(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., was host to the Hormone sensitive metastatic prostate cancer: Thematic Session. Dr. Valerie Fonteyne discussed What evidence do we have from intensification with SBRT?
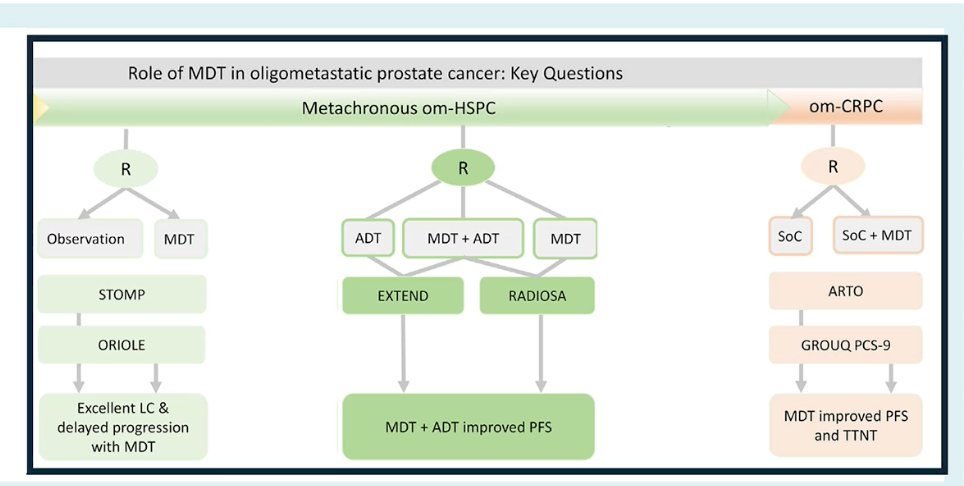
Dr. Fonteyne began by reviewing the current evidence supporting metastasis-directed therapy (MDT) in oligometastatic prostate cancer, noting that most of the available data come from the setting of metachronous oligometastatic hormone-sensitive disease. Early trials such as STOMP and ORIOLE demonstrated excellent local control with MDT, with delayed disease progression and minimal toxicity, supporting the concept that treating limited metastatic sites may modify the natural history of the disease.1
She also highlighted the RADIOSA trial, where the combination of ADT plus MDT improved progression-free survival compared with MDT alone.2 In the castration-resistant oligometastatic setting, the ARTO trial showed that adding MDT to standard of care improved progression-free survival.3 While these data suggest that MDT can provide clinical benefit across different oligometastatic states, Dr. Fonteyne emphasized that integrating MDT into international guidelines remains challenging due to the small size of available trials and the heterogeneity in inclusion criteria and clinical endpoints.
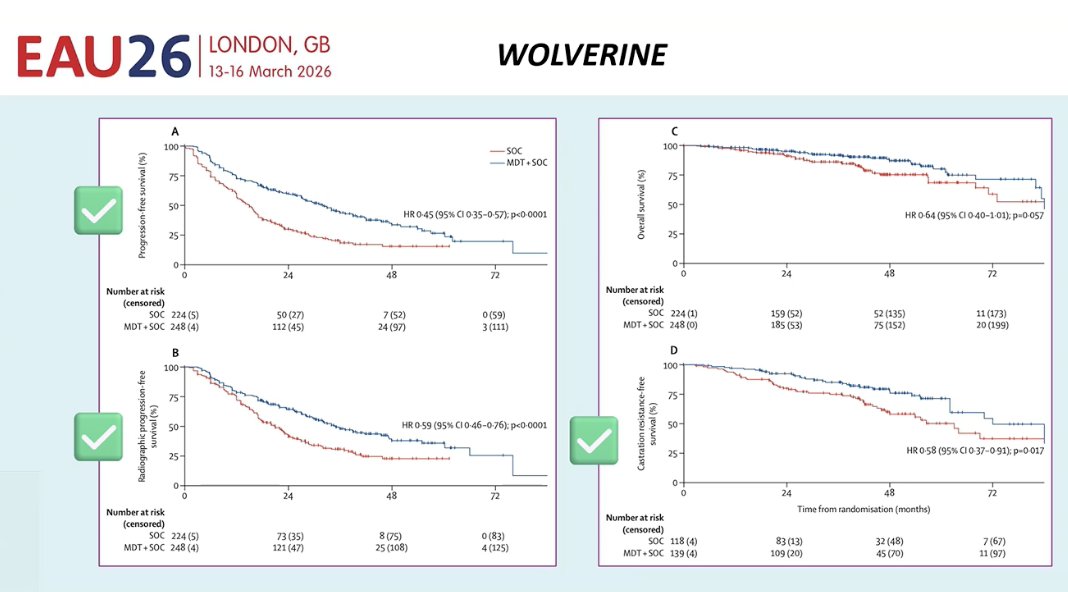
She then discussed results from the WOLVERINE trial evaluating the addition of MDT to standard of care in oligometastatic prostate cancer. The study demonstrated that adding MDT significantly improved progression-free survival and radiographic progression-free survival compared with standard therapy alone. In addition, MDT delayed progression to castration-resistant disease, suggesting a meaningful disease-control benefit with this approach. However, despite these improvements in disease-related outcomes, no statistically significant overall survival benefit was observed.4
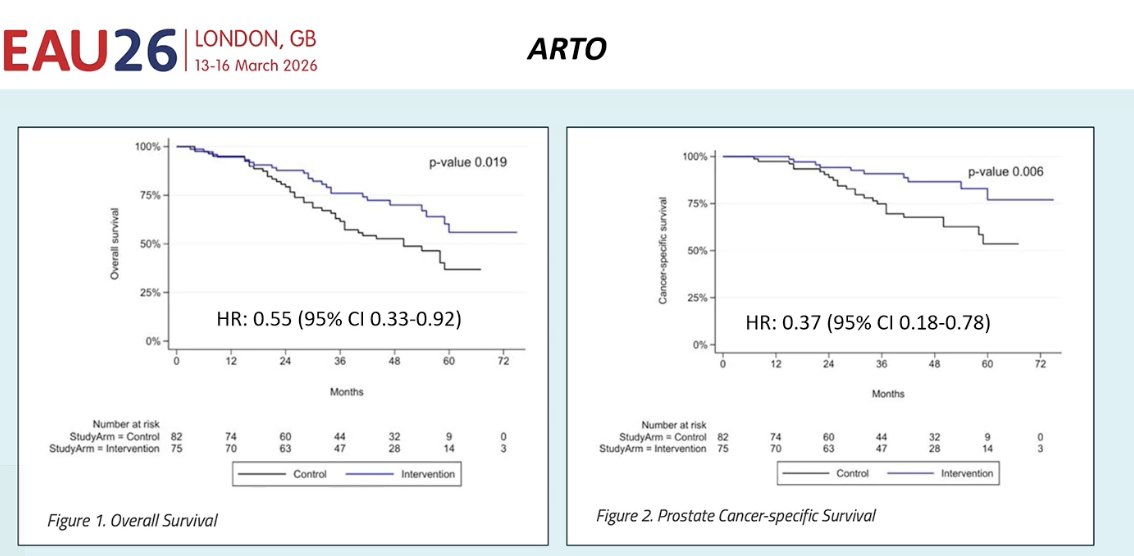
Moreover, she highlighted results from the ARTO trial, which provided the first randomized evidence suggesting that MDT may improve survival outcomes. In this study, the addition of MDT to standard systemic therapy was associated with improvements not only in progression-related endpoints but also in overall survival and prostate cancer–specific survival compared with standard treatment alone, as illustrated in the Kaplan-Meier curves below.3
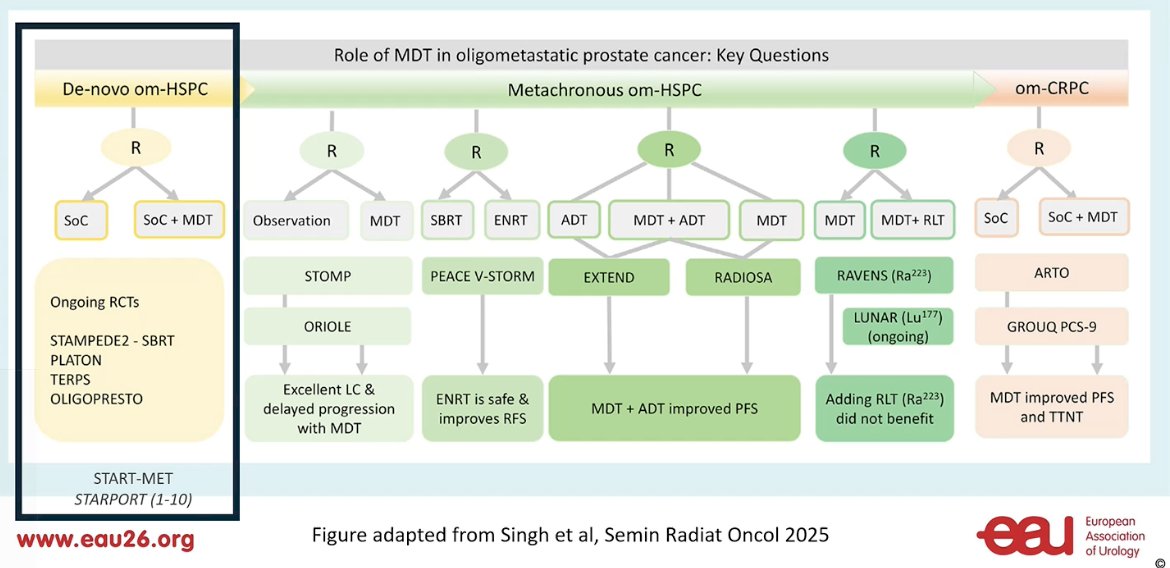
She then addressed the question of MDT in de novo oligometastatic hormone-sensitive prostate cancer, emphasizing that high-level evidence in this setting remains limited. Most of the available data supporting MDT comes from metachronous oligometastatic disease rather than patients presenting with de novo metastases.
Currently, several randomized trials are ongoing to clarify the role of MDT in this population, including STAMPEDE2 evaluating SBRT, as well as the PLATON, TERPS, and OLIGOPRESTO studies. These trials are expected to provide important evidence on whether adding MDT to standard of care can improve outcomes in patients with de novo oligometastatic HSPC.
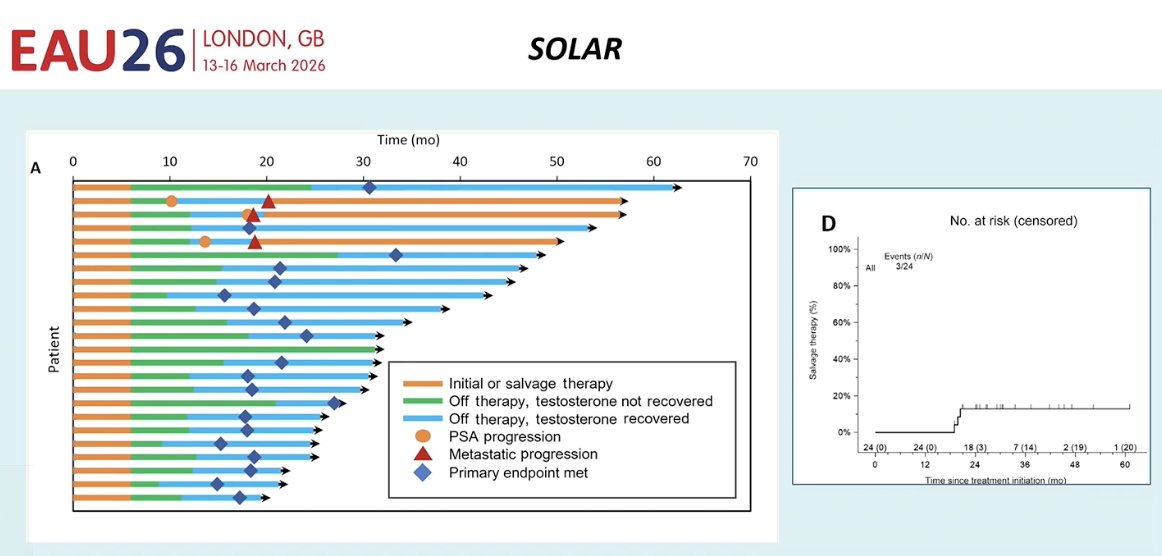
Dr. Fonteyne also discussed the SOLAR trial, a small study that included 21 patients. The aim of the trial was to evaluate whether hormonal therapy could be safely discontinued after MDT while maintaining disease control. Specifically, investigators assessed whether patients could recover testosterone levels while continuing to maintain very low PSA levels after treatment. The study explored the concept that MDT might allow treatment de-escalation in selected patients by enabling a treatment-free interval without immediate biochemical or metastatic progression.5
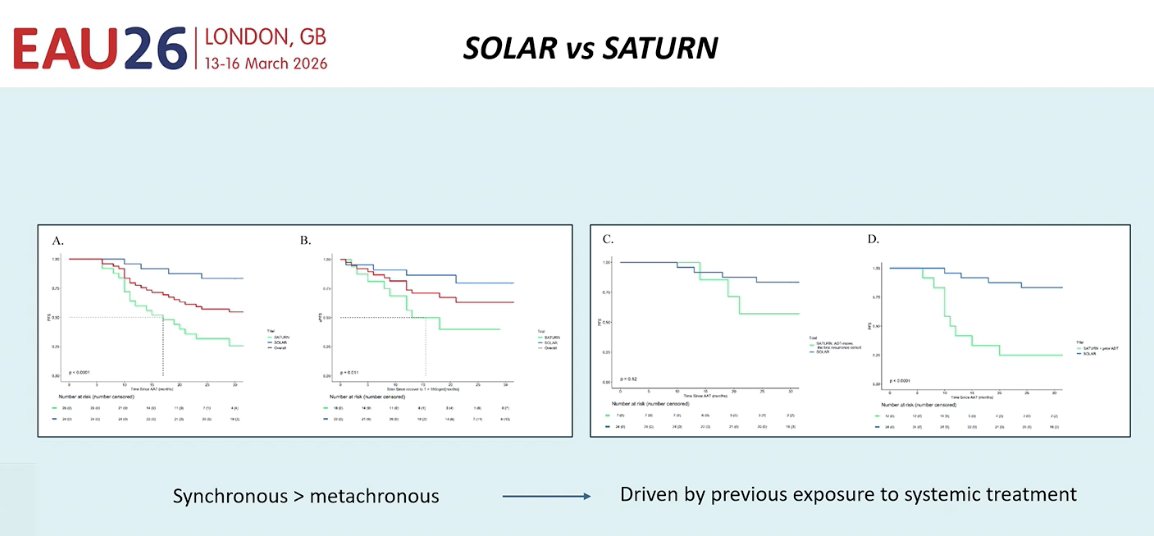
She then compared the SOLAR and SATURN trials. SATURN evaluated patients with metachronous oligometastatic HSPC, whereas SOLAR included patients with synchronous disease. Outcomes appeared more favorable in SOLAR than in SATURN, suggesting that synchronous disease may derive greater benefit from MDT compared with metachronous recurrence. This raises the hypothesis that earlier use of MDT in the disease course could be more effective. However, these findings remain hypothesis-generating and will need to be confirmed in larger randomized trials.6
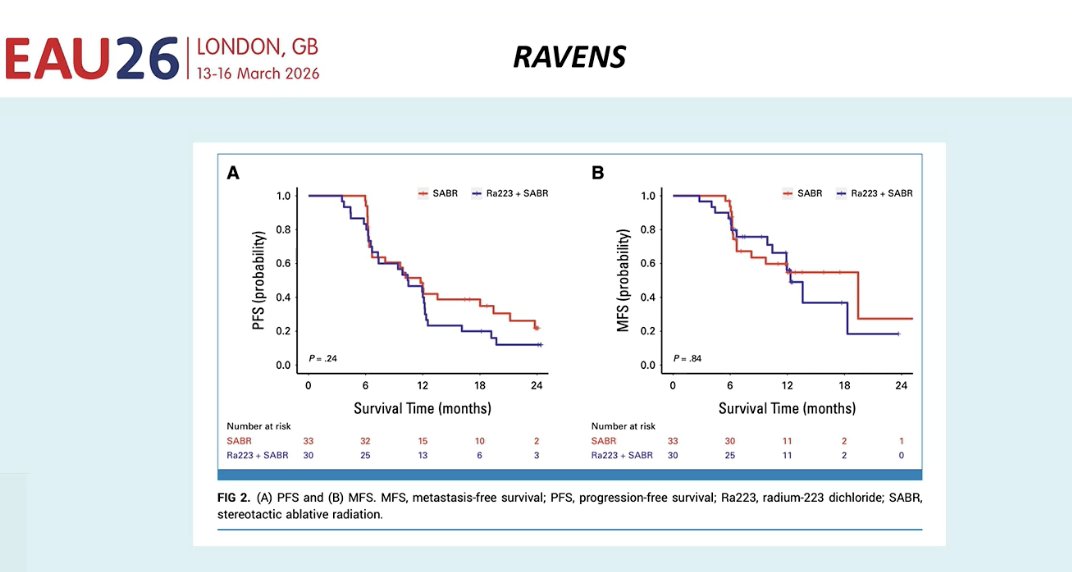
She also highlighted growing interest in combining MDT with radioligand therapy. Trials such as RAVENS evaluating Ra-223 and the ongoing LUNAR study with Lu-177 are exploring this strategy. However, early data suggest that adding radioligand therapy to MDT has not clearly demonstrated additional benefit so far, and further evidence is needed to clarify whether this combination can improve outcomes.
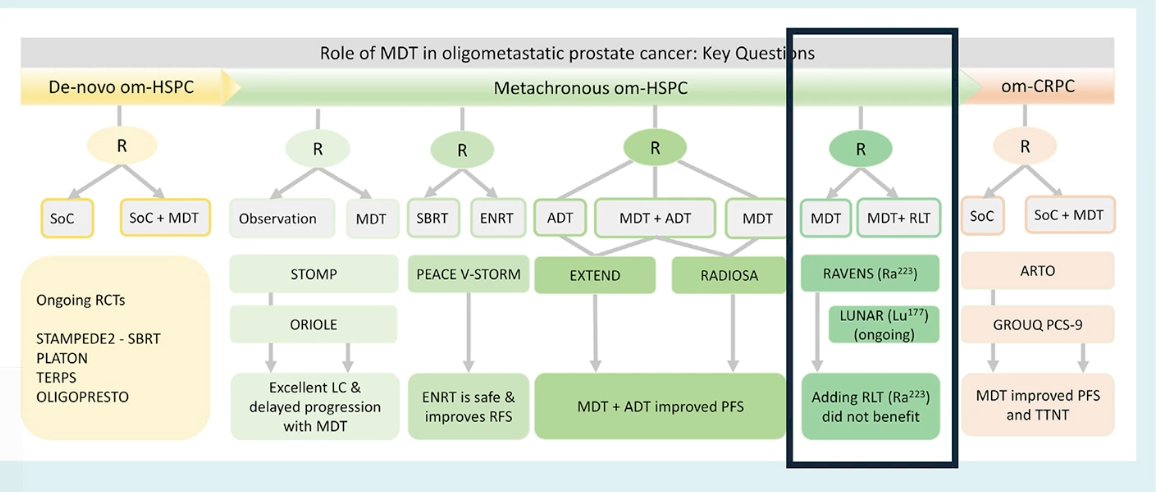
However, as shown in the RAVENS trial, adding Ra-223 to MDT did not improve progression-free survival or metastasis-free survival compared with MDT alone.7
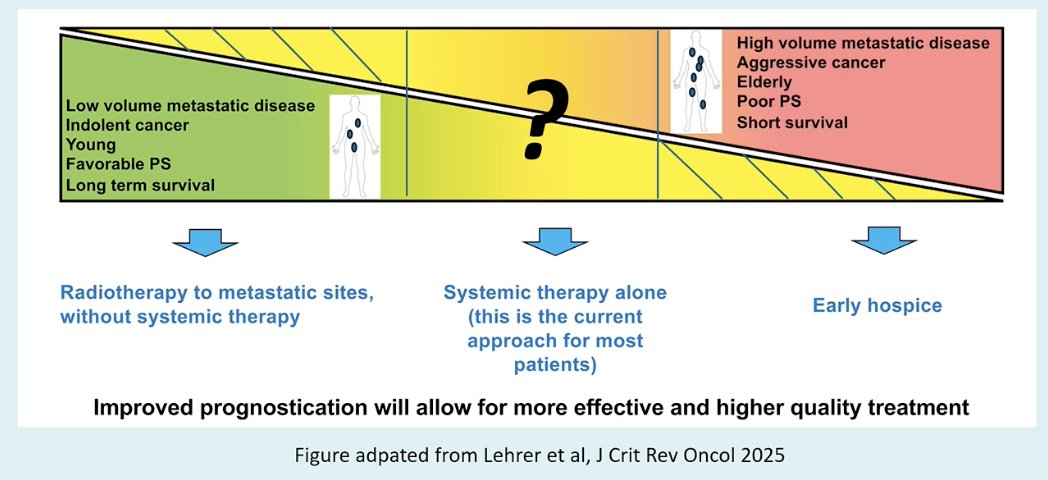
She concluded by emphasizing that patient selection remains the key challenge in oligometastatic prostate cancer. On one end of the spectrum are patients with low-volume metastatic disease, indolent biology, younger age, favorable performance status, and longer life expectancy, who may benefit from aggressive local approaches such as radiotherapy to metastatic sites, sometimes even with limited systemic therapy. On the opposite end are patients with high-volume disease, aggressive cancer, poor performance status, and shorter survival, where treatment strategies may be more focused on systemic therapy or supportive care. For most patients, systemic therapy alone remains the current standard approach. Improving prognostication and identifying the patients most likely to benefit from MDT will be critical to delivering more effective and higher-quality care.
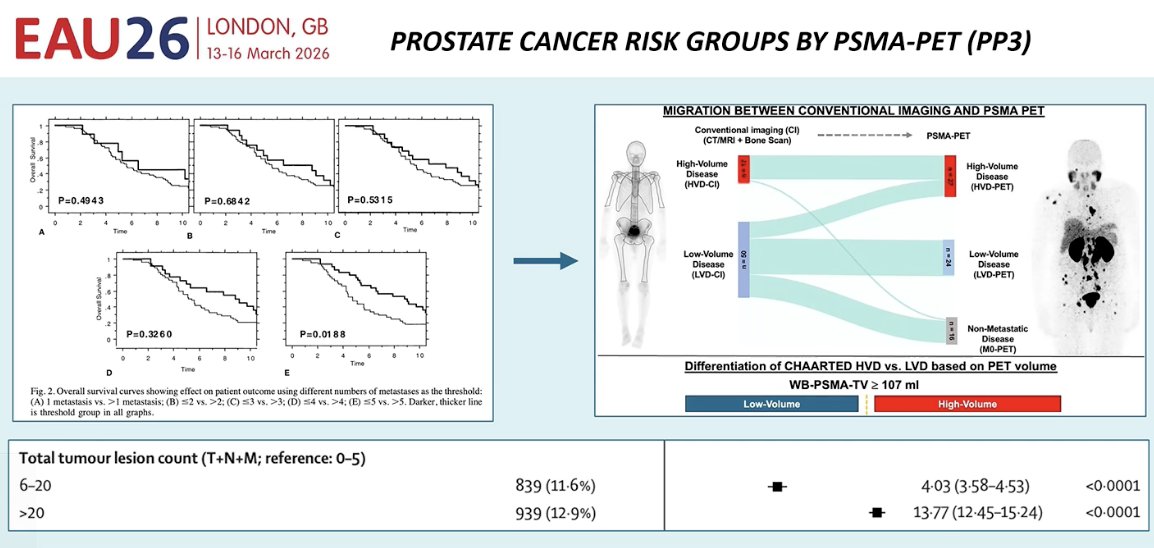
One final point she emphasized is that we often define patients who may benefit from MDT based primarily on the number of metastatic lesions, typically using a cutoff of up to five metastases to define oligometastatic disease. However, she highlighted a recently published retrospective analysis evaluating PSMA PET–based risk stratification (PP3), which examined how tumor burden assessed on PSMA PET correlates with overall survival. The study suggests that PSMA PET may provide a more refined assessment of metastatic burden compared with conventional imaging.
Still, lesion count alone does not capture the full biological picture. She emphasized that future strategies will likely incorporate biomarkers to better identify which patients may benefit from a pure MDT approach and which patients require more intensified systemic therapy.
Dr. Fonteyne concluded with several key take-home messages:
- Growing evidence supports the role of MDT in metastatic prostate cancer.
- Most of the available data come from the oligorecurrent setting, where MDT has been shown to delay disease progression and postpone the initiation of systemic therapy.
- Combining SBRT with systemic therapy appears to further improve outcomes compared with MDT alone.
- The ARTO trial may represent the first randomized study suggesting a potential overall survival benefit with MDT.
- Despite these encouraging results, several questions remain unanswered. The most important challenge moving forward is optimal patient selection, identifying which patients are most likely to benefit from MDT strategies.
Presented by: Valerie Fonteyne, MD, PhD, Associate Professor, Radiation Oncology, University of Ghent, East Flanders, Belgium
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:- Deek MP, Van der Eecken K, Sutera P, Deek RA, Fonteyne V, Mendes AA, Decaestecker K, Kiess AP, Lumen N, Phillips R, De Bruycker A, Mishra M, Rana Z, Molitoris J, Lambert B, Delrue L, Wang H, Lowe K, Verbeke S, Van Dorpe J, Bultijnck R, Villeirs G, De Man K, Ameye F, Song DY, DeWeese T, Paller CJ, Feng FY, Wyatt A, Pienta KJ, Diehn M, Bentzen SM, Joniau S, Vanhaverbeke F, De Meerleer G, Antonarakis ES, Lotan TL, Berlin A, Siva S, Ost P, Tran PT. Long-Term Outcomes and Genetic Predictors of Response to Metastasis-Directed Therapy Versus Observation in Oligometastatic Prostate Cancer: Analysis of STOMP and ORIOLE Trials. J Clin Oncol. 2022 Oct 10;40(29):3377-3382. doi: 10.1200/JCO.22.00644. Epub 2022 Aug 24. PMID: 36001857; PMCID: PMC10166371.
- Marvaso G, Corrao G, Zaffaroni M, Vincini MG, Lorubbio C, Gandini S, Fodor C, Netti S, Zerini D, Luzzago S, Mistretta FA, Venetis K, Cursano G, Burla T, Mazzocco K, Cattani F, Petralia G, Fusco N, Pravettoni G, Musi G, De Cobelli O, Tang C, Ost P, Palma DA, Orecchia R, Jereczek-Fossa BA. ADT with SBRT versus SBRT alone for hormone-sensitive oligorecurrent prostate cancer (RADIOSA): a randomised, open-label, phase 2 clinical trial. Lancet Oncol. 2025 Mar;26(3):300-311. doi: 10.1016/S1470-2045(24)00730-7. PMID: 40049196.
- Francolini G, Bertini N, Di Cataldo V, Garlatti P, Aquilano M, Caini S, Bruni A, Ingrosso G, D'angelillo RM, Tagliaferri L, Augugliaro M, Triggiani L, Parisi S, Timon G, Arcidiacono F, Marvaso G, Jereczek-Fossa BA, Lancia A, Franzese C, Alongi F, Simontacchi G, Greto D, Bonomo P, Loi M, Frosini G, Burchini L, Desideri I, Meattini I, Valicenti RK, Livi L. Impact of stereotactic body radiotherapy after progression in castrate resistant prostate cancer patients undergoing first line abiraterone treatment. A subgroup analysis from ARTO trial (NCT03449719). Prostate Cancer Prostatic Dis. 2025 Dec;28(4):908-912. doi: 10.1038/s41391-025-00950-3. Epub 2025 Feb 19. PMID: 39972049.
- Tang C, Sherry AD, Hwang H, Farris DP, Francolini G, Di Cataldo V, Livi L, Tran P, Corn PG, Aparicio A, Simontacchi G, Kiess AP, Wang JH, Fonteyne V, Bultijnck R, Phillips R, Deek MP, Olson R, Harrow S, Marvaso G, Lorubbio C, Jereczek-Fossa BA, Ludmir EB, Blanchard P, Warner A, Sun R, Palma DA, Ost P. Metastasis-directed therapy and standard of care versus standard of care for oligometastatic prostate cancer (WOLVERINE): a systematic review and individual patient data meta-analysis from the X-MET collaboration. Lancet Oncol. 2026 Feb;27(2):181-190. doi: 10.1016/S1470-2045(25)00658-8. PMID: 41643695.
- Nickols NG, Tsai S, Kane N, Tran S, Ghayouri L, Diaz-Perez S, Thein M, Anderson-Berman N, Eason J, Kishan AU, Steinberg ML, Reiter RE, Lee SP, Gin GE, Kwon R, Chang MG, Chao HH, Solanki AA, Sexton R, Lewis M, Lorentz W, Cheung MK, Gage DL, Duriseti S, Valle L, Berenji G, Aronson WJ, Garraway IP, Rettig MB. Systemic and Tumor-directed Therapy for Oligometastatic Prostate Cancer: The SOLAR Phase 2 Trial in De Novo Oligometastatic Prostate Cancer. Eur Urol. 2024 Aug;86(2):190-193. doi: 10.1016/j.eururo.2024.02.008. Epub 2024 Mar 14. PMID: 38490853; PMCID: PMC12363338.
- Juarez Casillas JE, Nikitas J, Rettig MB, Reiter RE, Lee A, Steinberg ML, Valle L, Kalbasi TR, Calais J, Czernin J, Eala MA, Tsai S, Kane N, Solanki AA, Sexton R, Duriseti S, Berenji GR, Aronson WJ, Garraway IP, Chang MG, Kwon R, Lee SP, Nickols NG, Kishan AU. Pooled Analysis of the SOLAR and SATURN Clinical Trials Comparing Progression of Synchronous Versus Metachronous Prostate-specific Membrane Antigen-defined Oligometastatic Prostate Cancer Following Systemic and Tumor-directed Therapy. Eur Urol Oncol. 2025 Aug;8(4):893-898. doi: 10.1016/j.euo.2025.05.027. Epub 2025 Jun 19. PMID: 40541485; PMCID: PMC12311854.
- Wang JH, Sherry AD, Bazyar S, Sutera P, Radwan N, Phillips RM, Deek MP, Lu J, Dipasquale S, Deville C, DeWeese TL, Song DY, Wang H, Hobbs RF, Malek R, Dudley SA, Greco SC, Antonarakis ES, Marshall CH, Denmeade S, Paller CJ, Carducci MA, Pienta KJ, Oz OK, Ramotar M, Leenstra JL, Park SS, Abramowitz MC, Desai N, Berlin A, Stish BJ, Tang C, Tran PT, Kiess AP. Outcomes of Radium-223 and Stereotactic Ablative Radiotherapy Versus Stereotactic Ablative Radiotherapy for Oligometastatic Prostate Cancers: The RAVENS Phase II Randomized Trial. J Clin Oncol. 2025 Jun 20;43(18):2059-2068. doi: 10.1200/JCO-25-00131. Epub 2025 May 7. PMID: 40334149; PMCID: PMC12169860.