(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a PARP inhibitors for prostate cancer session and a presentation by Dr. Inge Van Oort discussing the indications of genetic testing in prostate cancer. Patient care typically starts with the urologists at the time of diagnosis, which leads to a biopsy, appropriate staging, and subsequently treatment decisions.
However, Dr. Van Oort notes that we also need to know when molecular information is needed. Germline gene variants are present in all cells and are inheritable, whereas somatic gene variants are not inherited and are only present in specific cells or tumors. Germline testing can identify hereditary cancer, which leads to implications for family members, cascade testing for relatives, and starting surveillance and prevention measures:
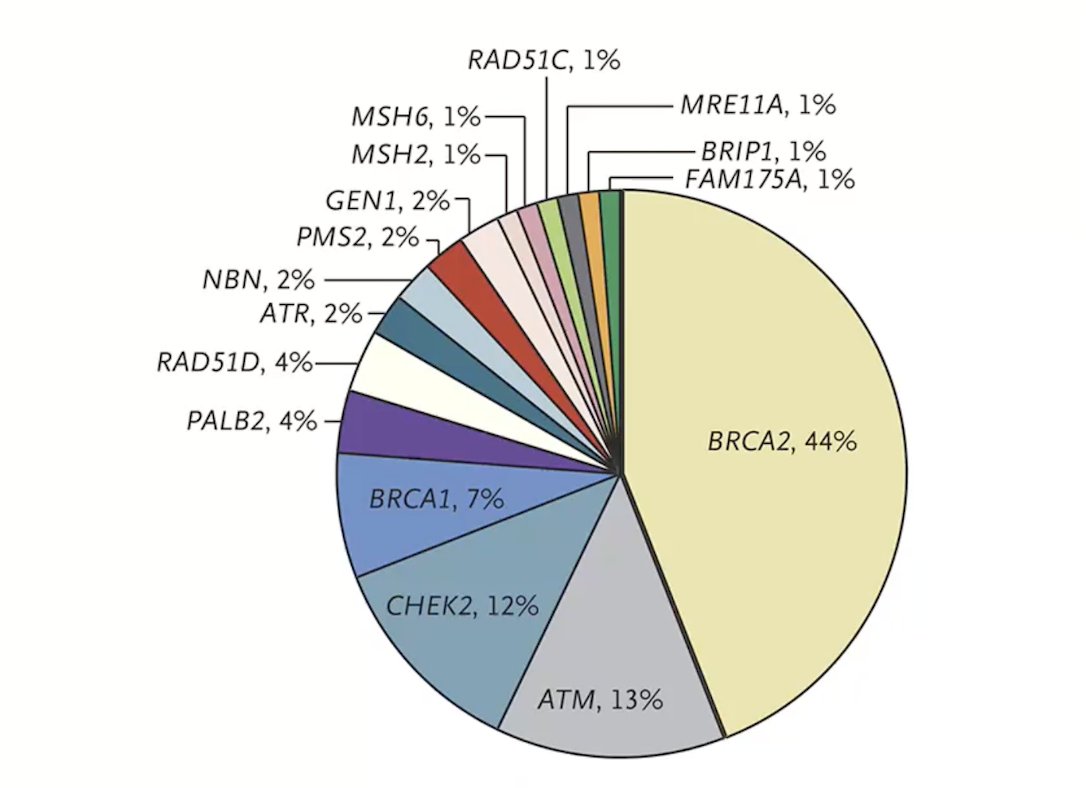
Genetic testing in prostate cancer matters because these results can be used to guide targeted therapy and may influence treatment sequencing. Importantly, we know that 8-15% of metastatic prostate cancers carry germline mutations:1
Dr. Van Oort emphasized that two developments changed practice, making testing clinically relevant:
- Identification of germline mutations in metastatic prostate cancer
- Development of targeted therapies exploiting DNA repair defects
Thus, genetic testing is clinically actionable.
To move from genetic testing to targeted therapy, tumor biology leads to DNA repair defects, which leads to genetic testing and subsequently targeted therapy. Examples include HRR defects leading to treatment with PARP inhibitors, and MMR deficiency leading to treatment with immunotherapy. Currently, the guidelines recommend the following for whom to test, with indications continuing to expand:
- EAU: metastatic prostate cancer + hereditary risk signals
- ESMO: metastatic prostate cancer
- NCCN: metastatic + N+ + high-risk localized prostate cancer
Dr. Van Oort notes that the EAU guidelines have several recommendations for somatic and germline testing, starting with metastatic hormone-sensitive prostate cancer (mHSPC), which states to “test patients for somatic or germline HRR aberrations, since they may qualify for the addition of niraparib to ADT + abiraterone in patients with M1 disease” (Strength: Weak). For metastatic castration resistant prostate cancer (mCRPC) patients, the guidelines state to “offer mCRPC patients somatic and/or germline molecular testing, as well as testing for mismatch repair deficiencies or microsatellite instability, if not done previously.” (Strength: Strong). Specific to germline testing, the guidelines offer 3 statements:
- Advise germline testing in patients with multiple family members diagnosed with prostate cancer at age < 60 years of age or a family member who died from prostate cancer < 60 years of age. (Strength: Weak)
- Offer germline testing in patients with a family history of high-risk germline mutations or a family history of multiple cancers on the same side of the family. (Strength: Strong)
- Offer germline testing to patients with BRCA mutations on somatic testing. (Strength: Strong)
What is also new in the EAU guidelines is that genetic counseling is required prior to germline testing. This recommendation has several implications, including that as testing indications expand, genetic services have limited capacity, and testing often occurs late. How do we integrate genetic testing into routine prostate cancer care? Dr. Van Oort emphasized that one solution could be mainstreaming, whereby counseling occurs at the time of testing by the treating physician + a targeted referral. Testing may be initiated by the urologist, oncologist, or trained nurse, instead of a referral to a geneticist first.
To assess whether mainstreaming is safe for patients, Dr. Van Oort’s group performed a prospective study of 15 patients comprising 767 patients to assess the psychosocial impact of genetic discussions.2 This study found that 5-8% of patients had clinically relevant anxiety or depression; however, 90% reported that testing did not increase their distress. Thus, Dr. Van Oort and colleagues concluded that mainstreaming does not negatively impact patient well-being. A second study from their group assessed whether mainstreaming is feasible for clinicians.3 Among 69 health care professionals, each underwent a 45-minute training module. The study found a positive attitude towards mainstreaming, with 94% of participants finding the pathway helpful. They also found that knowledge of genetics increased significantly, and 88% would continue the mainstream pathway. Overall, clinicians feel well prepared for mainstreaming after a short training module.
Dr. Van Oort concluded her presentation discussing the indications of genetic testing in prostate cancer with the following take-home points:
- Genetic testing is now an integral part of prostate cancer care
- Testing indications are expanding
- The EAU recommends testing in metastatic disease
- Implementation, not the indication, is now the main challenge
- Mainstreaming can enable earlier and broader testing
Presented by: Inge Van Oort, MD, PhD, Professor, University of Groningen, Groningen, The Netherlands
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Pritchard CC, Mateo J, Walsh MF, et al. Inherited DNA-Repair gene mutations in men with metastatic prostate cancer. N Engl J Med. 2016;375(5):443-453.
- Vlaming M, Bleiker EMA, Schijven G, et al. Experiences of metastatic prostate cancer patients with mainstream genetic testing pathway. Int J Cancer. 2026 Feb;158(4):984-993.
- Vlaming M, Ausems MGEM, Kiemeney LALM, et al. Experience of urologists, oncologists and nurse practitioners with mainstream genetic testing in metastatic prostate cancer. Prostate Cancer Prostatic Dis. 2025 Sep;28(3):789-794.