(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a PARP inhibitors for prostate cancer session and a presentation by Dr. Himisha Beltran discussing how to read a genetic report for clinical practice. Dr. Beltran started her presentation by highlighting what a sample ctDNA report looks like:
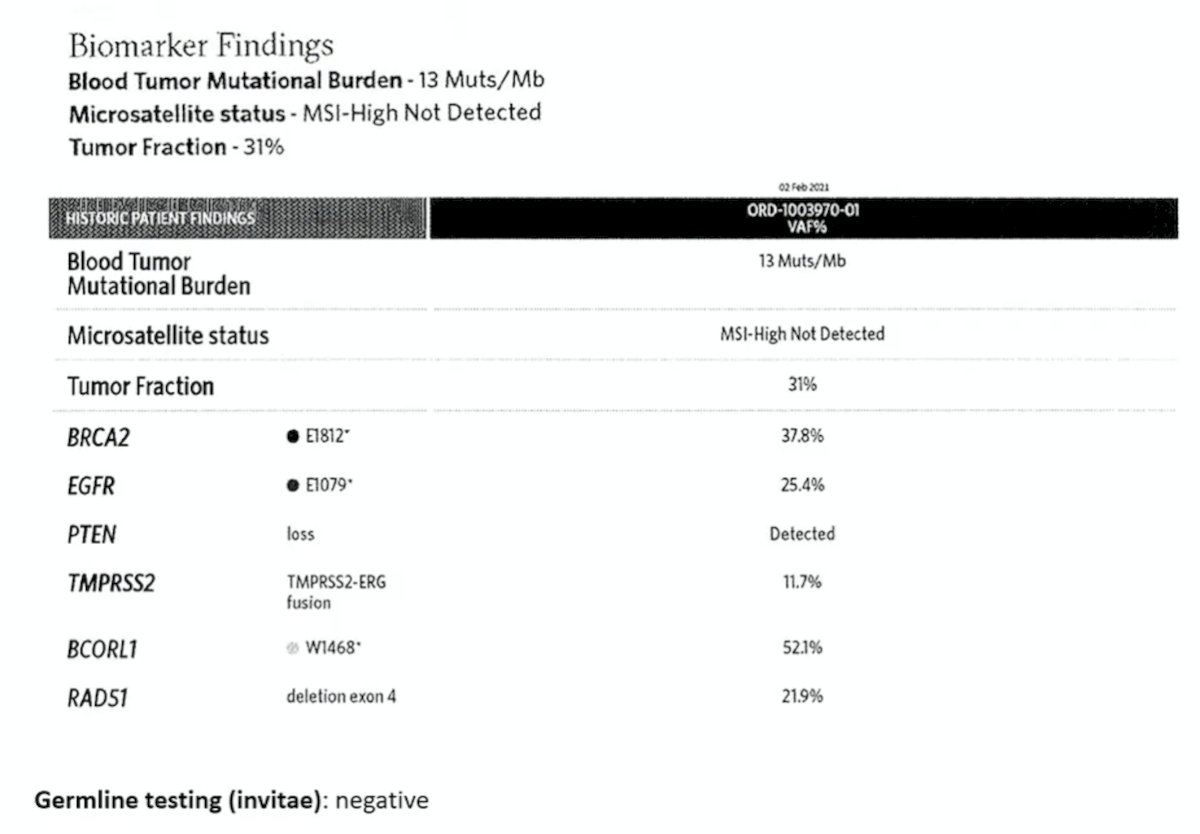
What we should be looking for in a genomic report is the tumor fraction (ie, tumor cellularity in the tissue). This is the proportion of cell-free DNA (cfDNA) coming from the cancer, often relying on aneuploidy, variant allele frequency, fragment length prediction, and CHIP predictions. ctDNA fraction varies widely in mCRPC studies (median 3-10%), and if the tumor fraction is very low (<1-2%), a lack of mutations may be due to a lack of ability to detect mutations. Thus, we should check ctDNA when patients are progressing on therapy. Dr. Beltran notes that baseline total cfDNA and ctDNA fractions are independently prognostic in mCRPC trials, with early declines in ctDNA fraction therapy associated with response. We should also be looking at tumor mutational burden and MSI-high status to assess whether a patient is a candidate for immunotherapy. There is pan-cancer approval for tumor tissue tumor mutational burden >= 10, which ctDNA often overestimates, with a higher cutoff of >20 suggested. Third, we should also be looking for mutations and copy number alterations. Variant allele frequency is a metric of the proportion of variant relative to total reads at a genomic locus, which should be interpreted in the context of tumor cellularity of the ctDNA fraction. A very low variant allele frequency may suggest a subclonal event (less likely to be a driver or targetable), and a variant allele frequency of 50% may suggest a germline variant, however a variant allele frequency of 15% may also be germline if the tumor content is 30%.
Should we be looking for bi-allelic loss? Dr. Beltran notes that BRCA2 loss of function occurs via loss of both alleles. Bi-allelic inactivation can occur via a mutation + a loss of heterozygosity or by homozygous deletion. If a pathogenic mutation is found (either germline or somatic), do we need to confirm the second allele is also lost? Of note, this is more challenging to detect in ctDNA. Generally, bi-allelic loss is not linked to drug approval, but it may identify the best responders.
Dr. Beltran then provided a case study of a patient who had his primary tumor sequenced from Oncopanel (targeted exome test, with approximately 500 genes in the tumor only):
- Tumor Mutational Burden/Megabase: 3.802
- Mismatch Repair Status: Proficient (MMR-P / MSS)
- Mutations:
- Tier 1 variants: BRCA2 c.5434G>T (p.E1812*), exon 11 - in 11% of 245 reads --This variant is a nonsense mutation and is predicted to lead to loss of function.
- Tier 2 variants: None identified
- Structural Variants:
- Tier 1 variants: None identified
- Tier 2 variants: Rearrangement - ERG intron 1 (chr21:39965305): TMPRSS2 intron 1 (chr21:42876023)
- Copy Number Variants:
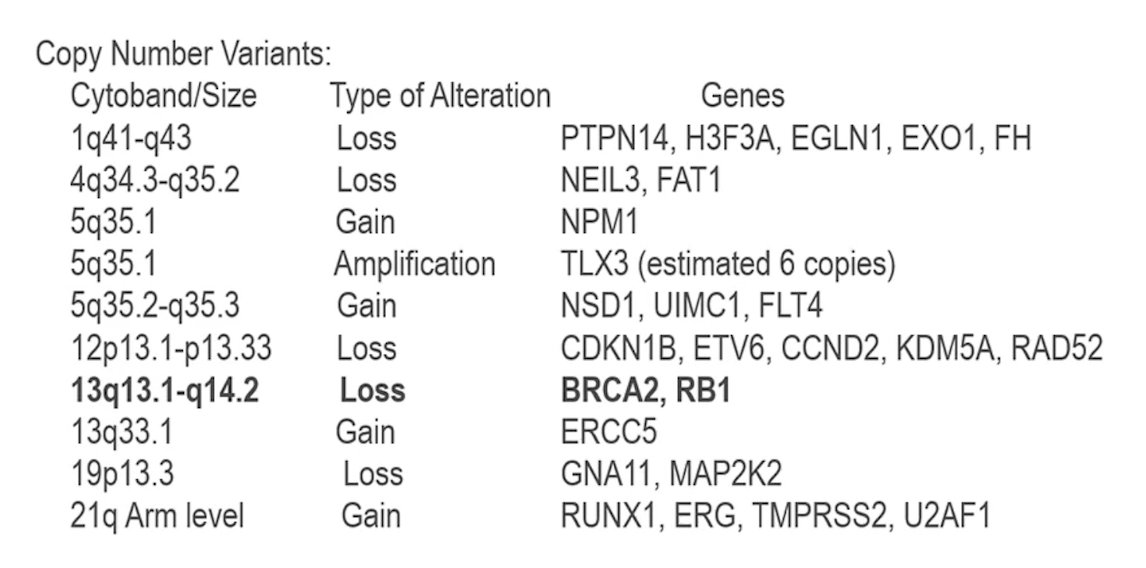
This report identified a single copy deletion of BRCA2 at 13a13.1, and taken together with the loss-of-function mutation, this event is predicted to contribute to biallelic inactivation of BRCA2. This patient was subsequently started on olaparib, with his PSA going from 703 ng/mL to 111 ng/mL, with ctDNA counts improving on therapy, as well as a clinical improvement (ie, energy, pain). However, 6 months later, his PSA increased to 285.40 ng/mL, and he re-presented with new spinal cord compression. Repeat ctDNA showing 16 BRCA2 mutations:
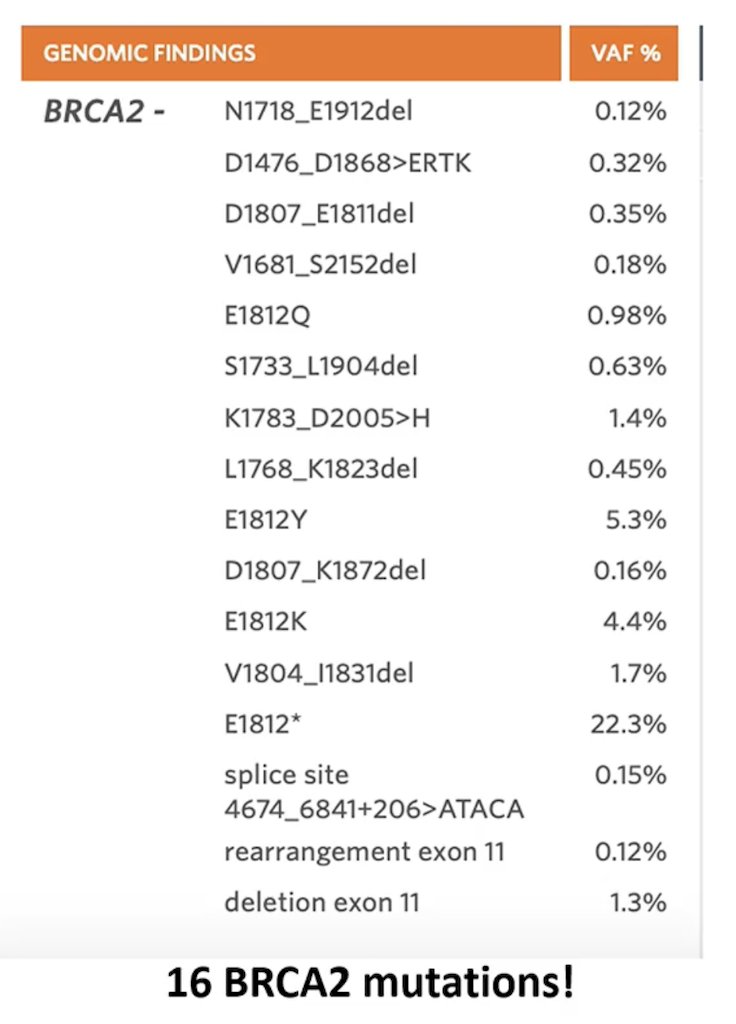
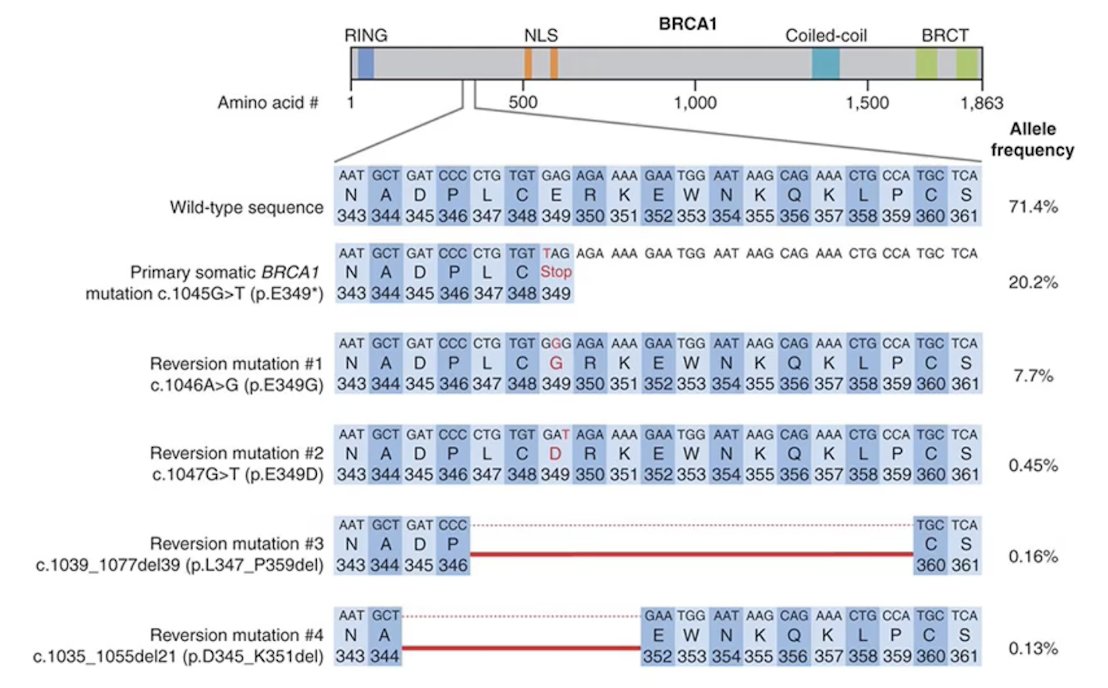
Reversion mutations are secondary mutations, often small deletions, in a mutant BRCA1/2 allele that convert the initial frameshift mutation into an in-frame internal deletion that produces a partly functional protein product:1
Dr. Beltran concluded her presentation discussing how to read a genetic report for clinical practice with the following take-home points:
- What to look for in a genomic report:
- Tumor cellularity (tissue) or ctDNA fraction (blood)
- Prognostic
- Helps interpret a test’s ability to detect alterations (especially copy number), and the interpretation of variant allele frequency
- Tumor mutational burden (tissue versus blood) and MSI status
- Mutations (and variant allele frequency) and copy number
- Tumor cellularity (tissue) or ctDNA fraction (blood)
- Under investigation: mutational signatures, functional readouts, minimal residual disease platforms, fragmentomics, and epigenetics
Presented by: Himisha Beltran, MD, Medical Oncologist, Dana Farber Cancer Institute, Associate Professor of Medicine, Harvard Medical School, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
Reference:
- Lin KK, Harrell MI, Oza AM, et al. BRCA reversion mutations in circulating tumor DNA predict primary and acquires resistance to the PARP inhibitor rucaparib in high-grade ovarian carcinoma. Cancer Discov. 2019 Feb;9(2):210-219.