(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K. between March 13th and 16th 2026, was host to the Hormone sensitive metastatic prostate cancer: Thematic Session. Dr. Gunhild von Amsberg delivered a presentation titled: PARPi in mHSPC or should we wait until mCRPC?
Dr. von Amsberg began by noting that, to date, no randomized trial has specifically addressed the optimal timing of PARP inhibitor therapy in prostate cancer. She emphasized that several key factors should guide treatment decisions. First, clinicians should consider the available phase III evidence across different disease states.1-6 Second, the prognostic significance of HRR alterations, particularly BRCA1/2 mutations, should be taken into account. She also highlighted that treatment effects vary across HRR subgroups, underscoring the importance of careful patient selection. Finally, benefit-risk considerations remain essential, including the potential for long-term toxicities associated with PARP inhibitor therapy.
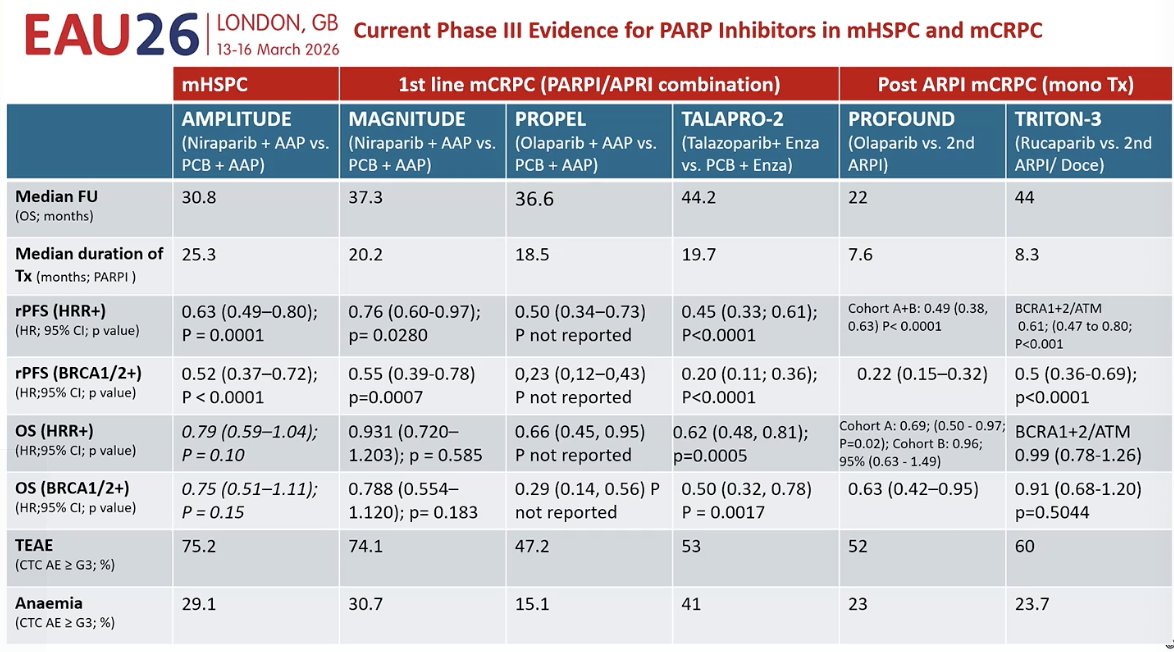
Dr. von Amsberg then reviewed the phase III evidence for PARP inhibitors across prostate cancer disease states. In mCRPC, five phase III trials have reported results: three evaluating combinations of an ARPI plus a PARP inhibitor (MAGNITUDE, PROpel, and TALAPRO-2)2-4 and two evaluating PARP inhibitor monotherapy after ARPI exposure (PROfound and TRITON-3).5 Across these studies, patients with BRCA1/2 alterations consistently derived the greatest benefit, with the most pronounced improvements observed in both rPFS and overall survival.
In the mHSPC setting, the AMPLITUDE trial represents the main phase III evidence to date.1 Similar to what has been observed in mCRPC, the greatest benefit was seen in patients harboring BRCA1/2 alterations. She also noted that treatment exposure appeared more favorable in the hormone-sensitive setting compared with the castration-resistant setting. Importantly, the safety profile was generally consistent across disease states, with similar rates of anemia reported in both mHSPC and mCRPC populations.
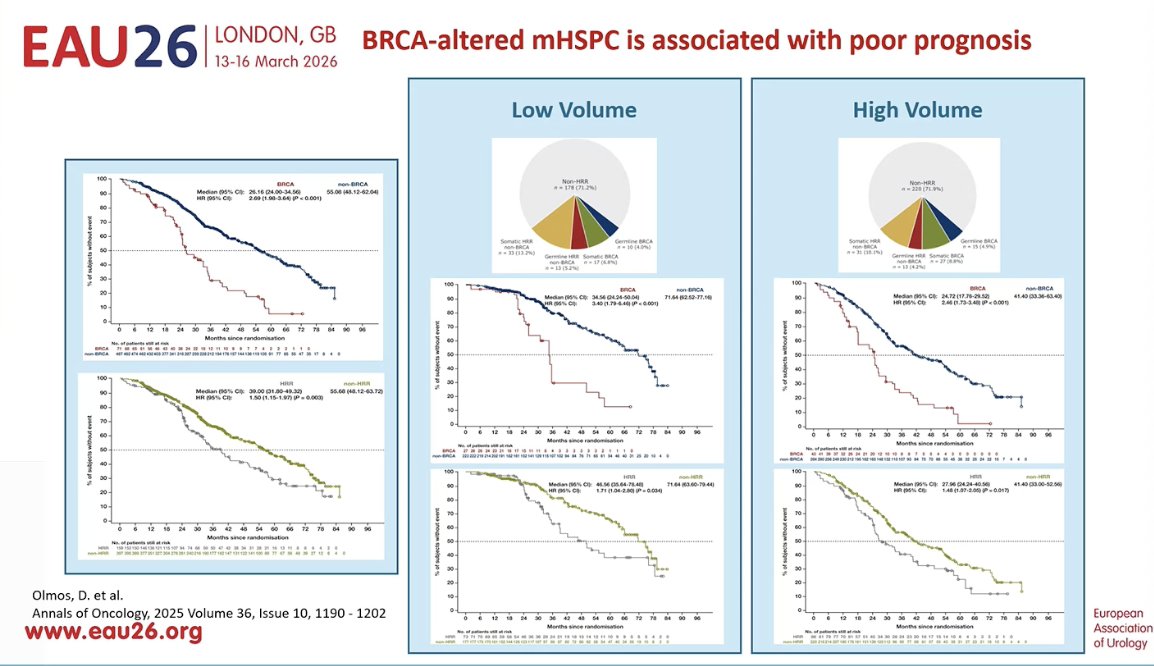
Dr. von Amsberg then addressed the prognostic implications of HRR alterations in the mHSPC setting. She noted that the prevalence of HRR alterations is similar across low-volume and high-volume disease, raising the important question of who should undergo testing. Based on the available data, she emphasized that genomic testing should be performed broadly, as approximately 10% of patients harbor BRCA alterations.1
Importantly, patients with BRCA alterations have significantly worse outcomes compared with those without these mutations. A similar pattern is observed when comparing patients with HRR alterations versus those without. These poorer outcomes appear consistent regardless of disease volume, underscoring the prognostic significance of HRR alterations in mHSPC.
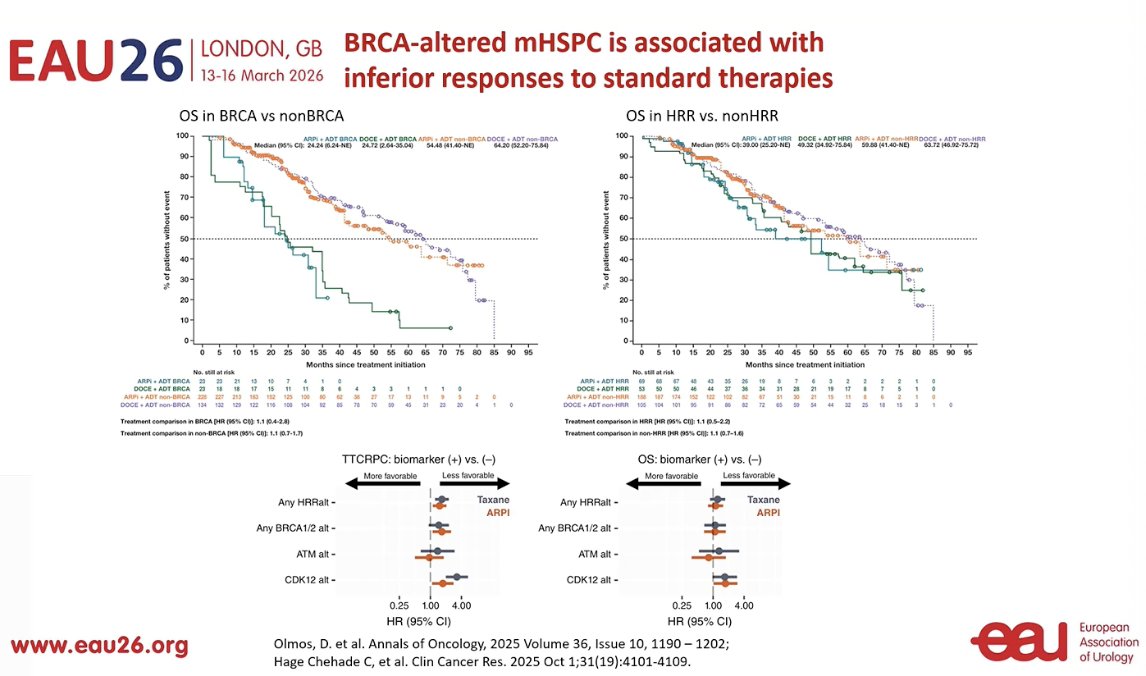
Dr. von Ambserg highlighted that patients with BRCA alterations tend to have inferior responses to standard therapies in the mHSPC setting. Compared with patients without these alterations. This further supports the rationale for considering PARP inhibitor strategies earlier in the treatment course for these patients. She also noted that emerging data suggest patients with CDK12 alterations may experience similarly poor outcomes, performing almost as poorly as those with BRCA mutations in some analyses from U.S. cohorts. These findings further emphasize the importance of molecular profiling to guide treatment decisions in advanced prostate cancer.
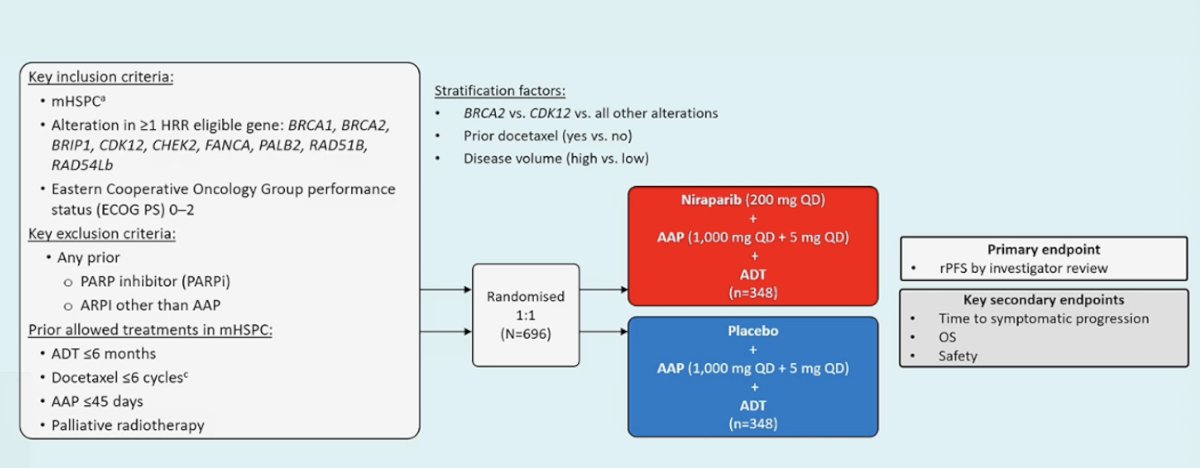
Going back to the AMPLITUDE trial, this was a phase III randomized study evaluating niraparib in combination with abiraterone acetate plus prednisone and ADT in patients with mHSPC harboring HRR alterations. Eligible patients had alterations in at least one HRR gene, including BRCA1, BRCA2, ATM, PALB2, CHEK2, FANCA, RAD51B, RAD54L, and others, with an ECOG performance status of 0–2. Patients were randomized 1:1 to receive niraparib plus AAP and ADT or placebo plus AAP and ADT. Randomization was stratified according to BRCA2 versus other HRR alterations, prior docetaxel exposure, and disease volume (high versus low). The primary endpoint was radiographic progression-free survival by investigator review, with key secondary endpoints including time to symptomatic progression, overall survival, and safety. The study design is shown below.
Notably, the trial met its primary endpoint of rPFS. In patients with BRCA alterations, niraparib plus AAP significantly improved rPFS compared with placebo plus AAP (HR 0.52; 95% CI 0.37–0.72; p<0.0001), with the median rPFS not yet reached in the niraparib arm versus 26.0 months in the control arm. A similar benefit was observed in the overall HRR-mutated population, with an HR of 0.63 (95% CI 0.49–0.80; p=0.0001), again with median rPFS not reached in the niraparib arm compared with 29.5 months in the placebo arm.1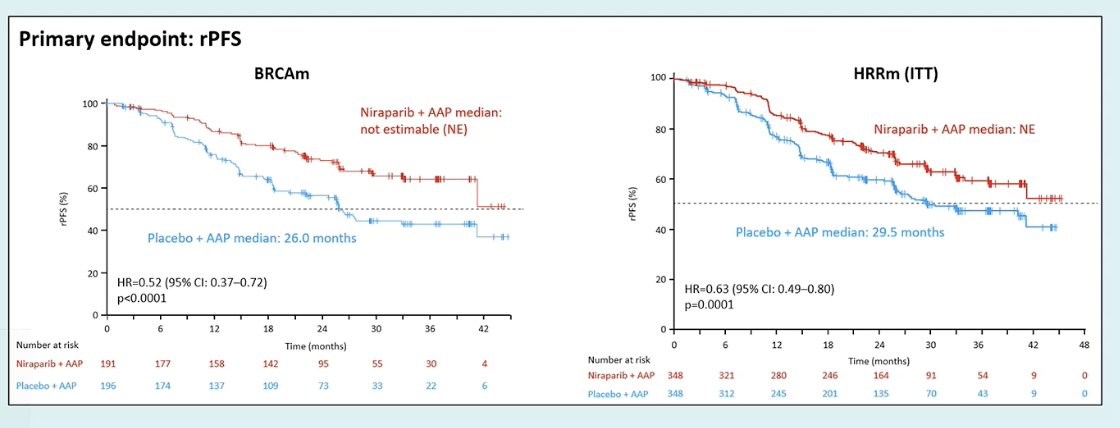
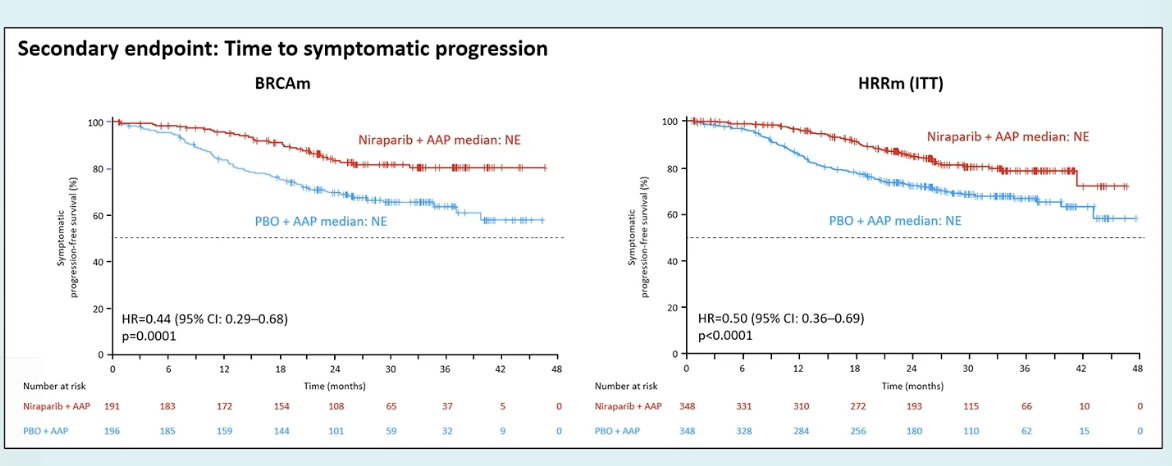
Similarly, niraparib plus AAP significantly improved time to symptomatic progression compared with placebo plus AAP. In patients with BRCA alterations, the hazard ratio was 0.44 (95% CI 0.29–0.68; p=0.0001), while in the overall HRR-mutated population the hazard ratio was 0.50 (95% CI 0.36–0.69; p<0.0001), with median time to symptomatic progression not reached in either arm. These results further support the clinical benefit of adding niraparib to AAP in patients with HRR-altered mHSPC.1
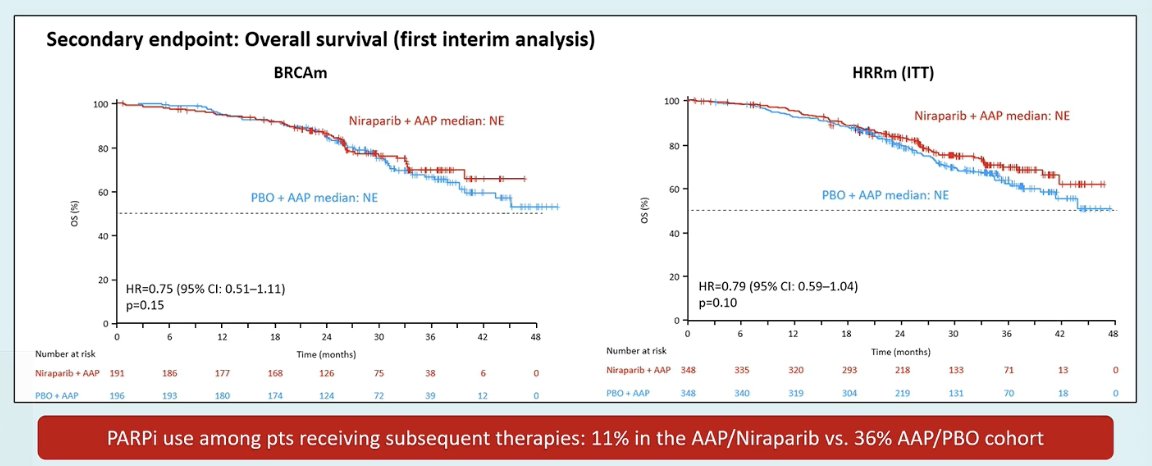
Overall survival data remain immature at this first interim analysis. Although there was a numerical trend favoring niraparib plus AAP in both the BRCA-mutated and overall HRR-mutated populations, the differences did not reach statistical significance at this stage (BRCA: HR 0.75; HRR: HR 0.79). Notably, PARP inhibitor use among patients receiving subsequent therapies was higher in the control arm, with 36% of patients in the AAP/placebo group receiving a PARP inhibitor compared with 11% in the AAP/niraparib arm, which may influence the final OS anal
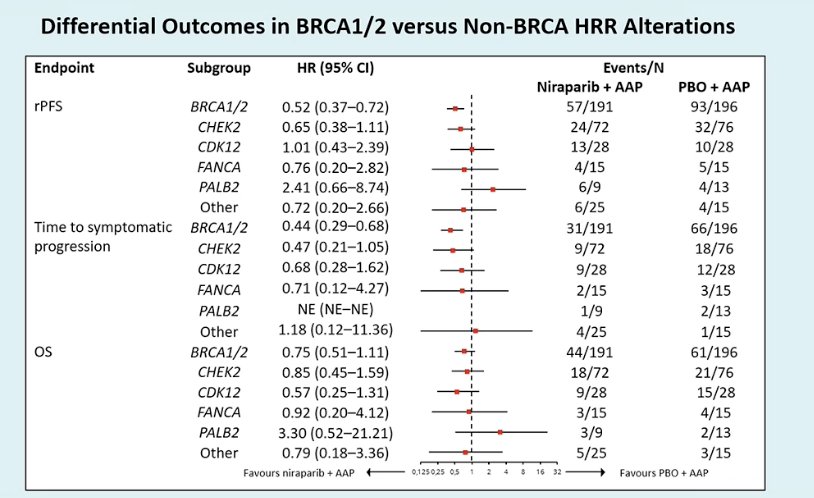
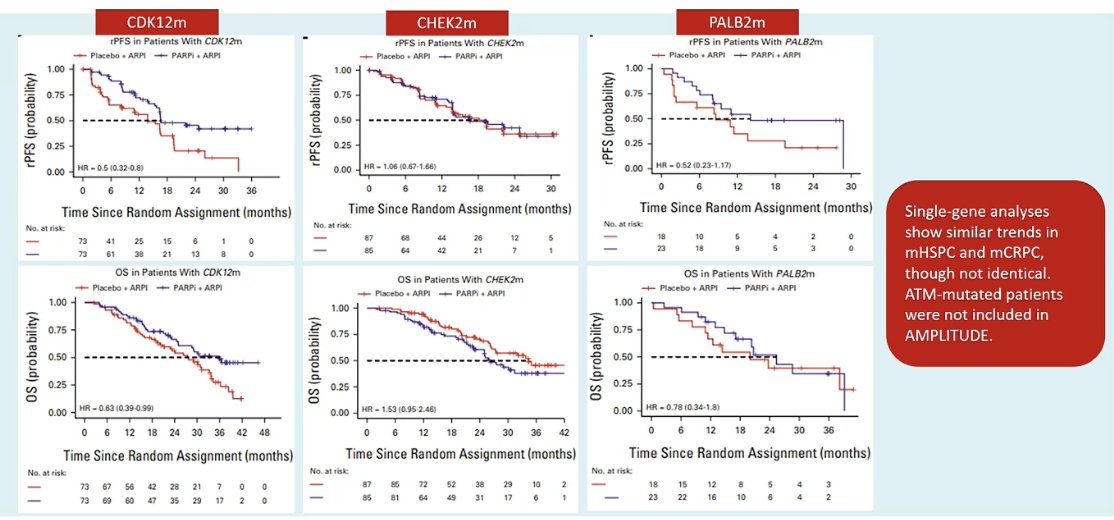
She highlighted the differential outcomes observed across HRR subgroups. The greatest benefit with niraparib plus AAP was seen in patients with BRCA1/2 alterations, with consistent improvements in rPFS and time to symptomatic progression. In contrast, treatment effects in non-BRCA HRR alterations such as CHEK2, CDK12, FANCA, and PALB2 appeared more variable and less pronounced, emphasizing that the magnitude of benefit from PARP inhibition differs substantially across HRR subgroups.
Dr. von Amsberg also highlighted a meta-analysis in the mCRPC setting evaluating outcomes according to individual HRR gene alterations. These analyses suggest that patients with alterations such as CDK12 and PALB2 may derive greater benefit from PARP inhibitor–based approaches, whereas patients with CHEK2 alterations appear to derive less benefit. She also noted that single-gene analyses show broadly similar trends across mHSPC and mCRPC, although results are not identical, and ATM-mutated patients were not included in the AMPLITUDE trial.
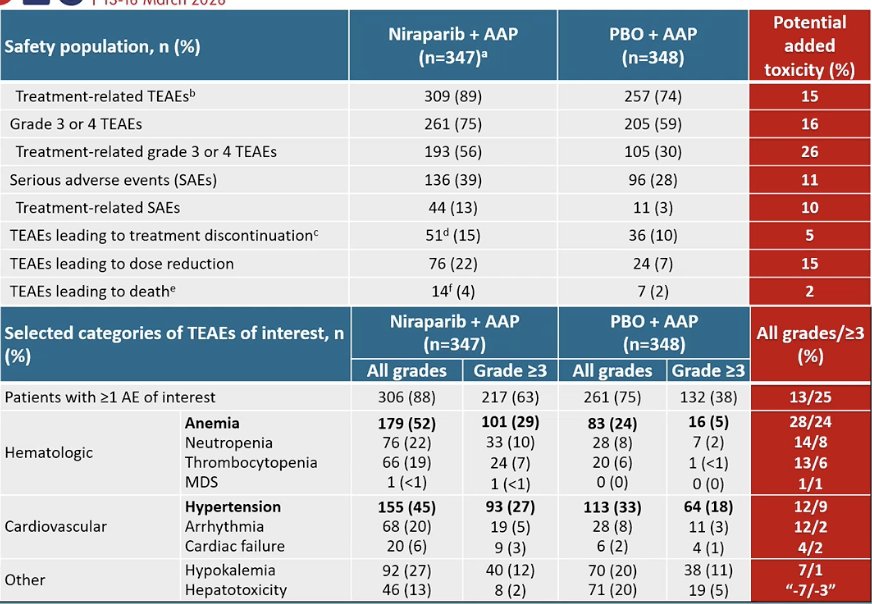
As expected, the combination was associated with higher toxicity compared with AAP alone. Hematologic adverse events were more frequent, particularly anemia, which occurred in roughly one-third more patients receiving the PARP inhibitor combination. Higher rates of neutropenia and thrombocytopenia were also observed. These findings highlight the importance of carefully weighing the clinical benefit against the added toxicity when considering PARP inhibitor combinations in this setting.1
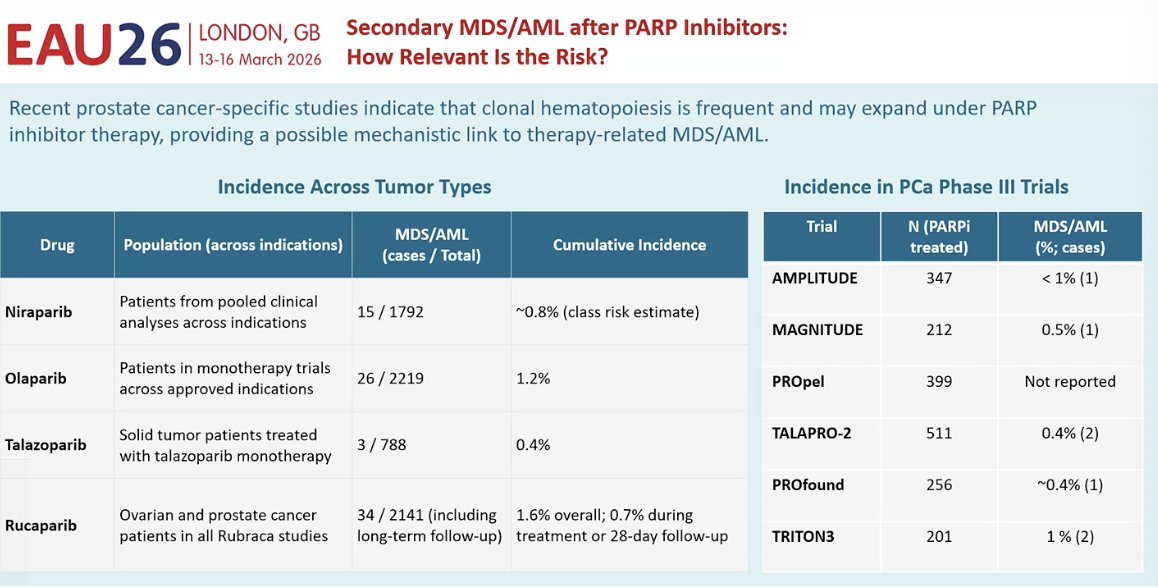
She also addressed concerns regarding long-term toxicity with PARP inhibitors, particularly the potential risk of myelodysplastic syndrome (MDS) and acute myeloid leukemia (AML). One proposed mechanism relates to clonal hematopoiesis, which is relatively common in older patients and may expand under the selective pressure of PARP inhibitor therapy. However, across prostate cancer phase III trials, the absolute risk of MDS or AML remains very low, generally reported in well under 1% of treated patients (Table below). These data suggest that while the risk should be recognized and monitored, it remains uncommon in clinical practice.
Lastly, she discussed the impact of the AMPLITUDE regimen on quality of life. Overall, patient-reported outcomes, including FACT-P and EQ-5D-5L scores, suggested that the addition of niraparib to AAP had a manageable impact on quality of life. While some decline was observed over time, the overall trends between treatment arms remained relatively similar, indicating that the addition of PARP inhibition did not result in a major deterioration in patient-reported quality-of-life measures.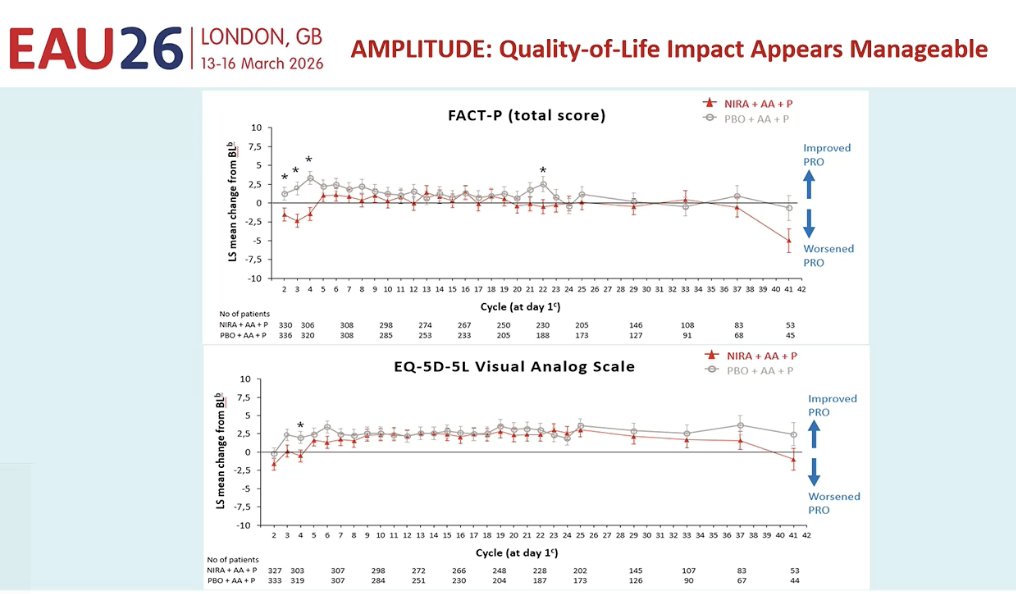
Dr. von Amsberg concluded with several key considerations:
- Patients with BRCA1/2-mutated mHSPC have a poorer prognosis and appear to derive less benefit from standard therapies such as ARPIs and docetaxel.
- Randomized trials consistently show the greatest and most robust rPFS benefit, with emerging OS signals, for PARP inhibitor–based combinations in this population, both in mCRPC and now in mHSPC.
- In contrast, outcomes among patients with non-BRCA HRR alterations are more heterogeneous, and the magnitude of benefit from PARP inhibition remains less clear.
- Ongoing trials in the mHSPC setting, including TALAPRO-3 and EvoPAR-PR01, will help determine whether PARP inhibitors should be used earlier and which patients are most likely to benefit.
- Long-term toxicity remains an important consideration. Although the cumulative incidence of therapy-related myelodysplastic syndrome (MDS) and acute myeloid leukemia (AML) is low, it is not negligible, highlighting the importance of long-term hematologic monitoring, particularly as PARP inhibitors move into earlier disease settings.
- Clonal hematopoiesis is common in men with advanced prostate cancer and may expand with PARP inhibitor exposure, which could partly explain these rare hematologic events.
- Importantly, up to one in four men receive no further therapy after progression from mHSPC. Therefore, effective treatments should not necessarily be deferred to later lines of therapy when patients may never reach them.
Presented by: Gunhild von Amsberg, MD, Urologic Oncologist, UCC-Hamburg, Associated Faculty der Martini-Klinik, Hamburg, Germany
- Attard G, Agarwal N, Graff JN, Sandhu S, Efstathiou E, Özgüroğlu M, Pereira de Santana Gomes AJ, Vianna K, Luo H, Gotto GT, Cheng HH, Kim W, Varela CR, Schaeffer D, Kramer K, Li S, Baron B, Shen F, Mundle SD, McCarthy SA, Olmos D, Chi KN, Rathkopf DE. Niraparib and abiraterone acetate plus prednisone for HRR-deficient metastatic castration-sensitive prostate cancer: a randomized phase 3 trial. Nat Med. 2025 Dec;31(12):4109-4118. doi: 10.1038/s41591-025-03961-8. Epub 2025 Oct 7. PMID: 41057655; PMCID: PMC12705445.
- Chi KN, Rathkopf DE, Smith MR, Efstathiou E, Attard G, Olmos D, et al. Niraparib plus abiraterone acetate for metastatic castration-resistant prostate cancer with homologous recombination repair gene alterations (MAGNITUDE). Lancet Oncol. 2023;24(6):703-716. doi:10.1016/S1470-2045(23)00177-6.
- Clarke NW, Armstrong AJ, Thiery-Vuillemin A, Oya M, Shore ND, Loredo E, et al. Olaparib combined with abiraterone in patients with metastatic castration-resistant prostate cancer (PROpel): a randomised, double-blind, phase 3 trial. N Engl J Med. 2022;387:1747-1759. doi:10.1056/NEJMoa2209045.
- Agarwal N, Azad AA, Carles J, Fay AP, Matsubara N, Heinrich D, et al. Talazoparib plus enzalutamide in metastatic castration-resistant prostate cancer (TALAPRO-2). N Engl J Med. 2023;389:1529-1541. doi:10.1056/NEJMoa2304694.
- de Bono J, Mateo J, Fizazi K, Saad F, Shore N, Sandhu S, et al. Olaparib for metastatic castration-resistant prostate cancer. N Engl J Med. 2020;382:2091-2102. doi:10.1056/NEJMoa1911440.
- Abida W, Campbell D, Patnaik A, Sautois B, Vogelzang NJ, Shapiro JD, et al. Rucaparib versus physician’s choice of therapy in patients with metastatic castration-resistant prostate cancer associated with homologous recombination deficiency (TRITON-3): a randomised, open-label ph