(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a plenary prostate cancer session and a state-of-the-art lecture by Dr. Barbara A. Jereczek-Fossa discussing who can really benefit from metastasis-directed therapy. When discussing oligorecurrent prostate cancer, what we are treating is:
- Biochemical recurrence after primary treatment
- Limited metastases (commonly <=3-5 lesions)
- Lesions detectable mainly by PSMA PET
- Often low tumor burden, hormone-sensitive patients
However, the key issue is: is there a window of opportunity for treatment, or is this an early systemic disease? Dr. Jereczek-Fossa notes that the biological rationale for metastasis-directed therapy is to (i) eradicate visible disease burden, (ii) delay systemic therapy, and (iii) postpone castration resistance. The concept being that we intervene early, before widespread dissemination, given the low toxicity, low cost, and low impact on quality of life of metastasis-directed therapy.
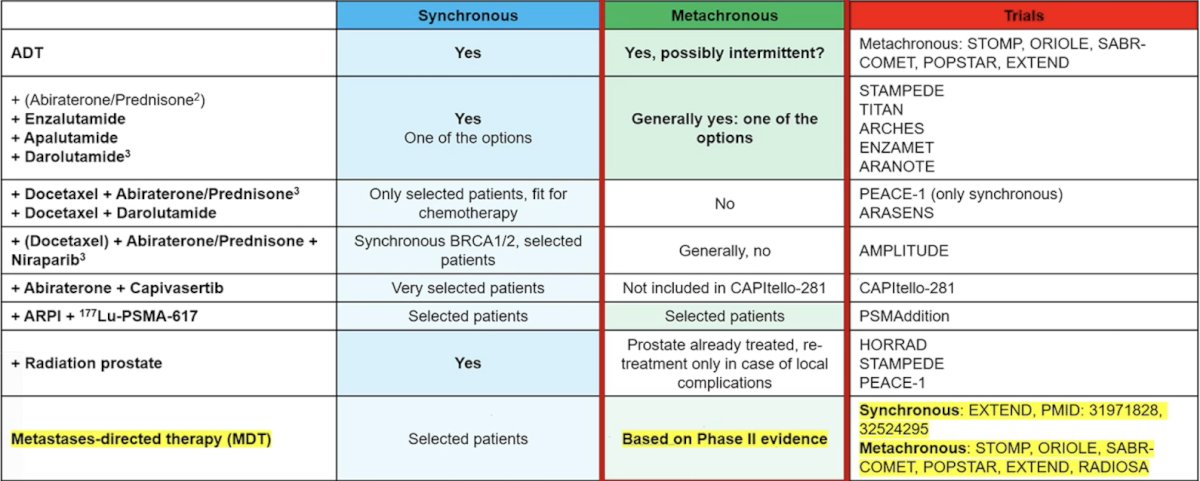
Should metastasis-directed therapy be performed alone or in combination? Should it be used to delay intensification or used as part of treatment intensification? Dr. Jereczek-Fossa notes that metastasis-directed therapy alone may delay ADT, although there is increasing data for metastasis-directed therapy with a short course of ADT. Currently, the role of systemic intensification is under investigation, and multidisciplinary decision-making is essential. The following table highlights treatment options in low-volume mHSPC:
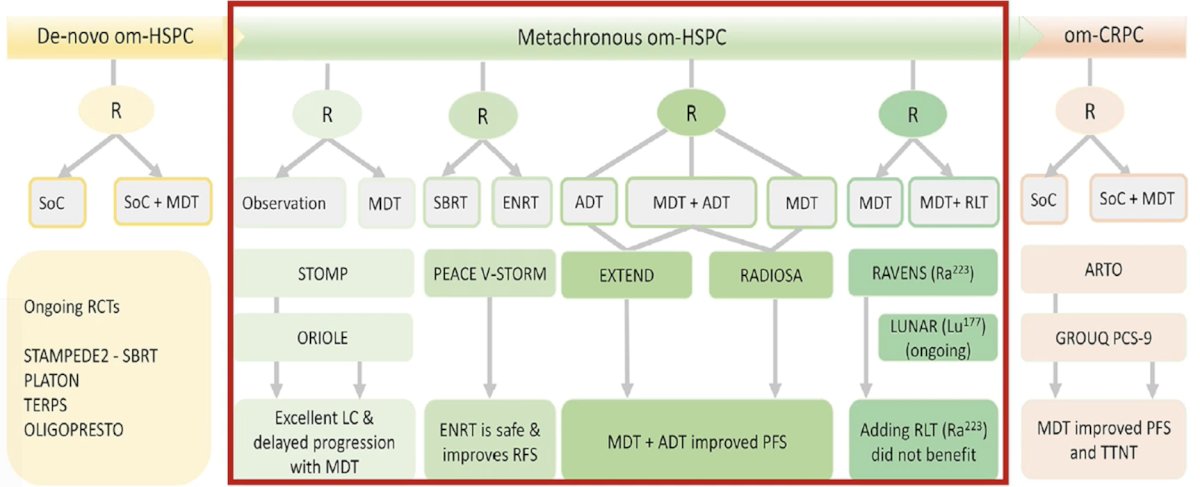
Moreover, the following table highlights the evidence from randomized trials for metastasis-directed therapy for oligorecurrent hormone-sensitive prostate cancer:
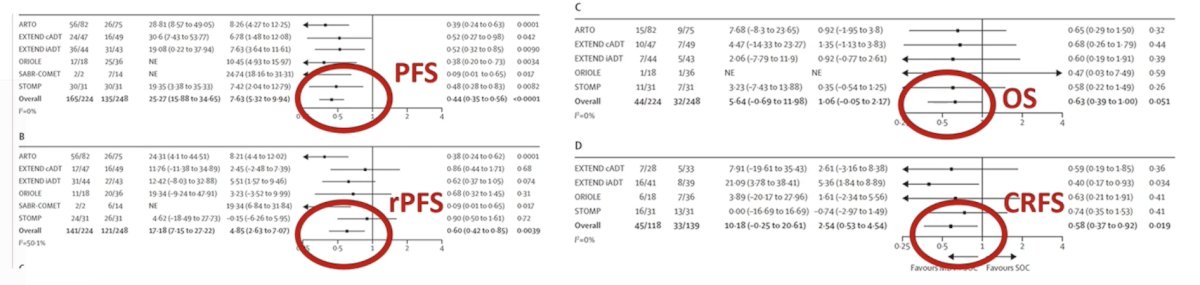
The WOLVERINE meta-analysis was published in early 20261 and amalgamated individual patient data across trials to evaluate the effectiveness of metastasis-directed therapy for oligometastatic prostate cancer. Overall, 7 phase 2 trials (n = 574) were included in the analysis. There were 6 trials randomly assigning 472 patients to metastasis-directed therapy + standard of care (n = 248) versus standard of care (n = 224) used to evaluate metastasis-directed therapy, and had a median follow-up time of 40.7 months (IQR 25.6-53.7). Metastasis directed therapy was associated with improved progression free survival (trial level HR 0.44, 95% CI 0.35-0.56, p < 0.0001; patient level HR 0.45, 95% CI 0.35-0.57, p < 0.0001), radiographic progression free survival (trial level HR 0.60, 95% CI 0.42-0.85, p = 0.0039; patient level HR 0.59, 95% CI 0.46-0.76, p < 0.0001), and castration resistance free survival (trial level HR 0.58, 95% CI 0.37-0.92, p = 0.019; patient level HR 0.58, 95% CI 0.37-0.91, p = 0.017). The association between metastasis-directed therapy and overall survival showed an HR of 0.63 (95% CI 0.39-1.00, p = 0.051) in trial-level analyses and 0.64 (95% CI 0.40-1.01, p = 0.057) in patient-level analyses:
Ultimately, patient selection is crucial. Dr. Jereczek-Fossa notes that patients who are likely to be better candidates are those with:
- <=3-5 lesions
- Long PSA doubling time
- Hormone-sensitive disease
- No visceral metastases
- All lesions treatable
- PSMA-negative disease elsewhere
Less suitable patients are those with rapid PSA kinetics, multiple nodal chains, or those with early polymetastatic evolution. To assist with patient selection, the PORTAL nomogram2 was developed from 1,461 patients to properly select those for metastasis-directed therapy and deferment of ADT. Key factors in the nomogram include (i) the total number of lesions, (ii) PSA doubling time pre-stereotactic body radiotherapy, (iii) PSA pre-stereotactic body radiotherapy, and (iv) NM stage:
![Less suitable patients are those with rapid PSA kinetics, multiple nodal chains, or those with early polymetastatic evolution. To assist with patient selection, the PORTAL nomogram [2] was developed from 1,461 patients to properly select those for metastasis-directed therapy and deferment of ADT. Key factors in the nomogram include (i) the total number of lesions, (ii) PSA doubling time pre-stereotactic body radiotherapy, (iii) PSA pre-stereotactic body radiotherapy, and (iv) NM stage:](/images/com-doc-importer/252-eau-2026/eau-2026-state-of-the-art-lecture-who-can-really-benefit-from-metastasis-directed-therapies/image-3.jpg)
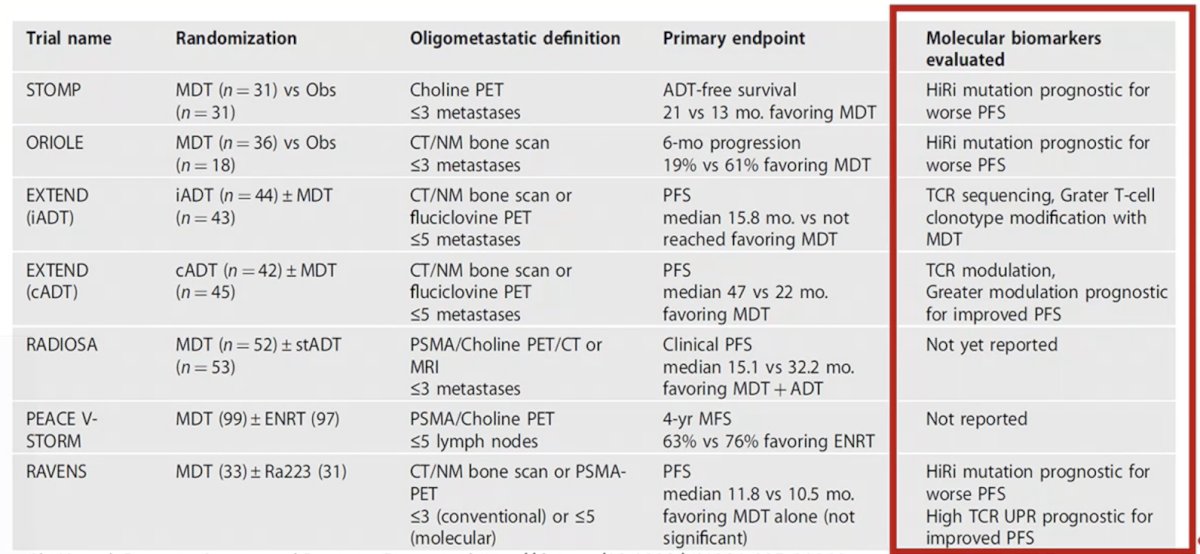
Who really benefits from metastasis-directed therapy depends on biology, highlighting the need for molecular biomarkers:
Dr. Jereczek-Fossa concluded her presentation discussing who can really benefit from metastasis-directed therapy with the following take-home points:
- Not all oligo-recurrences are equal; thus, selection matters
- Metastasis-directed therapy can reduce treatment burden
- The best candidates are:
- Low metastatic extent (<=3-5 lesions)
- All visible disease is amenable to metastasis-directed therapy
- Favorable biology and slow PSA kinetics
Presented by: Barbara Alicja Jereczek-Fossa, MD, PhD, Director, Division of Radiotherapy, European Institute of Oncology, Associate Professor in Radiation Oncology, University of Milan, Italy
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Tang C, Sherry AD, Hwang H, et al. Metastasis-directed therapy and standard of care versus standard of care for oligometastatic prostate cancer (WOLVERINE): A systematic review and individual patient data meta-analysis from the X-MET collaboration. Lancet Oncol. 2026 Feb;27(2):181-190.
- Soeterik TFW, Miszczyk M, Peters M, et al. Nomogram-based risk classification for predicting response to metastasis-directed stereotactic body radiotherapy in PSMA PET-staged oligorecurrent prostate cancer (PORTAL): An international retrospective cohort study. Lancet Oncol. 2026 Mar;27(3):383-392.