(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a plenary prostate cancer session and a presentation by Dr. Wolfgang Fendler discussing the optimal management of oligorecurrent disease and whether there is a role for lutetium PSMA. Dr. Fendler’s discussion was based on a prior case presentation of a 61 year old fit man with oligo-recurrent prostate cancer after radical prostatectomy, with a PSA of 1.5 ng/mL (PSA doubling time: 3 months) and 3 PSMA positive pelvic lymph node metastases. There is evidence for PSMA radioligand therapy for oligorecurrent prostate cancer, and Dr. Fendler used his presentation to discuss these 3 trials.
First, the LUNAR phase II trial1 enrolled patients with recurrent oligometastatic hormone sensitive prostate cancer, characterized by 1-5 lesions outside the prostate or prostate bed on PSMA PET/CT. Patients were randomized in a 1:1 fashion to receive either stereotactic body radiotherapy to all metastatic lesions versus 2 cycles of neoadjuvant 177Lu-PSMA PNT2002 (6.8 GBq/cycles) 6-8 weeks apart, followed by stereotactic body radiotherapy to all metastatic lesions. Stratification was based on the number of lesions (1 versus 2-3 versus 4-5) and PSMA-based stage (N1/M1a versus M1b versus M1c):
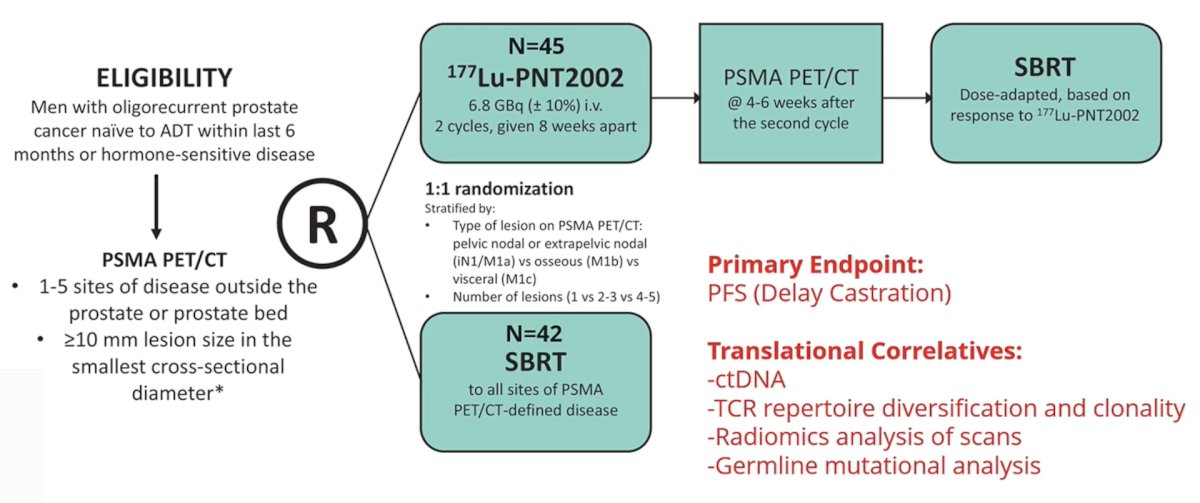
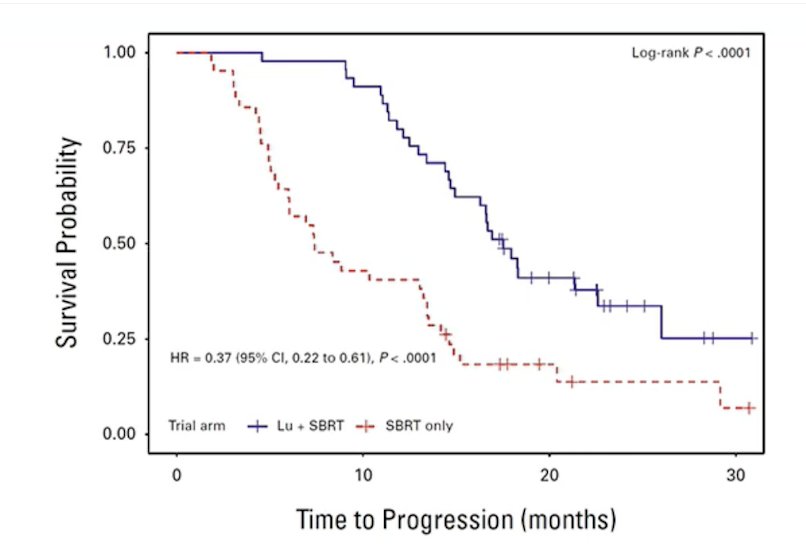
At a median follow-up of 20 months, the addition of 177Lu-PSMA to stereotactic body radiotherapy significantly improved median progression free survival from 7.4 months (95% CI 6.0-13.5 months) to 17.6 months (95% CI 15 months – not reached; HR 0.37, 95% CI 0.22-61):
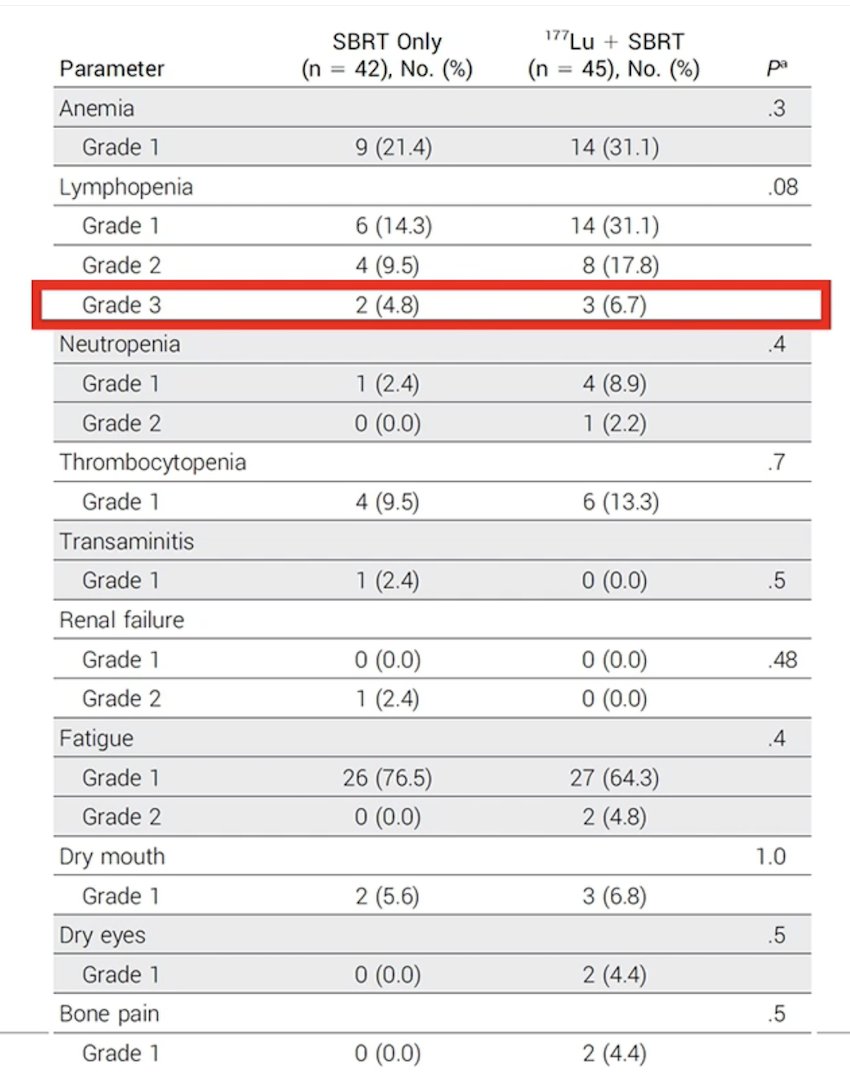
Importantly, there was a significant benefit for 177Lu-PSMA + stereotactic body radiotherapy for patients with N1-M1a (HR 0.2, 95% CI 0.08, 0.47) and patients with a lesion count of 2-3 (HR 0.32, 95% CI 0.15, 0.70). Grade 3 lymphopenia was seen in 7% and 5% of patients receiving 177Lu-PSMA + stereotactic body radiotherapy and stereotactic body radiotherapy, respectively, with no other grade 3 toxicities attributable to treatment:
Dr. Fendler notes that the addition of two cycles of 177Lu-PSMA before stereotactic body radiotherapy in patients with hormone sensitive prostate cancer improved progression free survival, and that this benefit of 177Lu-PSMA likely reflects activity against occult microscopic disease.
Second, the BULLSEYE trial was an international, multicenter, open-label, randomized phase II trial, randomizing 58 patients 1:1 to 177Lu-PSMA-617 versus standard of care of deferred ADT. Patients in the standard of care arm were allowed to receive 177Lu-PSMA-617 upon disease progression. Eligibility consisted of fast-progressing oligometastatic hormone sensitive prostate cancer following local treatment with ≤5 metastases. The primary outcome was progression free survival (ie, time without ADT). Secondary outcomes were PSA response, adverse events, quality of life, and outcomes observed in the control arm receiving 177Lu-PSMA-617. The trial design for BULLSEYE is as follows:
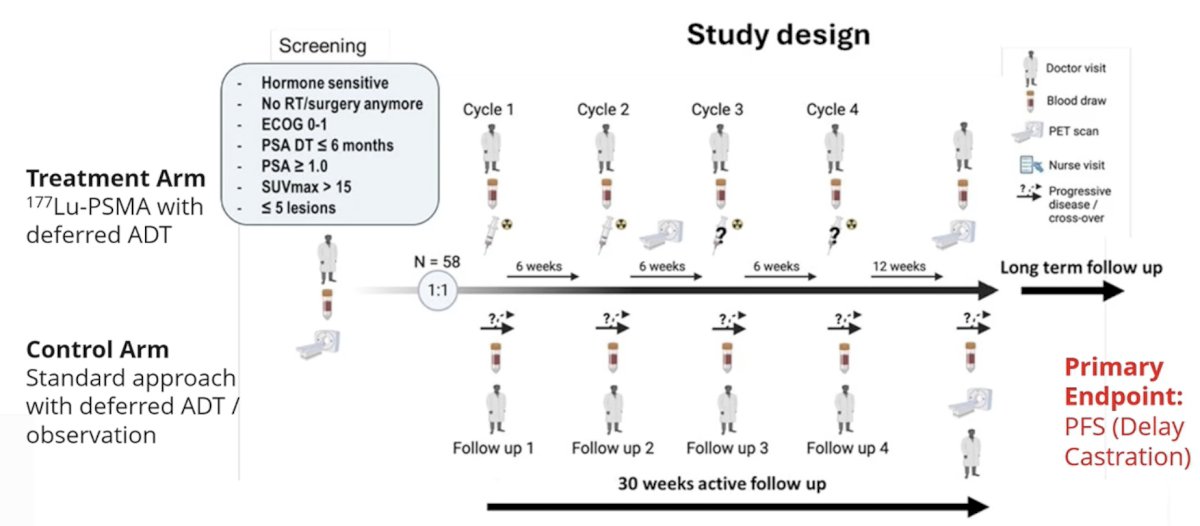
Patients received a median of 4 (IQR 4-4) cycles of 7.4GBq 177Lu-PSMA-617. During a median follow-up of 27 months (IQR 18-32), one standard of care arm patient (3%) remained without disease progression as compared to 14 (48%) patients in the 177Lu-PSMA-617 group. The median per protocol progression free survival was 5 (IQR 3-7) and 18 (IQR 10-28) months for the standard of care arm and 177Lu-PSMA-617, respectively (HR 0.07, 95% CI 0.03-0.17; p < 0.001):
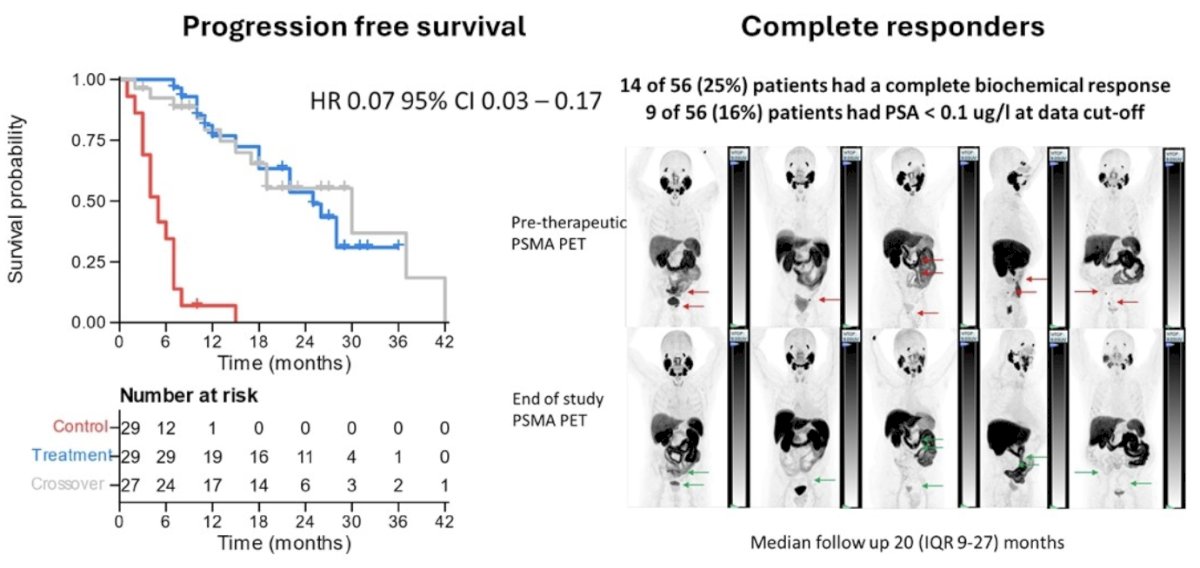
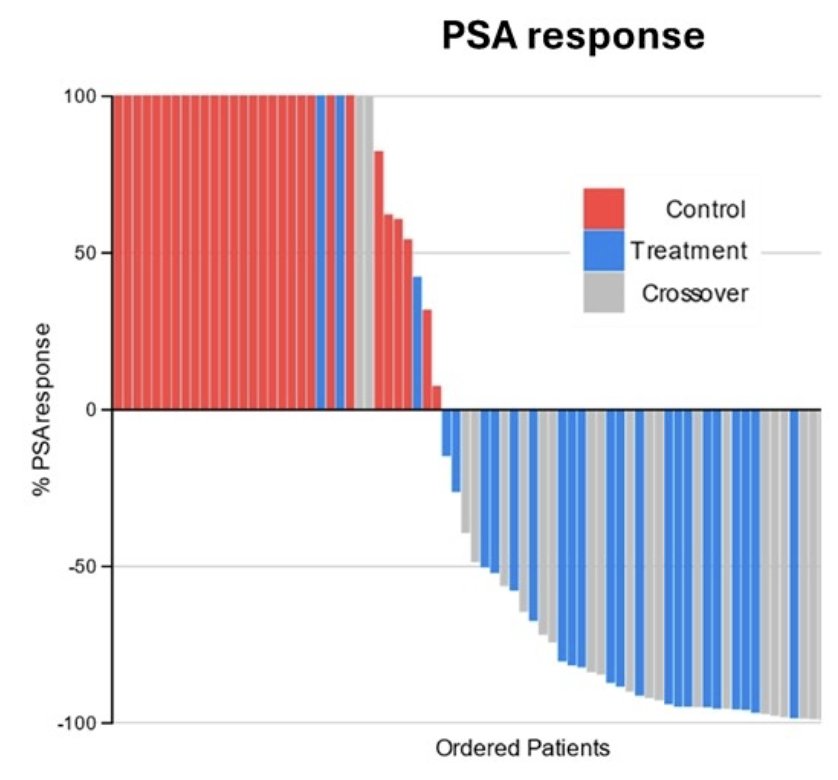
Overall, 31/56 of patients treated with 177Lu-PSMA-617 had a ≥90% PSA decline, and 14 had a complete biochemical response:
Dr. Fendler emphasized that BULLSEYE included a high-risk oligo-recurrent patient population with a PSA doubling time of <= 6 months, with 177Lu-PSMA resulting in:
- PSA90 in >50% of patients, and 25% had a complete biochemical response
- Postponing castration for 25 months in 50% of patients
- Well tolerated
Third, Dr. Fendler discussed the PSMA-DC trial in progress. Patients (n = ~450) in PSMA-DC will be randomized 2:1 to 177Lu-PSMA-617 or observation and will receive stereotactic body radiation therapy to all metastatic lesions within 14 days, completed within 3 weeks. Patients will then receive either IV 177Lu-PSMA-617 (7.4 GBq/6 weeks; 4 cycles), starting 7–21 days after stereotactic body radiation therapy, or undergo observation only. Additional stereotactic body radiation therapy for new lesions is allowed. ADT is allowed after a metastasis free survival event by conventional imaging confirmed by a blinded independent review committee. The trial design for PSMA-DC is as follows:
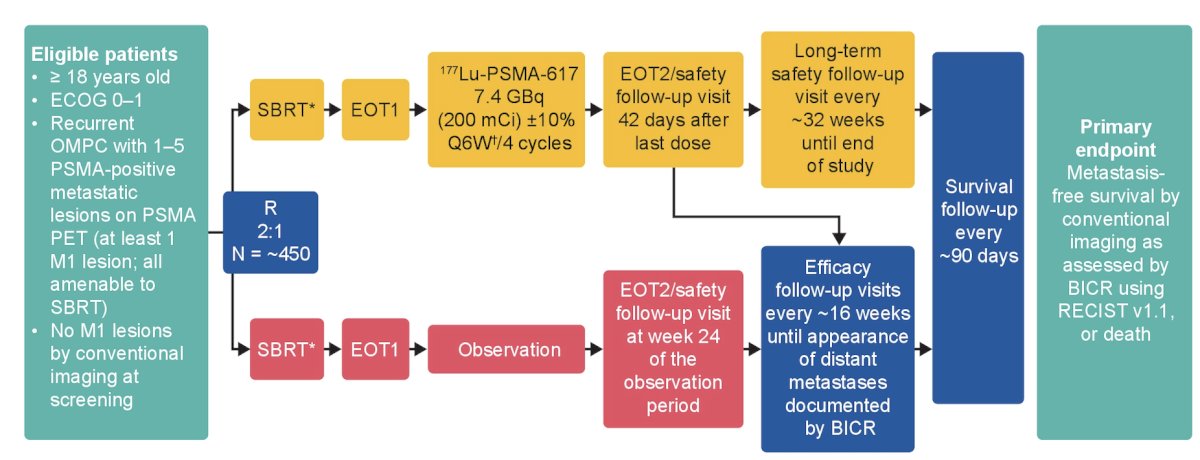
The primary endpoint is metastasis free survival by conventional imaging as assessed by a blinded independent review committee using RECIST v1.1, or death. The key secondary endpoint is time to next hormonal therapy, and additional secondary endpoints include time to PSA progression, radiographic progression-free survival, symptomatic progression, patient-reported health-related quality of life, overall survival, and safety.
Dr. Fendler concluded his presentation discussing the optimal management of oligorecurrent disease and whether there is a role for lutetium PSMA with the following take-home points:
- What we know:
- Can we offer PSMA radioligand therapy for nodal oligo-recurrence?
- No, it is not yet ready for primetime
- We need phase 3 data and await results from PSMA-DC
- We also need metastasis free and overall survival outcomes (PSMA-DC)
- Long term safety is required (LUNAR, BULLSEYE, PSMA-DC)
- The question remains whether radioligand therapy in this disease space is cost effective
Presented by: Wolfgang Fendler, MD, University of Duisburg-Essen, Essen, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References: