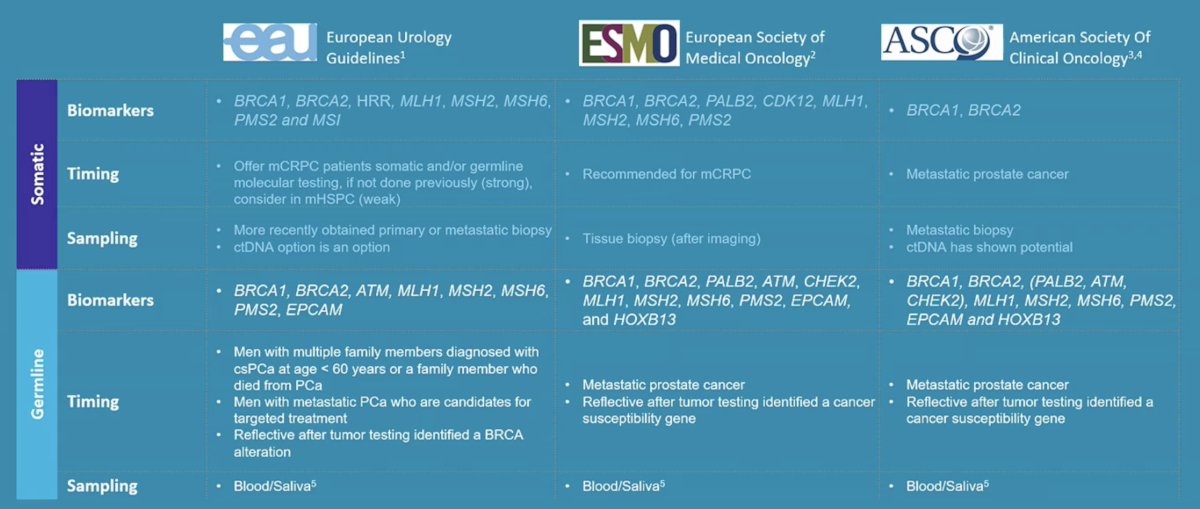
(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a PARP inhibitors for prostate cancer session and a presentation by Dr. Niven Mehra discussing how to optimize germline and somatic testing in prostate cancer. Somatic mutations are acquired and can be found through tumors (clonal) or in a portion of tumor cells (subclonal). The gold standard is detection in tumor tissue, but somatic mutations can also be detected with ctDNA testing. Germline mutations are inherited mutations that are passed on from parents to offspring and are present in every cell. There are validated assays for detecting mutations in blood samples, and germline mutations can also be suspected by tumor tissue and ctDNA testing. As follows are the current oncological testing guidelines from the EAU, ESMO, and ASCO:
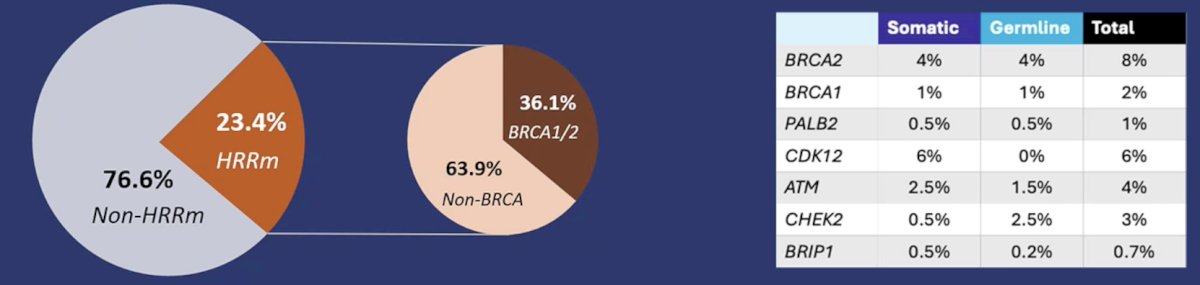
HRR mutations are commonly of germline origin, with several real world studies suggesting a 23-44% probability of an HRR alteration to be of germline origin:1
The following summarizes recommendations for germline and somatic testing in localized and metastatic disease:
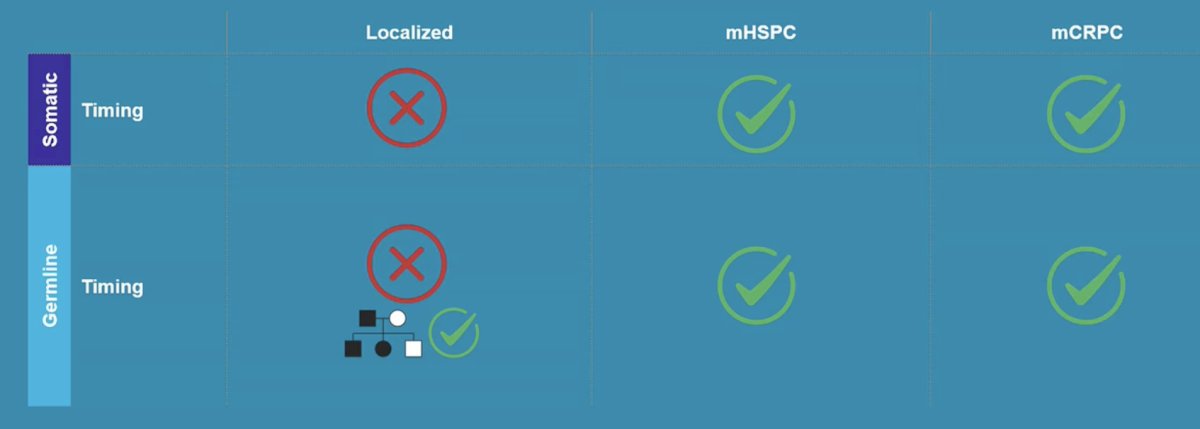
International guidelines do not recommend family history-based germline testing in metastatic prostate cancer; reflective testing is still used in some national and local guidelines. Unfortunately, this results in an under-referral for germline testing, with ~33% of germline variants being missed, including ~42% of high risk variants (ie. BRCA1/2, PALB2). Dr. Mehra notes that broad tumor next generation sequencing panels already interrogate most cancer predisposition genes, thus tumor sequencing can serve as a first line screen for potential germline variants. This tumor first strategy may improve the detection of hereditary cancer risk, which streamlines testing pathways.
Tumor only sequencing misses approximately 10-20% of pathogenic germline variants, with most discordance caused by technical and bioinformatics factors (80%) rather than tumor biology (20%):
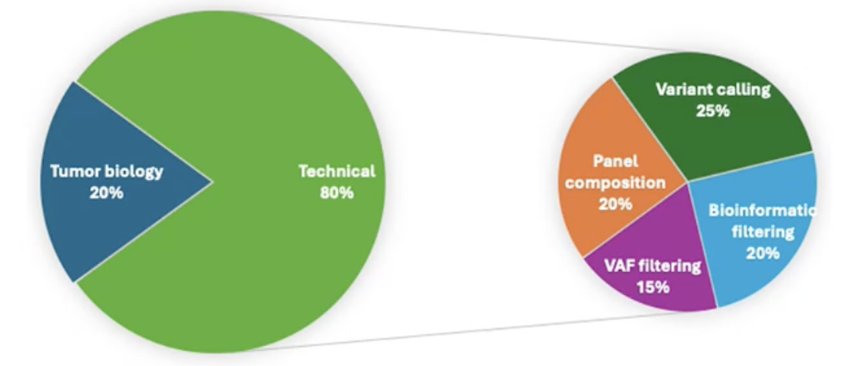
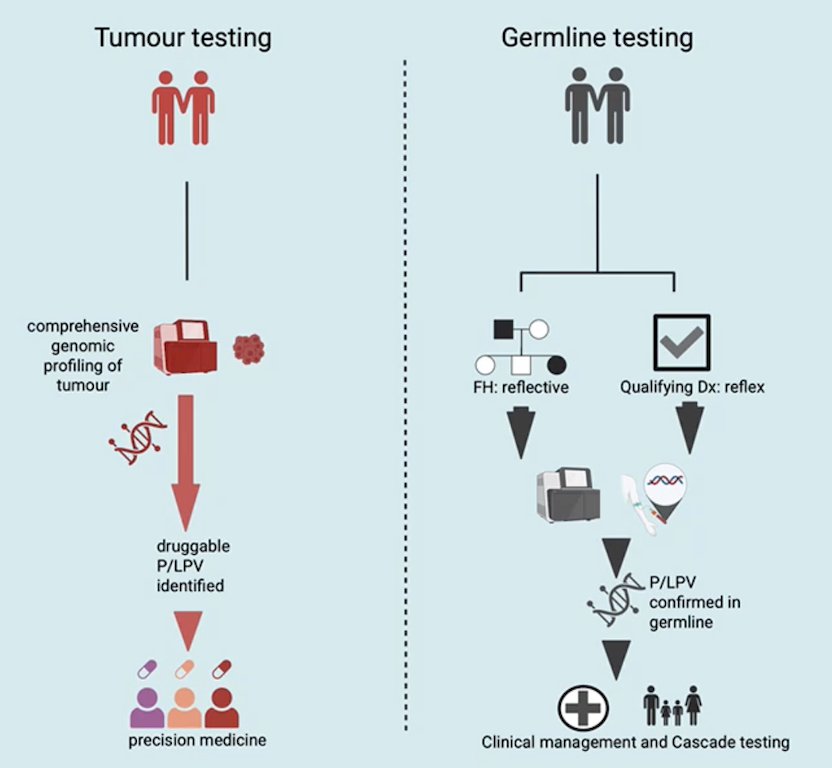
Of note, adaption of tumor-only sequencing pipelines and panels could reduce false-negative pathogenic germline variants to +/- 1-2%, but more prospective data with comprehensive panels are needed. The following outlines two complementary pathways for HRR testing, tumor and germline pathways:
Dr. Mehra concluded his presentation discussing how to optimize germline and somatic testing in prostate cancer with the following take-home points:
- Tumor genomic testing should be performed in metastatic prostate cancer
- Germline testing remains essential when guideline criteria are met
- While cost and resource effective, tumor only sequencing should not (yet) replace dedicated germline testing
- Tumor findings should trigger confirmatory germline testing
- False negative germline variants remain a concern
Presented by: Niven Mehra, MD, PhD, Radboud University Medical Center, Nijmegen, The Netherlands
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References: