(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a plenary prostate cancer session and a state-of-the-art lecture by Dr. Bertrand Tombal discussing the road to cure and whether intensification matters.
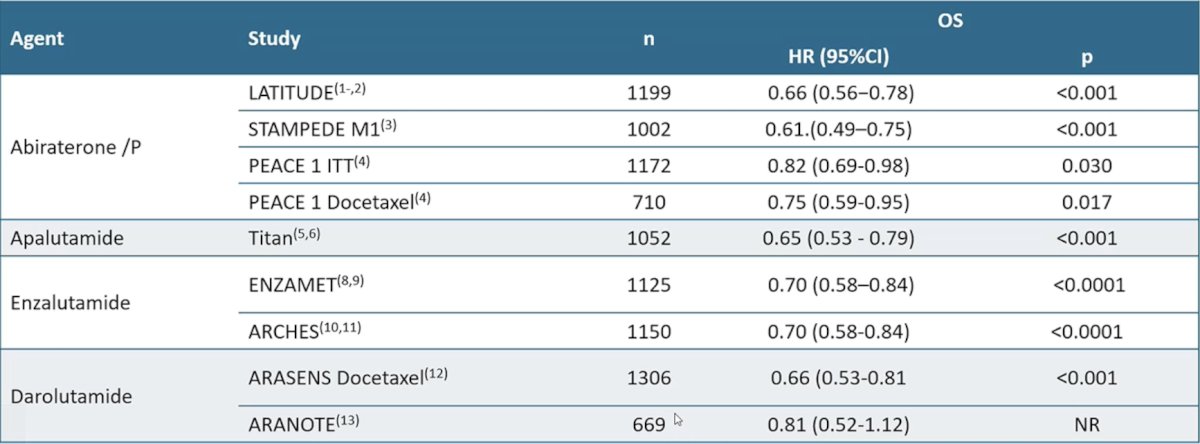
Dr. Tombal started by emphasizing that systemic intensification in oligorecurrent disease is reliant on whether oligo-progression is based on conventional imaging or based on modern imaging. For patients with oligo-progressive disease based on conventional imaging, these patients have low volume asynchronous prostate cancer, ADT + an androgen receptor pathway inhibitor is the standard of care. Early intensification of ADT + an androgen receptor pathway inhibitor has a very well-established track record with abiraterone + prednisone, apalutamide, enzalutamide, or darolutamide:
In 2026, Bin Riaz et al.1 published a living network meta-analysis assessing survival in mHSPC by volume of disease and timing of metastasis (11 trials, 12,668 patients, and 12 unique treatments). In the metachronous low volume subgroup (n = 775), androgen receptor pathway inhibitor + ADT led to a statistically significant improvement compared with ADT alone (HR 0.43, 95% CI 0.29-0.64) and docetaxel + ADT (HR 0.41, 95% CI 0.24-0.70). Furthermore, there was no statistically significant difference between androgen receptor pathway inhibitor + docetaxel + ADT and androgen receptor pathway inhibitor + ADT (HR 1.56, 95% CI 0.40-6.25):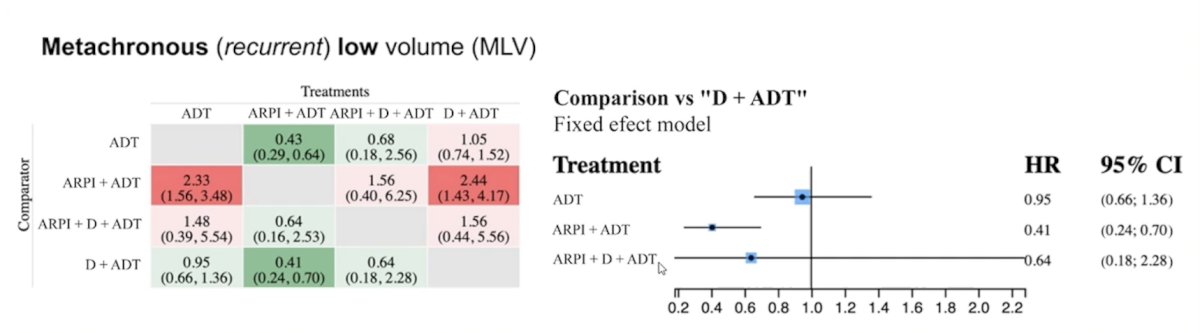
Dr. Tomball notes that from the APCCC 2024 conference, when experts were asked: “In the majority of patients with metachronous low-burden mHSPC on conventional imaging, what are your treatment recommendations?” 68% responded systemic therapy + metastasis-directed therapy, 22% systemic therapy alone, and 10% metastasis directed therapy alone. When asked, “If you recommend systemic therapy in a patient with metachronous low-burden mHSPC on conventional imaging, what type of systemic therapy do you recommend?” 91% stated ADT + androgen receptor pathway inhibitor, 8% ADT alone, and 1% androgen receptor pathway inhibitor alone.
Patients with oligo-progressive disease based on conventional imaging are also likely to be multi-metastatic on conventional imaging, and thus poor candidates for metastasis-directed therapy. At APCCC 2024, when experts were asked: “If you recommend metastasis-directed therapy in patients with metachronous low-burden mHSPC on conventional imaging, what do you recommend?” 88% responded they would treat only if no relevant additional and/or untreatable lesions are confirmed by next-generation imaging, and 12% that they would treat based on conventional imaging alone. There are several outstanding questions that remain:
- Are there exceptions?
- How long should the treatment be maintained?
- Is there a benefit from more intensification?
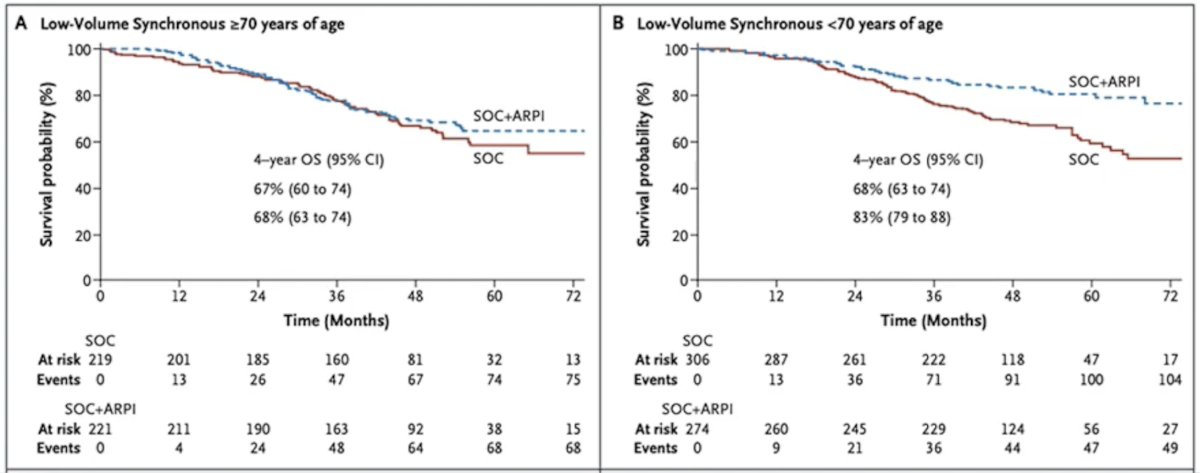
In 2025, Morgans and colleagues2 published an analysis assessing age and treatment intensification among patients with mHSPC (11 randomized comparisons, 13,648 patients). There were 8,324 young men and 5,162 older men included in the aggregate meta-analysis. Of note, individual patient data from three trials (TITAN, ARASENS, and LATITUDE) were used to validate the aggregative meta-analysis. Overall, treatment intensification was associated with improved overall survival (HR 0.73, 95% CI 0.68 to 0.78), and there was an interaction between age and treatment intensification on overall survival (p-interaction <0.001; younger men: HR 0.63, 95% CI 0.56 to 0.70; older men: HR 0.82, 95% CI 0.74 to 0.90). Notably, treatment intensification was not associated with improvement in overall survival in older men treated in trials utilizing predominantly triplet therapy (HR 0.94, 95% CI 0.77 to 1.14). For patients with low volume synchronous disease >= 70 years of age, there was no difference in overall survival between patients receiving standard of care + androgen receptor pathway inhibitor versus standard of care alone, whereas there was a benefit for standard of care + androgen receptor pathway inhibitor for patients < 70 years of age:
When APCCC 2024 experts were asked, “If you recommend systemic therapy in a patient with metachronous low-burden mHSPC on conventional imaging, what is your recommendation regarding systemic therapy?” 51% responded continuous lifelong treatment of ADT +/- androgen receptor pathway inhibitor or androgen receptor pathway inhibitor alone, 32% continuous treatment of ADT +/- androgen receptor pathway inhibitor or androgen receptor pathway inhibitor alone for 2-3 years, and 17% intermittent ADT +/- androgen receptor pathway inhibitor or androgen receptor pathway inhibitor alone (ie. interrupt after 6-12 months if PSA <0.2 ng/mL).
For patients with oligo-progressive disease on modern imaging, these patients pertain to the historical biochemical recurrence stage, and systemic intensification should be guided by the intrinsic risk of progression. Indeed, Dr. Tombal emphasized that not all biochemical recurrence is the same. However, based on the available evidence, there is limited benefit of ADT alone. Data from Moul et al. [3] assessing early versus delayed ADT for PSA only recurrence (<= 5 ng/mL) after radical prostatectomy showed no benefit amongst all patients (n = 1,352), but did show benefit among those patients with Gleason >7 disease and/or PSA doubling time <12 months:
![For patients with oligo-progressive disease on modern imaging, these patients pertain to the historical biochemical recurrence stage, and systemic intensification should be guided by the intrinsic risk of progression. Indeed, Dr. Tombal emphasized that not all biochemical recurrence is the same. However, based on the available evidence, there is limited benefit of ADT alone. Data from Moul et al. [3] assessing early versus delayed ADT for PSA only recurrence (<= 5 ng/mL) after radical prostatectomy showed no benefit amongst all patients (n = 1,352), but did show benefit among those patients with Gleason >7 disease and/or PSA doubling time <12 months:](/images/com-doc-importer/252-eau-2026/eau-2026-state-of-the-art-lecture-the-road-to-cure-does-intensification-matter/image-3.jpg)
Dr. Tombal also highlighted the TOAD trial, which assessed when to initiate ADT in patients with biochemical recurrence.4 This was a phase III randomized trial that randomized 293 men to immediate ADT vs deferred ADT (delay of at least 2 years). Over a median follow-up of 5 years, among patients with biochemical relapse, there was no significant difference in overall survival (HR 0.58, 95% CI 0.30-1.12, p = 0.10). After Cox regression, the unadjusted HR for overall survival for immediate versus delayed arm assignment was 0.55 (95% CI 0.30-1.00; p = 0.050):
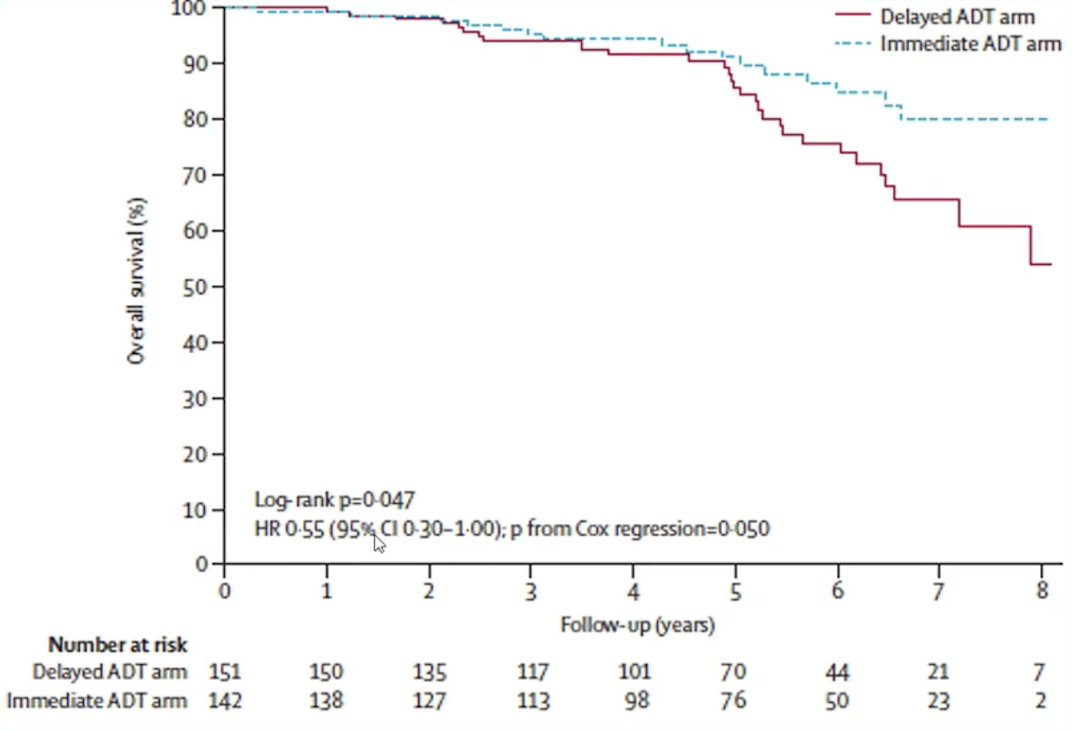
Based on the TOAD trial, survival may be prolonged with immediate treatment, but there is little gain for the first few years, and more than half of men with either strategy will still be alive after 8 years. For those opting to start treatment immediately, progression is delayed, but at a small cost in global quality of life.
In a 2022 systematic review of first-line treatment of recurrent prostate cancer after primary or salvage local therapy, Weiner et al.5 reported the following recommendations based on specific clinical questions:
![In a 2022 systematic review of first-line treatment of recurrent prostate cancer after primary or salvage local therapy, Weiner et al. [5] reported the following recommendations based on specific clinical questions:](/images/com-doc-importer/252-eau-2026/eau-2026-state-of-the-art-lecture-the-road-to-cure-does-intensification-matter/image-5.jpg)
For patients with oligo-progressive disease on modern imaging, low-risk biochemical recurrence (with or without oligometastases on new imaging modalities) should not receive systemic treatment. However, EMBARK6 reported improved outcomes and overall survival with enzalutamide in patients with high risk (PSA doubling time <= 9 months and PSA >= 1 ng/mL after radical prostatectomy +/- radiotherapy or >= 2 ng/mL after radiotherapy) biochemical recurrence:
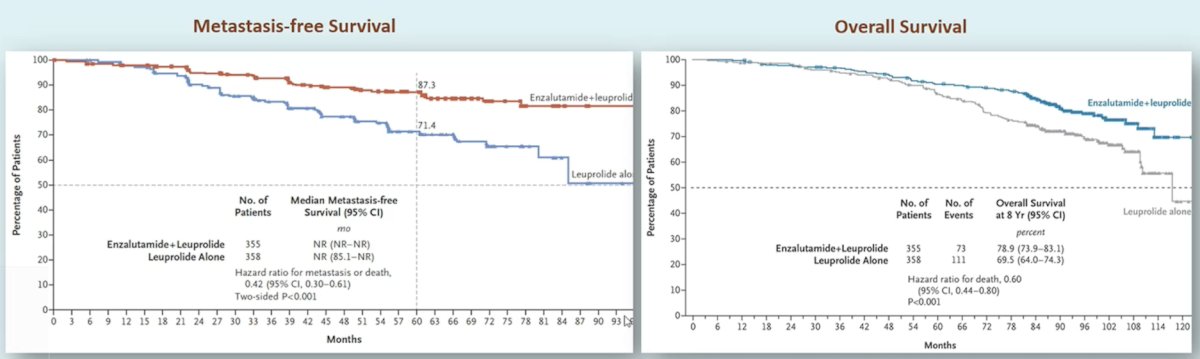
Thus, enzalutamide (and most likely other androgen receptor pathway inhibitors) significantly increase metastasis-free survival, alone or in combination with ADT, and overall survival in combination with ADT. The EAU guidelines make the following recommendations for systemic salvage treatment:
- Do not offer ADT to M0 patients with a PSA doubling time > 12 months (Strength: Strong)
- Offer enzalutamide with or without ADT to M0 patients with high-risk biochemical recurrence, defined as PSA doubling time <= 9 months and a PSA level of >= 2 ng/mL above nadir after radiation therapy or >= 1 ng/mL after radical prostatectomy with or without postoperative radiation therapy (Strength: Strong)
Dr. Tombal concluded his presentation discussing the road to a cure and whether intensification matters with the following take-home points:
- Oligo-progressive on conventional imaging: these patients have low-volume asynchronous prostate cancer, thus ADT + androgen receptor pathway inhibitor is the standard of care
- Oligo-progressive on modern imaging:
- Patients with otherwise low EAU risk biochemical recurrence will derive little benefit from systemic treatment
- Patients with otherwise high EAU risk biochemical recurrence should receive systemic treatment
- Patients with EMBARK characteristics should receive an androgen receptor pathway inhibitor
- Intermittent treatment should be recommended in PSA responders
Presented by: Bertrand Tombal, MD, PhD, Cliniques Universitaires Saint-Luc, Brussels, Belgium
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Bin Riaz I, Naqvi SAA, Faisal KS, et al. Comparative survival in metastatic hormone-sensitive prostate cancer by volume of disease and timing of metastasis: A living network meta-analysis. Eur Urol. 2026 Jan;89(1):31-44.
- Morgans AK, Roy S, Jia AY, et al. Age and treatment intensification in metastatic hormone-sensitive prostate cancer. NEJM Evid. 2025 Nov;4(11):EVIDoa2500109.
- Moul JW, Wu H, Sun L, et al. Early versus delayed hormonal therapy for prostate specific antigen only recurrence of prostate cancer after radical prostatectomy. J Urol. 2024 Mar;171(3):1141-1147.
- Duchesne GM, Woo HH, Bassett JK, et al. Timing of androgen-deprivation therapy in patients with prostate cancer with a rising PSA (TROG 03.06 and VCOG PR 01-03 [TOAD]): A randomized, multicentre, non-blinded, phase 3 trial. Lancet Oncol 2016;17(6):727-737.
- Weiner AB, Siebert AL, Fenton SE, et al. First-line systemic treatment of recurrent prostate cancer after primary or salvage local therapy: A systematic review of the literature. Eur Urol Oncol. 2022 Aug;5(4):377-387.
- Freedland SJ, de Almeida Luz M, De Giorgi U, et al. Improved Outcomes with Enzalutamide in Biochemically Recurrent Prostate Cancer. N Engl J Med 2023 Oct 19;389(16):1453-1465.