCA mutations had worse radiographic progression-free survival, regardless of disease volume:
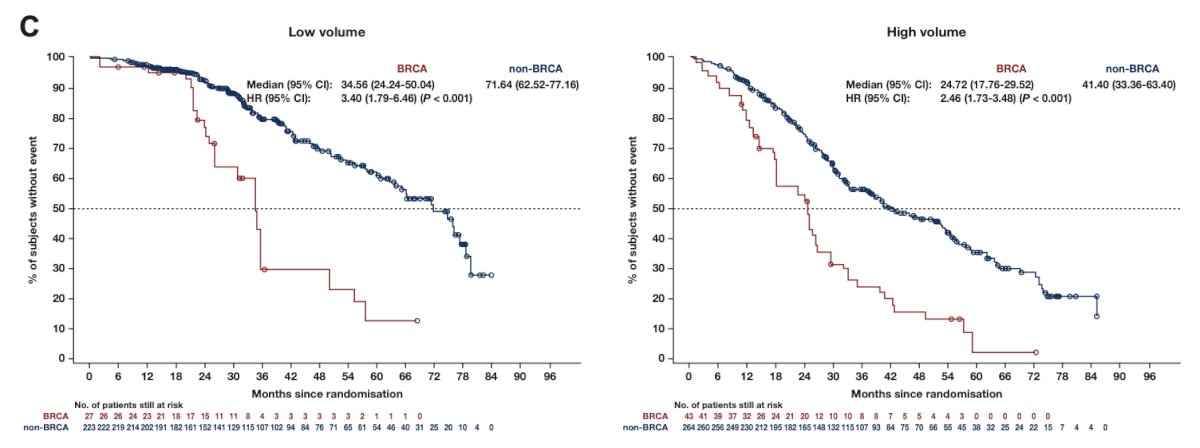
These similar findings were also noted when assessing the outcome of overall survival:
Finally, among 172 patients in the CAPTURE cohort that had non-BRCA HRR alterations, patients with FANCA and CDK12 mutations had comparably poor radiographic progression-free survival similar to BRCA2 mutations, whereas those with ATM, CHEK2, HDAC2, and BRIP1 did not.
Dr. Olmos concluded his presentation discussing why germline and somatic alterations in prostate cancer are important with the following take-home points:
- BRCA2 (more frequent) and BRCA1 (less frequent) mutations have clear prognostic and therapeutic relevance in advanced prostate cancer, regardless of whether they are germline or somatic. Germline mutations additionally carry important implications for family health
- In advanced disease, HRR alterations can exceed 10% across all clinical-risk groups; in BRCA1/2 carriers, disease volume loses prognostic value, as these tumors behave uniformly aggressively
- In localized prostate cancer, the prognostic role of somatic HRR alterations remains undefined, while germline BRCA mutations—particularly BRCA2—are a consistently validated adverse prognostic factor
- For most non-BRCA HRR genes, prognostic significance remains uncertain; specific alterations such as CDK12 (somatic) or FANCA (germline or somatic) may define aggressive disease phenotypes more similar to BRCA1/2
Presented by: David Olmos, MD, PhD, Hospital Universitario 12 de Octubre, Madrid, Spain
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Olmos D, Lorente D, Alameda D, et al. Treatment patterns and outcome in metastatic castration-resistant prostate cancer patients with and without somatic or germline alterations in homologous recombination repair genes. Ann Oncol. 2024 May;35(5):458-472.
- Olmos D, Lorente D, Jambrina A, et al. BRCA1/2 and homologous recombination repair alterations in high- and low-volume metastatic hormone-sensitive prostate cancer: prevalence and impact on outcomes. Ann Oncol. 2025 Oct;36(10):1190-1202.