(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured an advancement in metastatic castration resistant prostate cancer (mCRPC) therapy session and a presentation by Dr. Wei Chen discussing a reconstructed analysis of the PEACE-3 trial assessing the time-dependent survival benefit of enzalutamide + radium-223 in mCRPC.
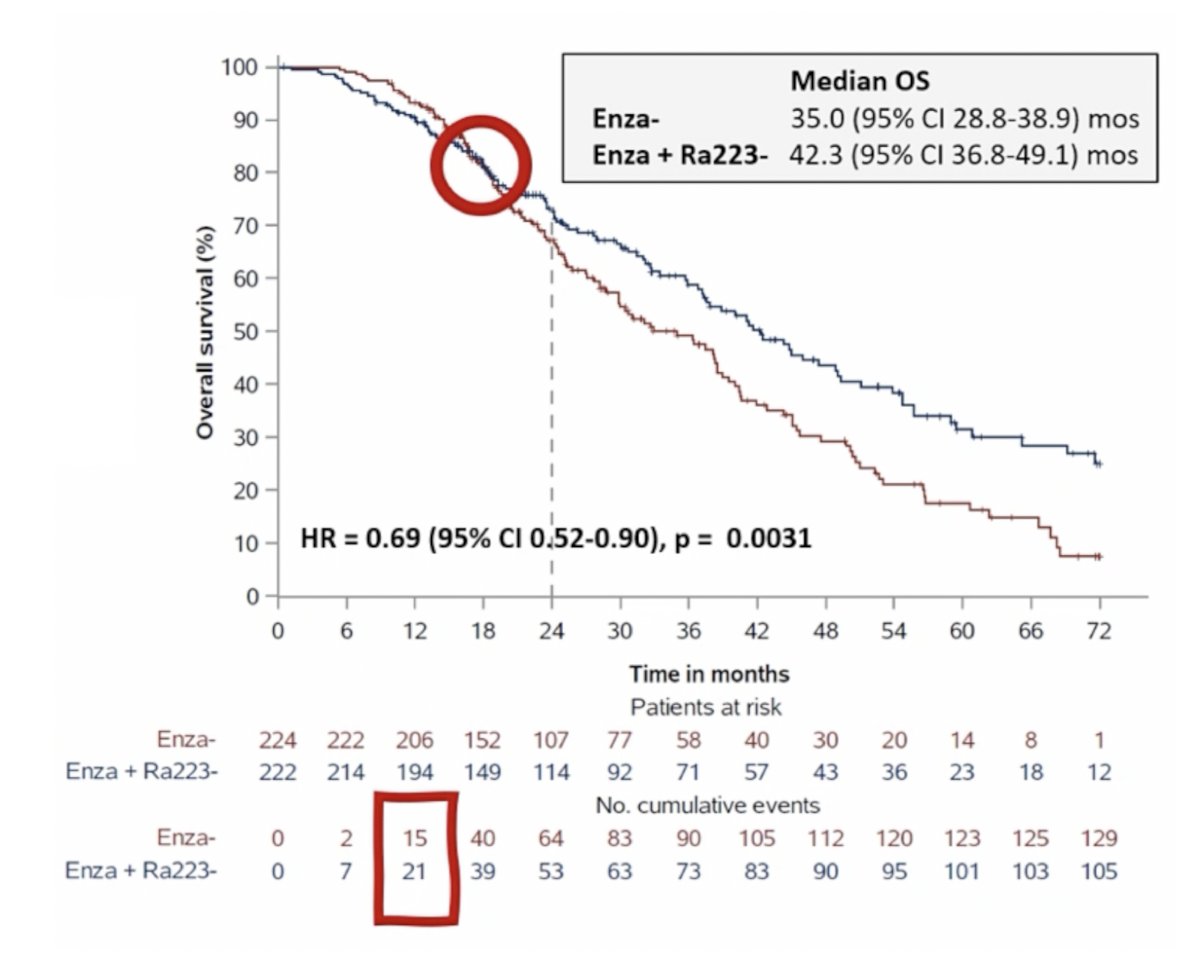
The PEACE-3 trial demonstrated improved overall survival for enzalutamide plus radium-223 versus enzalutamide alone in mCRPC,1 but the survival curves showed early crossover and later separation, suggesting non-proportional hazards:
Three key questions are outstanding:
- Is the treatment benefit time-dependent?
- Is there early harm followed by delayed benefit?
- When does the survival advantage truly emerge?
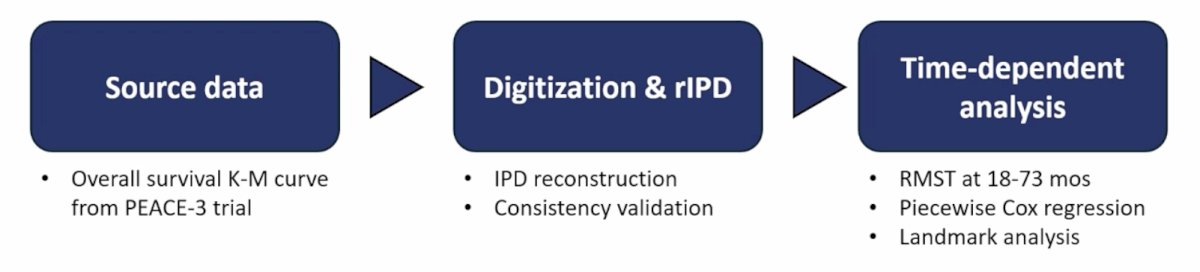
As such, Dr. Chen and colleagues aimed to characterize the time-dependent treatment effects using reconstructed individual patient data.
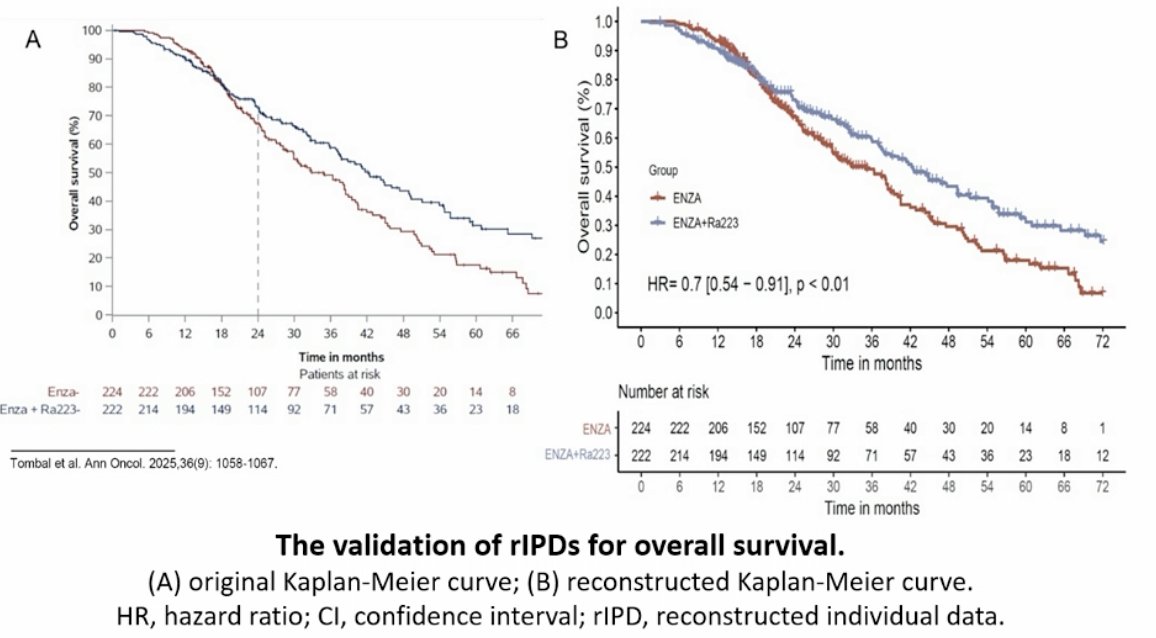
A total of 446 reconstructed individual patient data sets were generated from PEACE-3 using the individual patient data from the Kaplan-Meier algorithm. Consistency was validated by curve and hazard ratio concordance. Time-varying effects were evaluated using restricted mean survival time and restricted mean time lost analyses (18-72 months), time-dependent Cox regression with treatment-by-time interaction, piecewise Cox regression (6 intervals), landmark analyses, and Fleming-Harrington weighted log-rank tests:
The 446 individual patient data were reconstructed, and validation confirmed consistency with the original trial (consistency test: z = 0.04, p = 0.97):
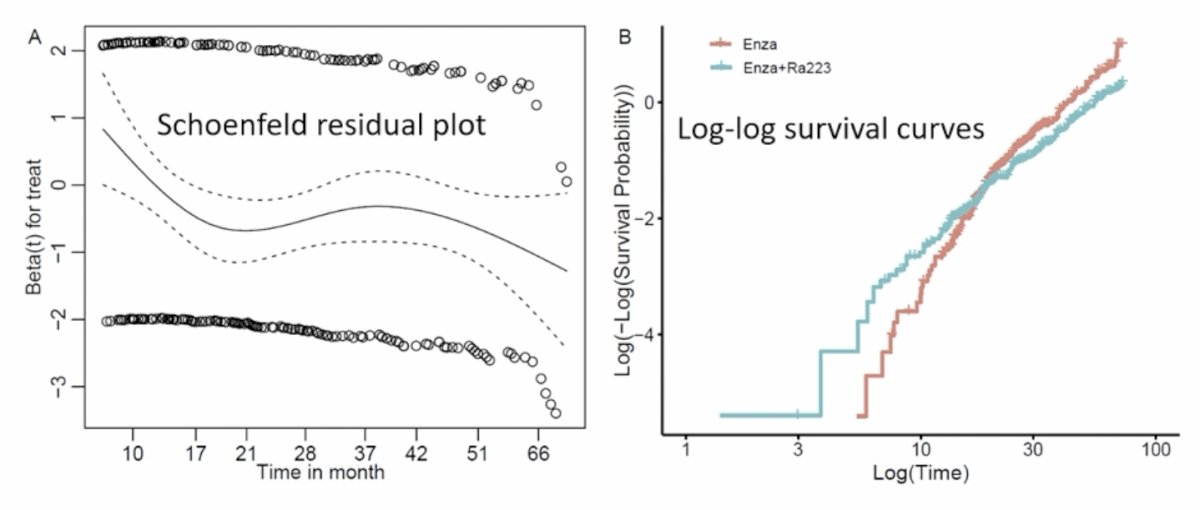
The proportional hazards assumption revealed significant violation (chi-squared = 5.01, p = 0.03), prompting the use of time-dependent, non-proportional hazards models in subsequent analyses:
During the initial 18 months, combination therapy showed no survival benefit (restricted mean survival time difference = -0.36 months, 95% CI -0.90 to 0.18, p = 0.20; HR 1.18, 95% CI 0.74-1.84, p = 0.48). The early mortality imbalance was driven by adverse events (ie. fractures and cardiovascular events), and thus, toxicity risk outweighed immediate gains. Between months 18-60, the biological efficacy of delayed overall survival benefit started to manifest after the initial increased risk:
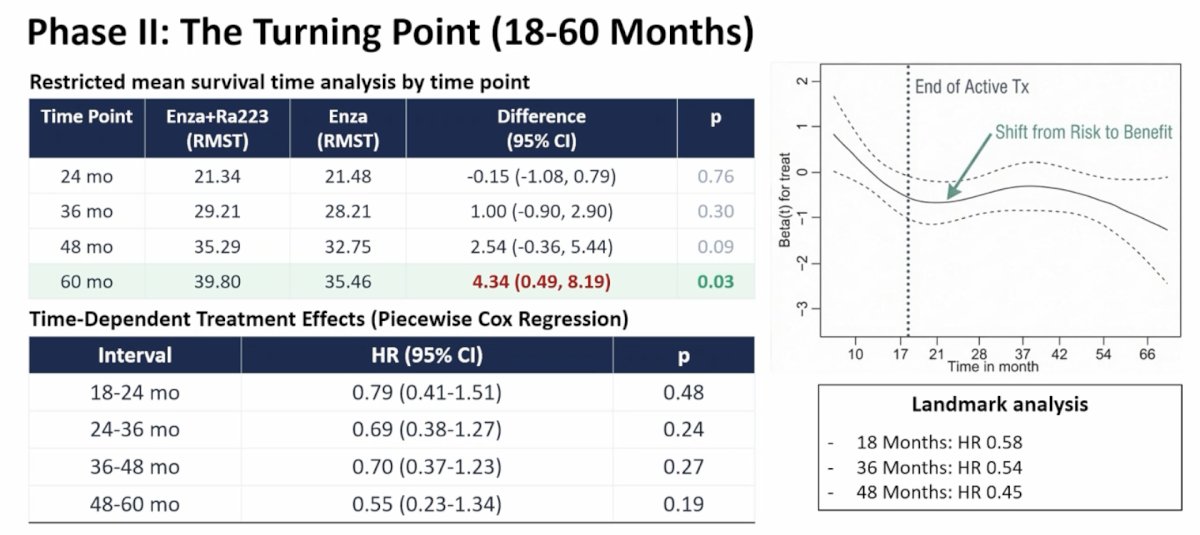
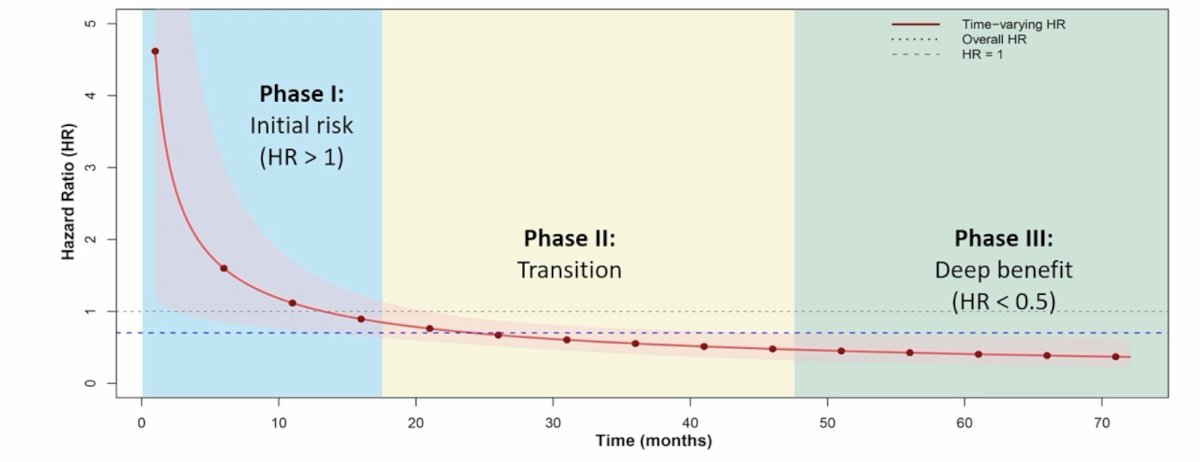
The survival advantage became significant after 60 months (restricted mean survival time difference = 4.34 months, 95% CI 0.49-8.19, p = 0.03) and further increased at 72 months (difference = 6.25 months, 95% CI 1.56-10.95, p = 0.01). Piecewise analysis revealed maximal benefits during 60-72 months (HR 0.20, 95% CI 0.05-0.77, p = 0.02). Thus, after 60+ months of observation, there was an 80% reduction in risk of death for long-term survivors. The following figure highlights the visualization of the time-varying hazard ratio shift:
Why the delayed benefit? Dr. Chen provided the following points:
- Radium-223 is not a rapid cytoreductive therapy, delivering targeted alpha-radiation to bone metastases via calcium-mimetic properties
- 6-month sequential therapy: the biological impact accumulates and becomes clinically visible months after completion
- Dual targeting may disrupt multiple resistance mechanisms over time
- Mandatory bone protective agents were instituted mid-trial, which significantly reduced fracture risk and may have contributed to long-term survival
These clinical implications include (i) patients needing sufficient life expectancy to benefit from the delayed effect, (ii) requires a long term perspective for both patients and their clinicians, (iii) full benefits may take several years to materialize, which impacts adherence counseling, and (iv) this supports enzalutamide + radium-223 consideration as a first line option for bone metastatic mCRPC with good prognosis.
Dr. Chen concluded his presentation discussing a reconstructed analysis of the PEACE-3 trial assessing the time-dependent survival benefit of enzalutamide + radium-223 in mCRPC with the following take-home points:
- Enzalutamide + radium-223 demonstrates a delayed but substantial survival benefit in mCRPC, becoming statistically significant after 60 months
- There is no survival advantage during the initial 18-month active treatment period (restricted mean survival time difference diff: -0.36 months, p = 0.20)
- There is a greater than 6-month survival advantage at 72 months (restricted mean survival time difference diff: +6.25 months, p = 0.01) with 80% death risk reduction in long-term survivors
- Non-proportional hazards analysis is essential for treatments with time-varying effects, as standard Cox may underestimate long-term benefit
- The final overall survival analysis of PEACE-3 is warranted and may reveal a more significant survival benefit
Presented by: Wei Chen, MD, MMed Institute of Science Tokyo, Tokyo, Japan
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
Reference: