(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a plenary prostate cancer session and a presentation by Dr. Henk van der Poel discussing the optimal management of oligorecurrent disease, which is to use radioguided surgery to take out all oligorecurrent lesions. Dr. van der Poel’s discussion was based on a prior case presentation of a 61 year old fit man with oligo-recurrent prostate cancer after radical prostatectomy, with a PSA of 1.5 ng/mL (PSA doubling time: 3 months) and 3 PSMA positive pelvic lymph node metastases. Dr. van der Poel notes that in the Netherlands, this patient has an additional 23 years of life expectancy, and with N+ recurrence, he has a 74% 10 year overall survival, and 88% 10 year disease specific survival, thus treatment should be recommended for this patient. This patient has several treatment options, including (i) pelvic radiotherapy + hormone therapy, (ii) metastasis directed radiotherapy, (iii) long term hormonal therapy, and (iv) surgical lymph node removal.
EMBARK1 previously demonstrated an overall survival benefit (HR 0.60) of early leuprolide + enzalutamide for those with a N0M0 biochemical recurrence on conventional imaging and a median PSA of 5.0 ng/mL. However, there is toxicity associated with treatment, given that 87% of patients in EMBARK had drug related toxicity, 27.5% stopped treatment, and 8.5% had a drug related serious adverse event. Notably, toxicity tended to be higher in younger men (88.5% versus 83.6%).
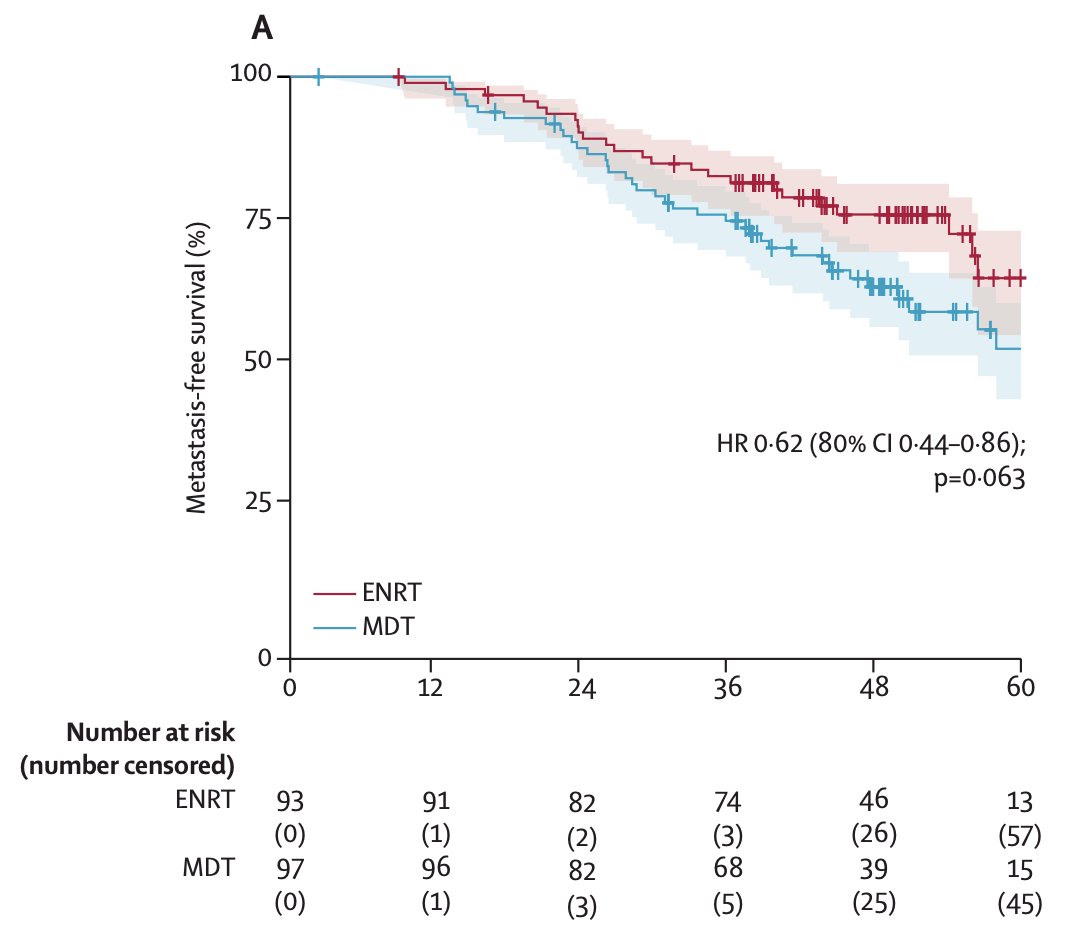
In the PEACE-V/STORM trial,2 the aim was to assess whether elective nodal radiotherapy to the pelvis would be superior to metastasis directed therapy. Among 190 evaluable patients (metastasis directed therapy n = 97; elective nodal radiotherapy n = 93), over a median follow up of 50 months (IQR 42-58), the 4-year metastasis free survival was 63% (80% CI 56-69) in the metastasis directed therapy group and 76% (80% CI 69-81) in the elective nodal radiotherapy group (HR 0.62, 80% CI 0.44-0.86; p = 0.063):
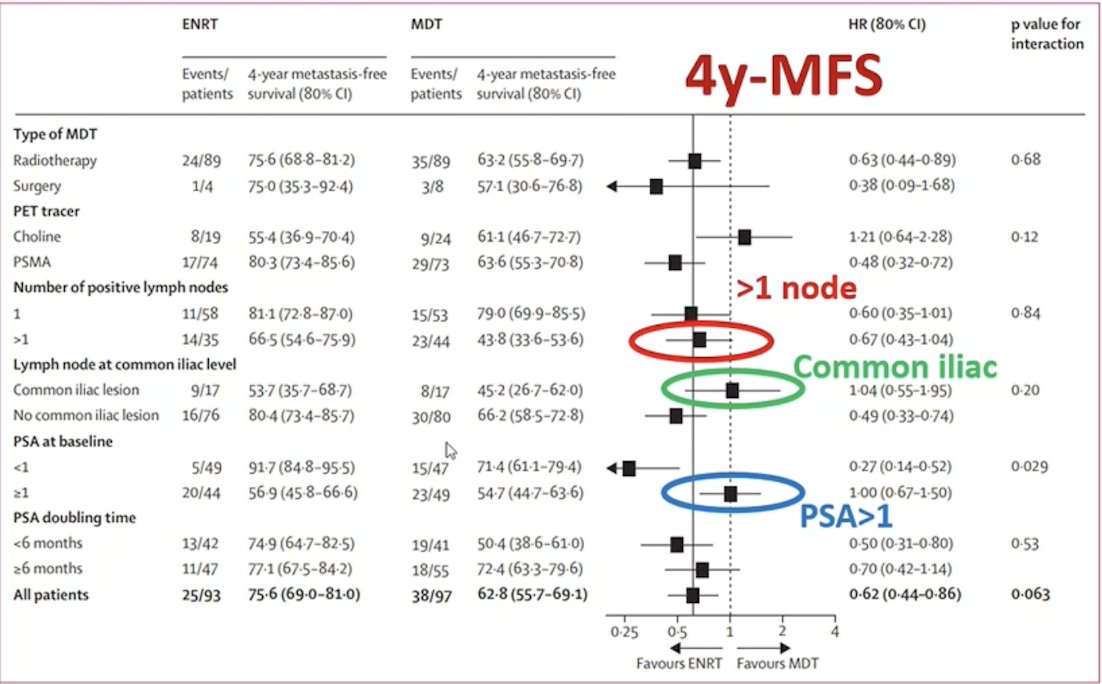
Dr. van der Poel notes that, based on the PEACE V/STORM data, for patients with >1 lymph node, common iliac nodes, and PSA >1 (like the current patient has), elective nodal radiotherapy does not work well:
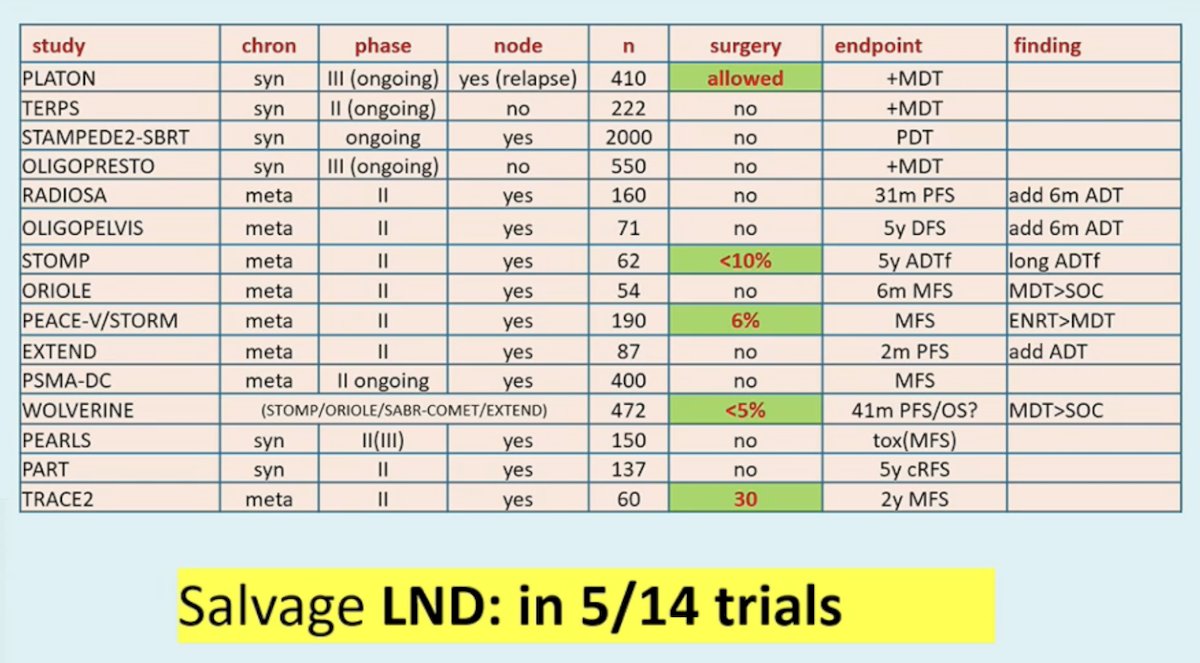
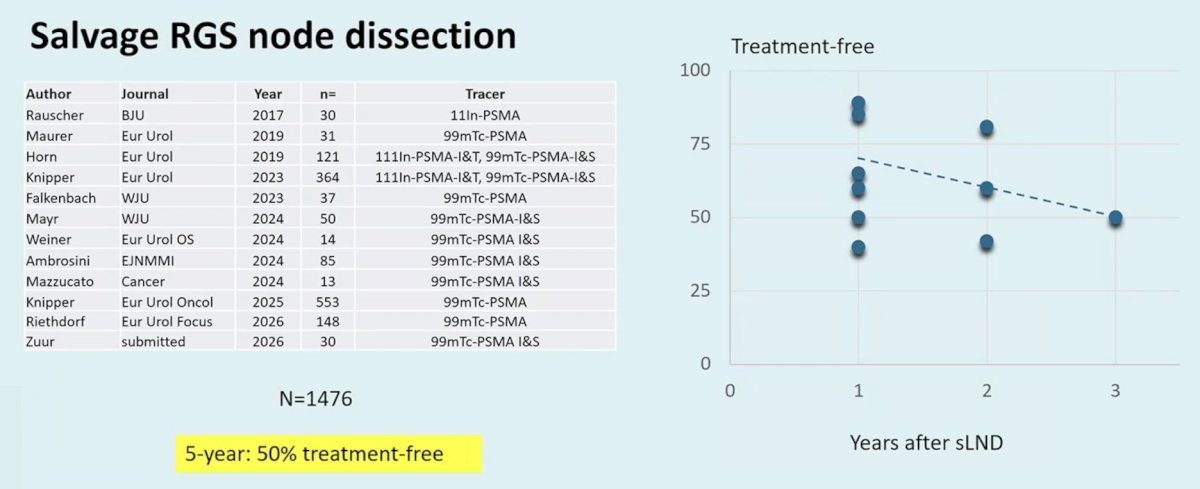
Dr. van der Poel emphasized that there is data for salvage lymph node dissection (5/14 trials), but admittedly, the data is not the strongest:
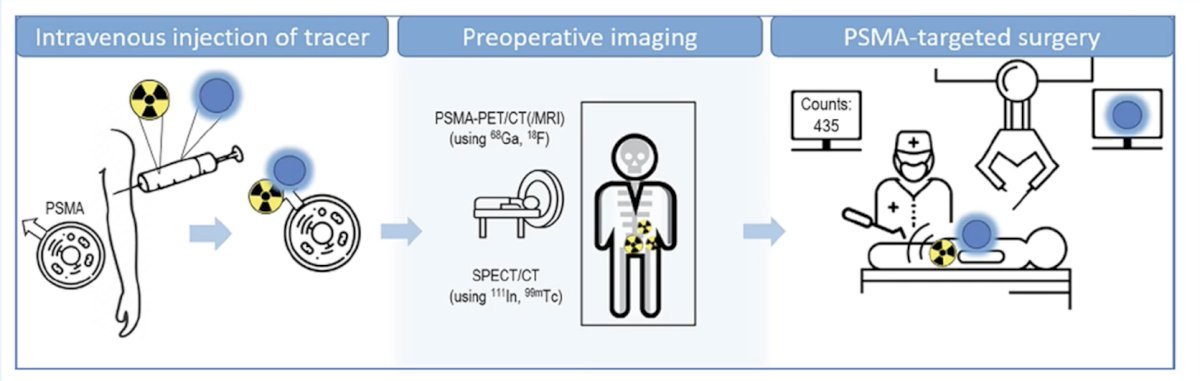
Therefore, PSMA targeting offers an opportunity to appropriately select patients who may benefit from surgery:
Compiling the available data, Dr. van der Poel suggests that for salvage radioguided surgery for nodal dissection (n = 1,476), the 5 year treatment free survival rates are ~50%:
In 2025, Bravi et al.3 published results assessing oncologic outcomes of template versus radioguided salvage lymph node dissection for node-only recurrent prostate cancer on PSMA PET scan. Overall, 80 (31%) and 179 (69%) patients received template and radioguided salvage lymph node dissection, respectively. They found that the first postoperative PSA level was higher in the template than in the radioguided group (median: 0.5 vs 0.1 ng/ml; p < 0.0001). Additionally, the 2-year biochemical recurrence free survival rate for patients in the template versus radioguided salvage lymph node dissection group was 18% (95% CI 9%, 29%) versus 30% (95% CI 22%, 37%), and the 2-year clinical recurrence-free survival rate for the template versus radioguided salvage lymph node dissection group was 51% (95% CI 35%, 65%) versus 73% (95% CI 65%, 80%):
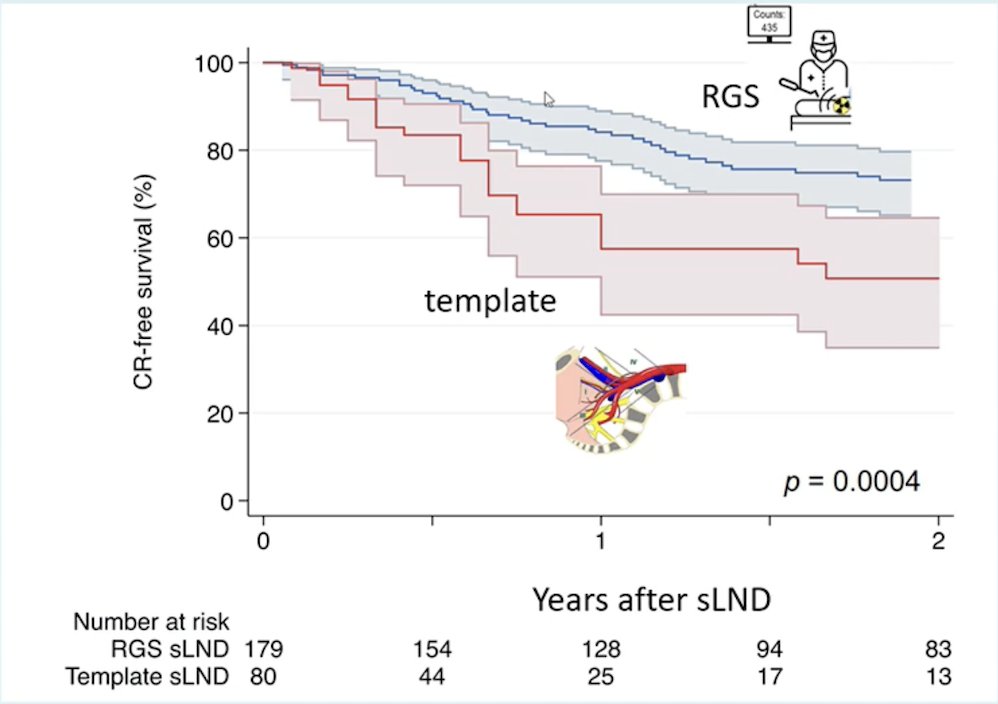
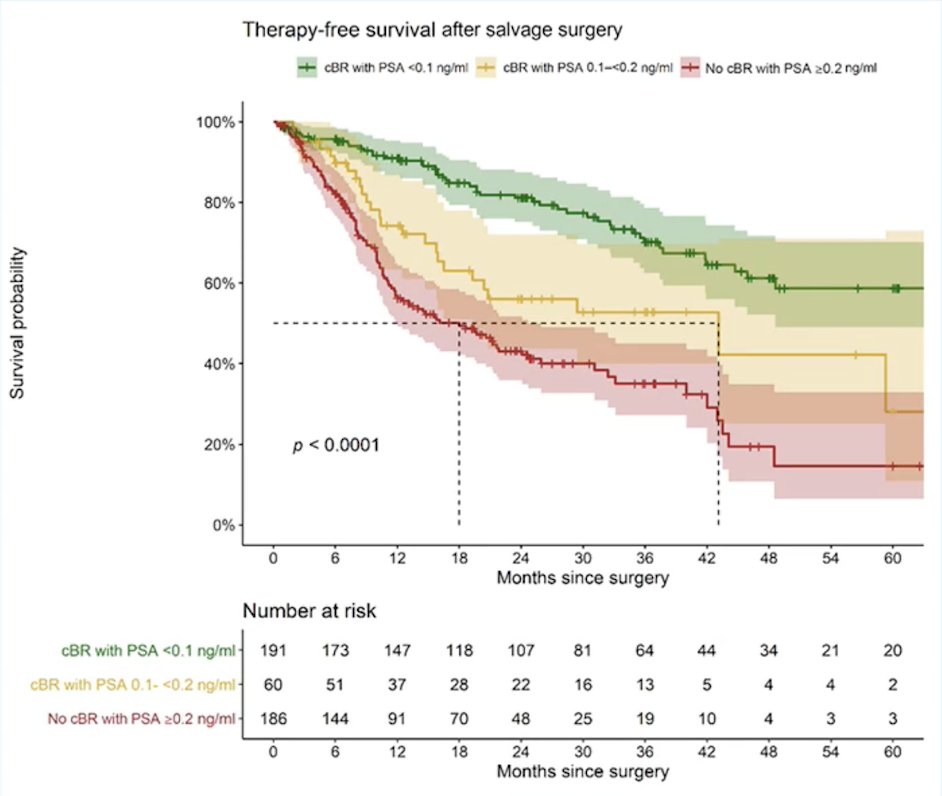
Thus, radioguided salvage lymph node dissection improved outcomes over a template lymph node dissection, highlighting the need for PSMA PET guided surgery in these situations. Knipper et al.4 also established that a biochemical response of <0.1 ng/mL predicts therapy free survival of prostate cancer patients following PSMA-targeted salvage therapy (n = 522). For patients with a post-therapy PSA <0.1 ng/mL, the treatment free rate at 5 years was 60%:
Side effects of salvage lymph node dissection are generally manageable, with low rates of colostomy reported and minimal impact on quality of life 6 months after treatment.
Dr. van der Poel concluded his presentation discussing the optimal management of oligorecurrent disease by emphasizing that lymph node removal avoids early hormone therapy, but allows radiotherapy and/or hormonal therapy to be used later in the disease process, if needed.
Presented by: Henk van der Poel, MD, PhD, Amsterdam, The Netherlands
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Freedland SJ, de Almeida Luz M, De Giorgi U, et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med 2023 Oct 19;389(16):1453-1465.
- Ost P, Siva S, Brabrand S, et al. Salvage metastasis-directed therapy versus elective nodal radiotherapy for oligorecurrent nodal prostate cancer metastases (PEACE V-STORM): A phase 2, open-label, randomized controlled trial. Lancet Oncol. 2025 Jun;26(6):695-706.
- Bravi CA, Knipper S, Heidenreich A, et al. Oncologic outcomes of template versus radioguided salvage lymph node dissection for node-only recurrent prostate cancer on prostate-specific membrane antigen positron emission tomography scan: Results from a multi-institutional collaboration. Eur Urol Focus. 2025 Nov;11(6):921-925.
- Knipper S, Lischewski F, Koehler D, et al. Biochemical response of <0.1 ng/mL predicts therapy free survival of prostate cancer patients following prostate-specific membrane antigen-targeted salvage therapy. Eur Urol Oncol. 2025 Apr;8(2):270-277.