(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., was host to the Hormone sensitive metastatic prostate cancer: Thematic Session. Dr. Declan Murphy delivered a presentation titled: Other treatment intensification strategies in mHSPC.
Dr. Murphy recapitulated the clinical case of a 60-year-old patient with PSA 56, cT4 disease, Grade Group 5, and high-volume mHSPC. The key question he raised was whether Lu-PSMA radioligand therapy should be added at this stage of the disease, reflecting the growing interest in moving PSMA-targeted therapies earlier in the treatment course.
Dr. Murphy began by highlighting the growing interest in radioligand therapy, an approach that is particularly appealing because it leverages imaging biomarkers to deliver targeted treatment. He noted that strong evidence already exists in the mCRPC setting, primarily from the TheraP and VISION trials, which established the clinical activity of PSMA-targeted radioligand therapy.1,2
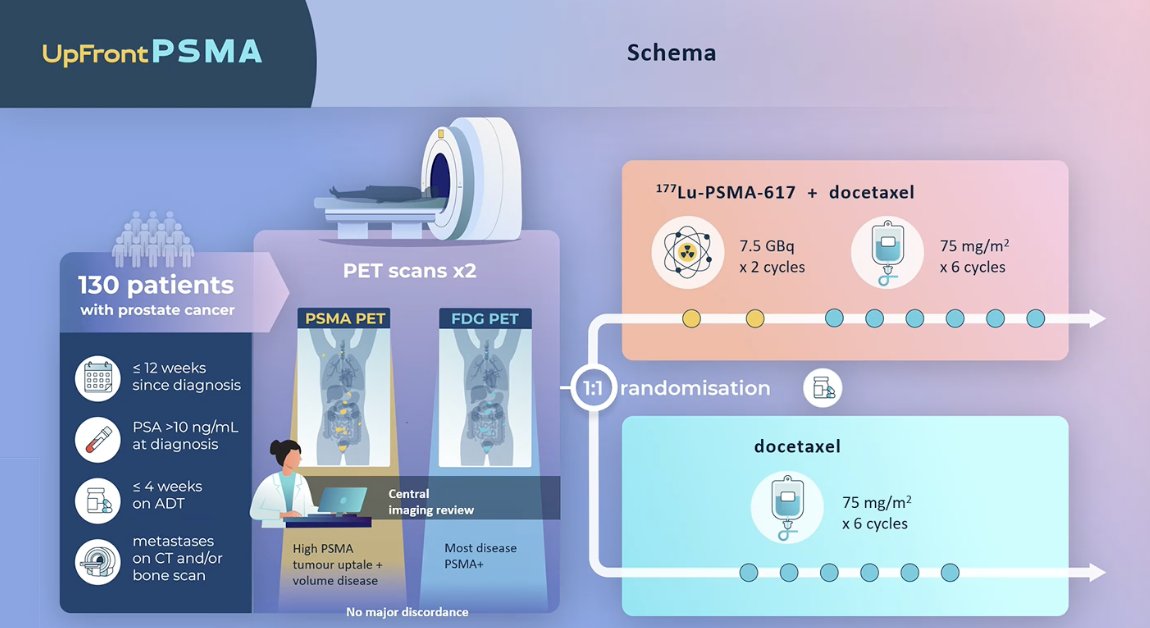
He then discussed the UpFrontPSMA trial, the first study evaluating the use of 177Lu-PSMA-617 earlier in the disease course for patients with newly diagnosed metastatic hormone sensitive prostate cancer. The trial randomized patients to receive sequential 177Lu-PSMA-617 followed by docetaxel versus docetaxel alone, on a backbone of standard ADT. The rationale for the study stems from the current standard of care established by the CHAARTED and STAMPEDE trials, which demonstrated a survival benefit with ADT plus docetaxel in metastatic hormone-sensitive prostate cancer. In this study, patients underwent both PSMA PET and FDG PET imaging prior to enrollment, and those with concordant PSMA-positive disease were randomized to receive two cycles of 177Lu-PSMA-617 before starting six cycles of docetaxel, compared with the standard approach of docetaxel alone.3 The study design is shown below.
Dr. Murphy highlighted that the trial met its primary endpoint. The addition of 177Lu-PSMA-617 to docetaxel was associated with improvements in progression-free survival and radiographic progression-free survival.

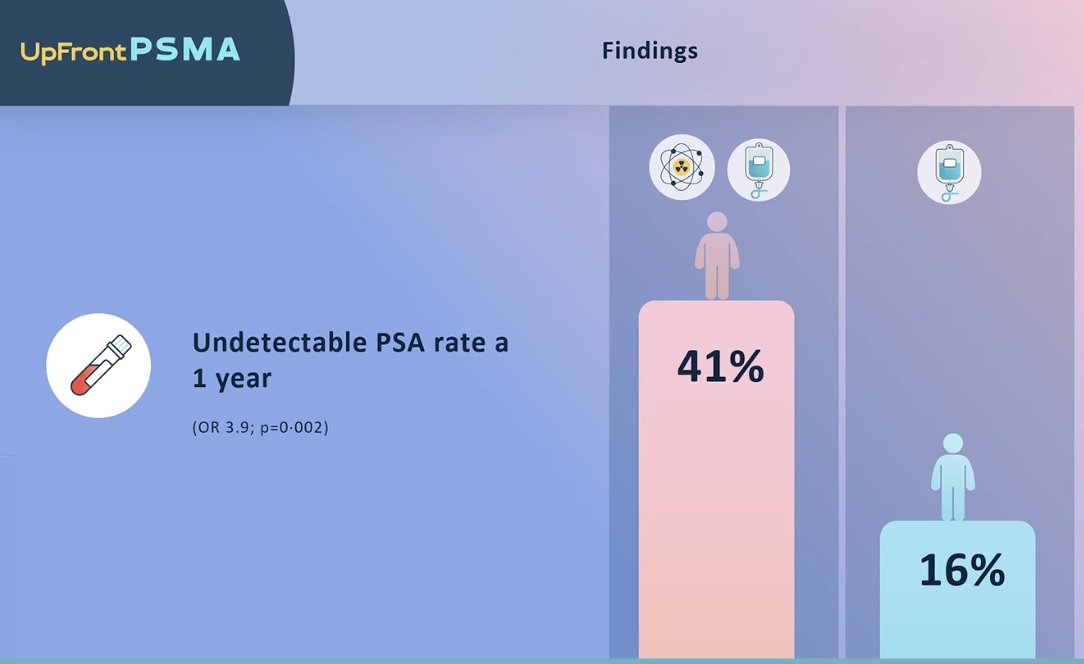
Notably, 41% of patients in the combination arm achieved an undetectable PSA at one year, compared with 16% in the docetaxel-alone arm, as shown in the figure.
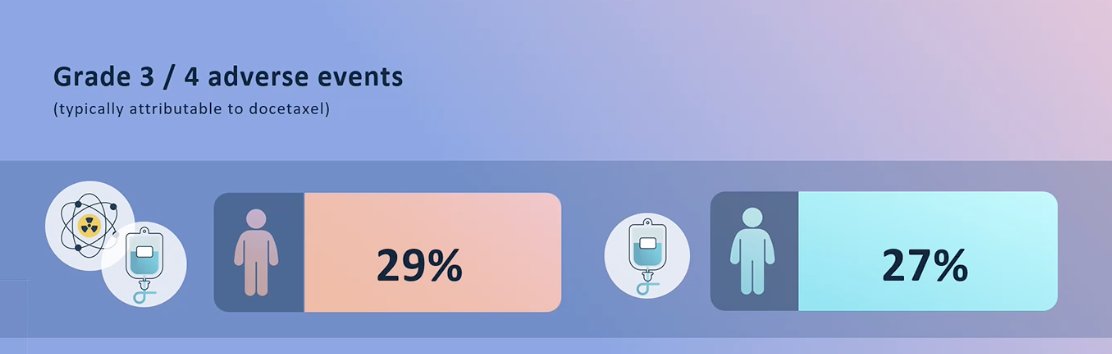
Safety outcomes were comparable between treatment arms, with grade 3–4 adverse events occurring in 29% of patients receiving the combination of 177Lu-PSMA-617 and docetaxel versus 27% with docetaxel alone. Dr. Murphy emphasized that the regimen was overall well tolerated, with most toxicity likely attributable to the backbone therapies, particularly docetaxel and androgen receptor pathway inhibition, rather than the radioligand therapy itself.
He noted that UpFrontPSMA is the first randomized study in mHSPC to demonstrate benefit from the addition of 177Lu-PSMA-617 to standard-of-care therapy. In patients with de novo high-volume mHSPC, treatment with 177Lu-PSMA-617 followed by docetaxel, compared with docetaxel alone, significantly improved the primary endpoint of undetectable PSA at 48 weeks without increasing overall toxicity. These findings suggest that 177Lu-PSMA-617 may have a potential role in the therapeutic management of mHSPC; however, he acknowledged that this was a phase II study and should therefore be considered hypothesis-generating.
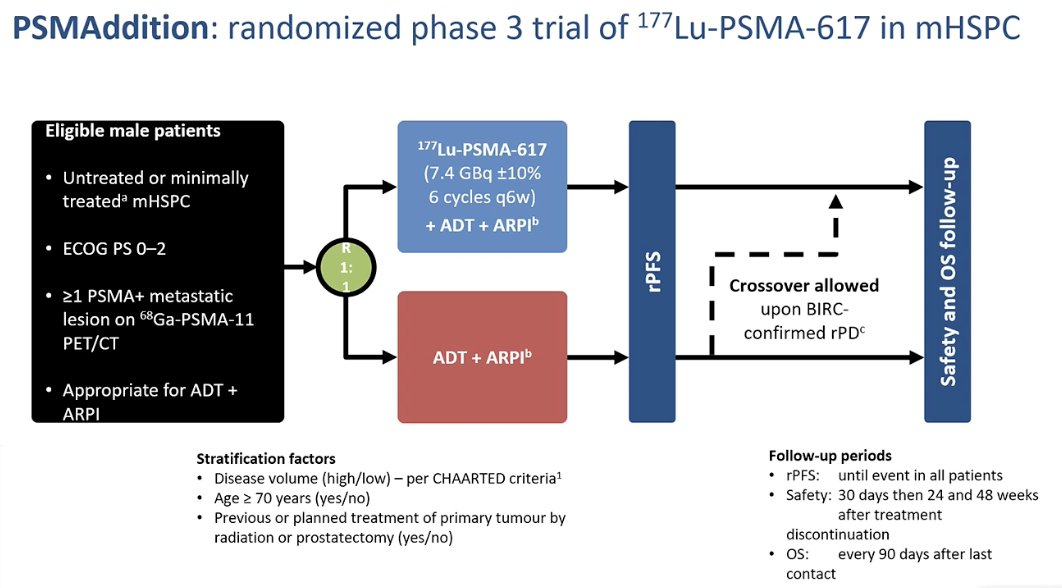
He then discussed the ongoing PSMAddition trial, a randomized phase III study evaluating 177Lu-PSMA-617 in patients with mHSPC. The study enrolls untreated or minimally treated patients with PSMA-positive metastatic disease and randomizes them to receive either 177Lu-PSMA-617 for six cycles in combination with ADT and an ARPI, or standard-of-care ADT plus ARPI alone. Dr. Murphy noted that this population is very similar to that included in UpFrontPSMA; however, the control arm more closely reflects contemporary clinical practice, where ADT plus an ARPI represents a common standard-of-care backbone.4 The study design is presented below.
Dr. Murphy highlighted that the PSMAaddition trial met its primary endpoint, demonstrating a significant improvement in radiographic progression-free survival with the addition of 177Lu-PSMA-617 to ADT plus ARPI. However, at the time of the interim analysis, overall survival remained immature and had not reached statistical significance.
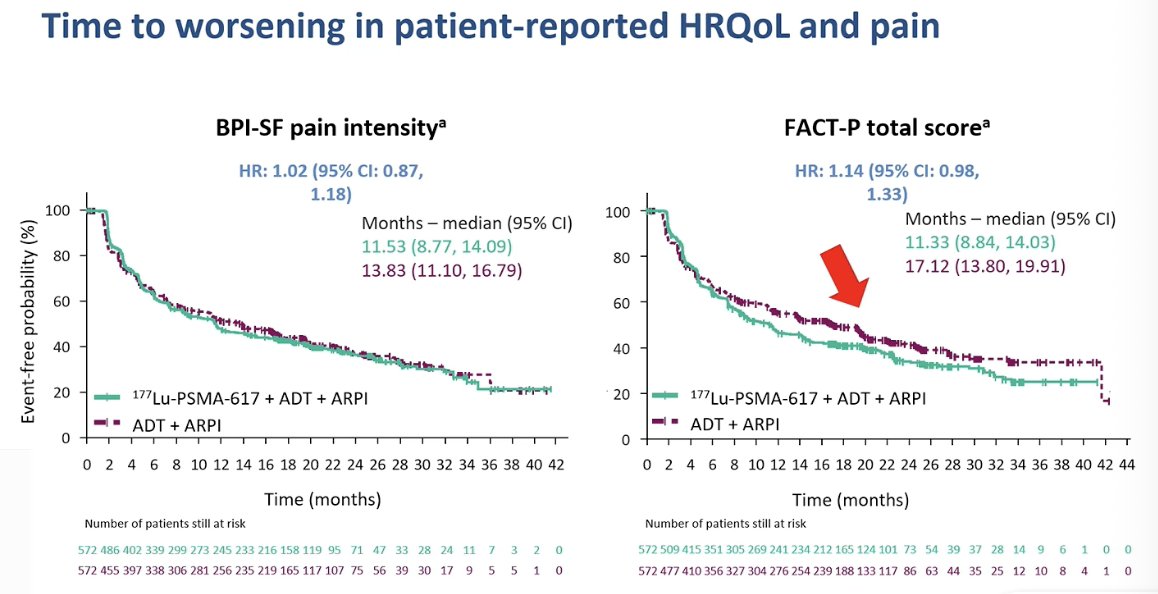
Regarding patient-reported outcomes, he noted it seems there is a potential decline in quality of life with the addition of 177Lu-PSMA-617. While time to worsening in pain intensity was similar between groups, the FACT-P analysis suggested an earlier deterioration in health-related quality of life in the combination arm compared with ADT plus ARPI alone, as illustrated in the figure.
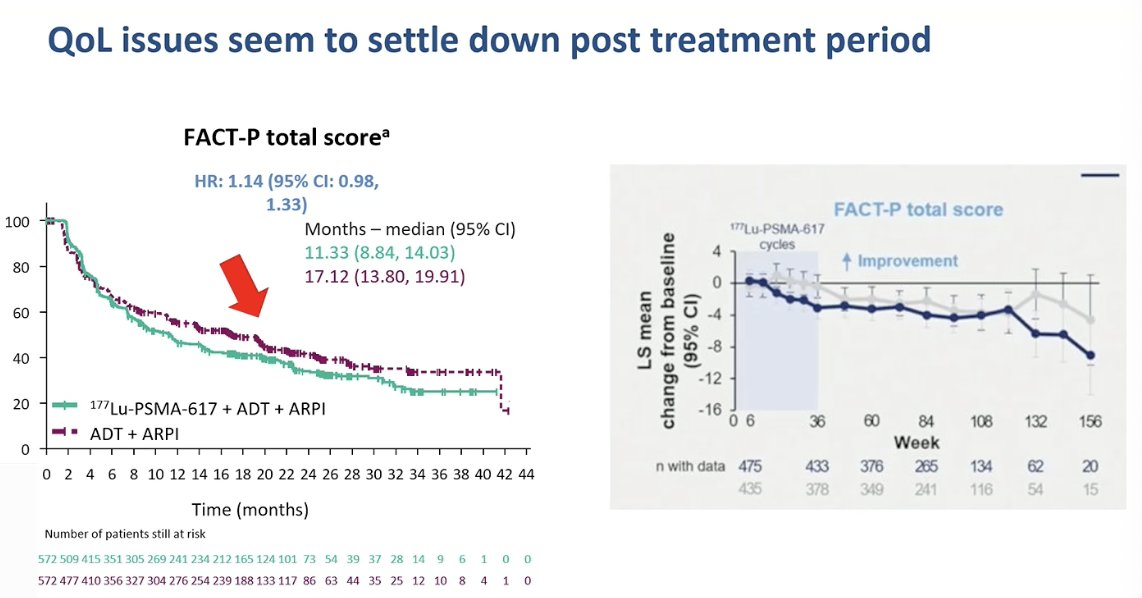
However, he noted that more recent data presented at ASCO GU last month suggest that these quality-of-life changes appear to stabilize after the treatment period. Patient-reported outcomes, including FACT-P scores, tend to recover over time, indicating that the initial decline in quality of life with 177Lu-PSMA-617 may be transient and not associated with a sustained long-term impairment, as shown in the curves below.
Dr. Murphy then reflected on the clinical implications of adding 177Lu-PSMA-617 in the mHSPC setting. He noted that if radiographic progression-free survival is considered a sufficiently meaningful endpoint, the strategy may appear reasonable. However, he emphasized that several existing treatment intensification strategies in mHSPC have already demonstrated overall survival benefits, and therefore, the absence of an overall survival signal with this approach warrants caution. In Australia, for example, reimbursement would not be expected until an overall survival benefit is demonstrated.
Looking ahead, Dr. Murphy suggested that future strategies may involve fewer treatment cycles and more adaptive dosing approaches. He noted that adaptive dosing may be particularly relevant in the mHSPC setting, where disease burden and target expression can change rapidly with therapy. Because theranostic treatments allow clinicians to visualize the target they are treating, the PSMA signal may diminish or even disappear after only a few months of therapy. In such situations, continuing additional cycles of radioligand therapy may provide little added benefit. He suggested that tailoring treatment duration based on imaging response and persistence of the target could represent an important future direction for theranostic therapy in prostate cancer.
Dr. Murphy concluded his presentation with several key takeaways:
- UpFrontPSMA and PSMAaddition demonstrate improvements in PSA responses and rPFS when 177Lu-PSMA-617 is combined with ADT plus docetaxel or ADT plus ARPI in mHSPC.
- However, no overall survival benefit has been demonstrated to date.
- Most clinicians worldwide will likely require mature overall survival data before broadly adopting this strategy in clinical practice.
- Future strategies may involve fewer treatment cycles and adaptive dosing approaches guided by imaging response.
- At present, 177Lu-PSMA-617 should not be considered standard of care for mHSPC in 2026.
- Radioligand therapy remains clearly established in the mCRPC setting at present.
Presented by: Declan Murphy, Urologist and Director of Genitourinary Oncology, Peter MacCallum Cancer Center, Honorary Clinical Professor of Urology, Melbourne University, Melbourne, Australia
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:- Hofman MS, Emmett L, Violet J, Y Zhang A, Lawrence NJ, Stockler M, Francis RJ, Iravani A, Williams S, Azad A, Martin A, McJannett M; ANZUP TheraP team; Davis ID. TheraP: a randomized phase 2 trial of 177 Lu-PSMA-617 theranostic treatment vs cabazitaxel in progressive metastatic castration-resistant prostate cancer (Clinical Trial Protocol ANZUP 1603). BJU Int. 2019 Nov;124 Suppl 1:5-13. doi: 10.1111/bju.14876. Epub 2019 Oct 22. PMID: 31638341.
- Sartor O, de Bono J, Chi KN, Fizazi K, Herrmann K, Rahbar K, Tagawa ST, Nordquist LT, Vaishampayan N, El-Haddad G, Park CH, Beer TM, Armour A, Pérez-Contreras WJ, DeSilvio M, Kpamegan E, Gericke G, Messmann RA, Morris MJ, Krause BJ; VISION Investigators. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103. doi: 10.1056/NEJMoa2107322. Epub 2021 Jun 23. PMID: 34161051; PMCID: PMC8446332.
- Azad AA, Bressel M, Tan H, Voskoboynik M, Suder A, Weickhardt AJ, Guminski A, Francis RJ, Saghebi J, Dhiantravan N, Joshua AM, Emmett L, Horvath L, Murphy DG, Hsiao E, Balakrishnar B, Lin P, Redfern A, Macdonald W, Ng S, Lee ST, Pattison DA, Nadebaum D, Kirkwood ID, Hofman MS; UpFrontPSMA Study Team. Sequential [177Lu]Lu-PSMA-617 and docetaxel versus docetaxel in patients with metastatic hormone-sensitive prostate cancer (UpFrontPSMA): a multicentre, open-label, randomised, phase 2 study. Lancet Oncol. 2024 Oct;25(10):1267-1276. doi: 10.1016/S1470-2045(24)00440-6. Epub 2024 Sep 15. PMID: 39293461
- Tagawa S. ESMO 2025: Phase III Trial of [177Lu]Lu-PSMA-617 Combined with ADT + ARPI in Patients with PSMA-Positive Metastatic Hormone-Sensitive Prostate Cancer (PSMAddition) at https://www.urotoday.com/conference-highlights/esmo-2025/esmo-2025-prostate-cancer/164097-esmo-2025-phase-iii-trial-of-177lu-lu-psma-617-combined-with-adt-arpi-in-patients-with-psma-positive-metastatic-hormone-sensitive-prostate-cancer-psmaddition.html.