(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a PARP inhibitors for prostate cancer session and a presentation by Dr. Martin Gleave discussing how to optimize tissue biopsy acquisition. The reason we biopsy patients is that it is actionable and informative. First, it confirms the diagnosis and may identify histologies of treatment emergent phenotypes such as neuroendocrine prostate cancer. Second, it enables genomic profiling for precision oncology, identifying DNA repair and MMR defects, as well as PTEN deficiency. These results can be prognostic (PTEN deficiency poorly controlled with androgen receptor inhibitors alone) and predictive (treatment selection, for example, PD-L1 for MMR deficient tumors, and PARP inhibitors for HRR mutation tumors). For those undergoing germline testing, family counseling can be initiated, particularly for those with BRCA, HOXB13, and Lynch syndrome. Furthermore, a biopsy may identify patients for clinical trial eligibility.
Who should be biopsied and when?
- Men with newly diagnosed de novo metastatic castration sensitive prostate cancer (CSPC). This is done to confirm histology, perform baseline genomic profiling, and may also include germline testing. This is done preferably by an ultrasound-guided transperineal prostate biopsy (MRI or DRE informed), with multiple cores taken from the region of interest for tumor content
- Men with metastatic castration resistant prostate cancer (mCRPC) progression. Allows identification of targetable alterations, as well as evaluation of emergent treatment resistance. This is also important when ctDNA is not evaluable (ie. low tumor content)
- Progression with atypical clinical features. This includes those with rapid progression, visceral metastases, and low PSA relative to the disease burden.
Where and what tissue should be biopsied? Archival tissue is convenient and a reasonable first pass, but fails in 30-50% of cases, thus it may under represent heterogeneity, especially in mCRPC. What is preferred is a metastatic biopsy site, especially if it is accessible, for those with progressing disease, and for PET-prioritized lesions. This includes:
- Lymph nodes: easiest, highest yield
- Liver: good tumor cellularity, often reflecting aggressive disease
- Lung: feasible via CT guidance, but may be more indolent
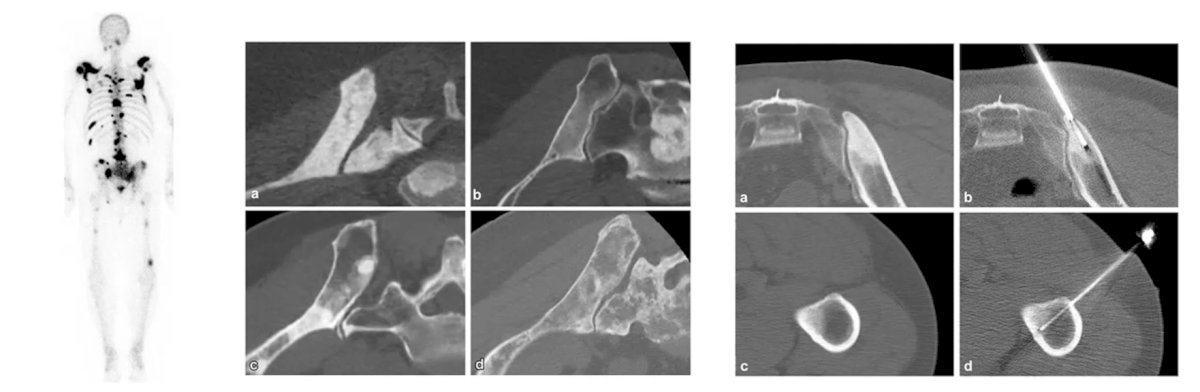
- Bone: the most common site of metastases, but technically challenging. These lesions are often sclerotic, and acid decalcification can degrade DNA
There are several specific challenges with metastatic bone biopsy for prostate cancer. The overall success rate of CT-guided bone biopsies is ~65% for histology and ~64% for RNA sequencing. The yield may be higher in areas of radiolucency versus dense sclerosis, and stimulated Raman histology may improve characterization of tumor cellularity yields:
Alternatives to bone biopsy include ctDNA liquid biopsy, archival tissue, or repeat transperineal guided biopsy if the patient is progressing locally.
The main reason to not simply biopsy the prostate in metastatic prostate cancer is that the prostate biopsy may not reflect biology, especially in patients with mCRPC. Prostate cancer can evolve genomically under treatment pressure with androgen receptor mutations, copy number gains/losses, and lineage plasticity. Of note, the SU2C West Coast dream team patients showed substantial genomic heterogeneity between primary and metastatic lesions. Importantly, the prostate biopsy may more likely reflect the biology in mCSPC. In the GUNS trial, 85% of biopsies in high risk localized prostate cancer were evaluable, and actionable alterations were found in 58% of patients, with 22% of patients being PARP inhibitor candidates. Dr. Gleave concluded by stating that a prostate biopsy may be appropriate for:
- Patients with de novo mCSPC to establish diagnosis, histological variants, and tissue for genomic testing
- In patients with progressing mCRPC when metastases are inaccessible, and ctDNA is negative. This may be performed with transperineal ultrasound guidance, assessing multiple cores from MRI or DRE informed regions of interest
Presented by: Martin Gleave, MD, FRCSC, FACS, Vancouver Prostate Centre, University of British Columbia, Vancouver, Canada
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.